 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
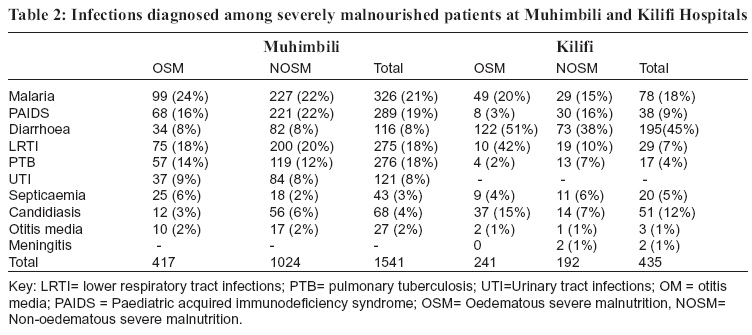
Tanzania Health Research Bulletin, Vol. 8, No. 3, 2006 pp. 189-192 Infections associated with severe malnutrition among hospitalised children in East Africa B. F.P. SUNGUYA1* , J.I. KOOLA2 and S. ATKINSON2 1Muhimbili University College of Health Sciences, P.O. Box 650001, Dar es Salaam, Tanzania 2Kenya Medical Research Centre, Wellcome Trust Research Collaboration Programme, Kilifi, Kenya * Correspondence: Dr. Bruno Sunguya; E-mail:sunguya@gmail.com Code Number: rb06036 Abstract: Severe protein-energy malnutrition (PEM) predisposes affected children to various infections, which either worsens their nutritional status or causes malnutrition, hence complicating their management and outcome. This study was carried out to determine the infections associated with severe malnutrition among children admitted at Kilifi District Hospital (KDH) in Kenya and Muhimbili National Hospital (MNH) in Dar es Salaam, Tanzania. Data was collected from hospital register books and online system database. A total of 1121 children with severe malnutrition were admitted during a period of one year (2004-2005) (MNH=781; KDH= 340). The proportion of male children with malnutrition was higher than that of female children. Non-oedematous malnutrition was more prevalent at MNH (N=504; 64%) than KDH (N=130; 38%). Conversely, oedematous was more prevalence than non-oedematous malnutrition among children admitted at KDH (N=210; 61.7%). More than 75% of all patients with severe PEM were children <2 years old. Thirty-six per cent of all severe PEM cases had malaria in both hospitals. Forty-five per cent of all admitted patients with severe PEM at KDH had diarrhoea. Two hundred twenty two (28%) and 64 (19%) of the children with severe malnutrition died at MNH and KDH, respectively. Oedematous PEM was associated with a higher case fatality rate than non-oedematous one (P<0.05). At MNH, 86% of the patients who died with severe malnutrition had other co-morbidities. More (46%) oedematous malnourished patients with co-infections died at MNH than non-oedematous malnourished patients (19%). At KDH, septicaemia was the leading cause of death (55%) among severely malnourished patients. In conclusion, coinfections complicate the management of severe malnutrition and are associated with higher death rate. Management of such infections is of paramount importance to reduce case fatality rates. Key words: Infections, malnutrition, children, hospital, Kenya, Tanzania Globally, malnutrition contributes to about 60% of the 11 million deaths that occur each year among children <4 years old (Berkley, 2002). Protein-energymalnutrition (PEM) is more common in developing countries among children <5 years old, the severe form being between 1-10% and underweight between 20-40%. Malnutrition has been associated with over half of all child deaths in developing countries (Stephenson et al., 2000). Severe malnutrition is defined as weight for height z-score <-3SD, bilateral oedema of kwashiorkor, or mid-upper arm circumference (MUAC) <11.0 cm (if >65 cm in length) (Berkley, 2002). Kwashiorkor occurs in infancy but maximally in the second year following abrupt weaning. Marasmus involves inadequate intake of protein and calories, representing the end result of starvation. It occurs in the first year of life due to lack of breast-feeding and use of dilute animal milk. Poverty and famine, ignorance and poor maternal nutrition are among the major contributory factors (Cederholm, 2002). Pre-school aged children in developing countries are often at risk of malnutrition because of their dependency on others for food, increased protein and energy requirements, and immature immune system causing greater susceptibility to infections. Severe malnutrition affects 1-2% of pre-school children mainly in the developing countries. In Tanzania, about 5% of the under fives are affected, marasmus being commoner than kwashiorkor in younger ages. In East Africa, malnutrition is increasing in prevalence and is a serious public health problem (Ngare & Muttunga, 1999; Ashworth et al., 2004). The ability of malnourished child to handle infections is lower. Common infections are those caused by Streptococcus pneumonia, Klebsiella pneumonia, Escherichia coli and Hemophilus influenza (Berkowitz, 2002). Malnutrition and infections are interrelated. This study was carried out to determine infections associated with severe malnutrition among children admitted to Kilifi District Hospital in Kenya and Muhimbili National Hospital in Tanzania. KDH is in Kilifi district on the coast of Kenya situated 60 km north of Mombassa. The district hospital serves a population of over 230,000 and the paediatric unit admits more than 5000 children per year. MNH in located in Dar es Salaam and is Tanzania’s national hospital, which also serves as the referral hospital for the eastern zone, which includes Dar es Salaam, Coast and Morogoro Regions. Data from paediatric wards at Kilifi District Hospital (KDH) in Kenya and Muhimbili National Hospital in Tanzania were collected from register books and online systeme database. In this study all severely malnourished children admitted at the two hospitals one-year (2004-2005) were included.’ In the two hospitals, PEM was clinically classified through the Wellcome Trust classification based on weight for age with or without oedema into the following grades; 80-60% without oedema as underweight; 80-60% with oedema- kwashiorkor; <60% with oedema-miasmic-kwashiorkor; <60% without oedema as marasmus (Taufan & Rampengan, 1991). There were 1121 patients admitted (MNH =69.7%; KDH=30.3%) with severe malnutrition for the duration of one year. Of 781 patients with severe malnutrition at MNH, 277 (35.5%) had oedematous severe malnutrition and 504 (64.5%) had nonoedematous severe malnutrition. At KDH, of the total 340 patients with severe malnutrition, 210 (61.8%) had oedematous and 130 (35.2%) non-oedematous type. Fifty-four percent of the patients admitted with severe malnutrition in both hospitals were male patients; More males (MNH=434; KDH= 182) than females (MNH=347; KDH= 158) were affected among the severely malnourished patients. Most of the severely malnourished children were in 1-2 years old age group. Children aged >4 years old were less affected by severe malnutrition (Table 1). Malaria was the leading co-morbidity with total prevalence of 21% at MNH among the admitted severely malnourished children. This was followed by HIV/AIDS, lower respiratory tract infection and pulmonary tuberculosis. At KDH, co-morbidity with diarrhoea was more prevalent (45%) than other infections. This was followed by malaria and candidiasis (Table 2). More than a quarter of severely malnourished children died during the period under review. High fatality rates were observed among children with oedematous type of severe malnutrition than in non-oedematous. A total of 222 (28%) and 64 (19%) of the children with severe malnutrition died at MNH and KDH, respectively. In both hospitals, more children were observed to suffer from Kwashiorkor (MNH=44%; KDH=23%) than from marasmus (MNH= 20%; KDH= 16%)(P<0.05). At MNH, of the 222 patients who died, 86% had comorbidities. More deaths were noted in patients with oedematous malnutrition and co morbidities than nonoedematous type. About 46% of oedematous patients with co-infections died compared to only 19% of nonoedematous patients with co-infections. At KDH, septicaemia was the most common cause of death followed by tuberculosis and HIV/AIDS. Mortality rates at KDH increased with age, with the highest rate of 42% and then decreased after the second year of life. Our findings indicate that severe malnutrition is a common condition among children admitted to hospitals in East Africa. In a different study, a prevalence of severe malnutrition of 16% at Kilifi was reported by Berkley (2002). The prevalence of the condition was similar in the two hospitals. Marasmus was found to be more prevalent at MNH (Isaac, 1990) than at KDH. Conversely, severe form of oedematous malnutrition was more prevalent at KDH than at MNH. It was also observed that boys were much more affected by severe malnutrition than girls in both hospitals. The reasons for this observation could not be established. More than half of the severely malnourished patients were in the age group of 1-2 year. This is likely to coincide with the time of weaning. These foods may not contain all the required nutrients supply especially protein and calories (PCC, 1988; Savva et al., 2005). It is also at this age that children are vulnerable to infections and helminths from contaminated environment or through eating of contaminated foods. The prevalence of severe malnutrition decreased among older children. Similar observations have been reported in previous studies (Brenton et al., 1967; Ashworth et al, 2004). Both kwashiorkor and marasmus peak at the age of 2 years due to the factors like weaning, infections, cultural and psychological factors (Savva et al., 2005; Taufan & Rampengan, 1991). Children with severe malnutrition are more prone to infections than others. This is due to nutritionally acquired immune dysfunctions syndrome, in which a child becomes immunocompromised and likely to suffer from bacterial, fungal and other infections (Isaac, 1990; Isaac et al., 1992; Stephenson et al., 2000). Ability of the malnourished child to handle infections is lower. At Muhimbili National Hospital, the majority of the patients with severe form of malnutrition had co-morbidities, with malaria been the most common co-infection. Malaria is likely to cause malnutrition when the child suffers recurrent infections leading to loss of appetite, nausea and vomiting. This situation limits the quantity of food that a child might take (Wafula et al., 1998). HIV causes immunosuppression; and may be associated with several other co-infections, which exacerbates malnutrition (Isaac et al., 1992). Lower Respiratory Tract Infections, tuberculosis and septicaemia are also prevalent in malnourished patients (Berkowitz, 1984; Isaac et al., 1992). Diarrhoea, which was the leading co-morbidity at KDH, causes malnutrition due to inadequate absorption and loss of nutrients and water. Higher mortality rates among severe malnutrition cases were recorded at MNH than KDH. High mortality rates were also observed in children with oedematous malnutrition than those without oedema in both hospitals. The high case fatality rate at MNH is most likely to be due to lack of guidelines on proper case management. KDH was observed to strictly follow WHO guide on management of severe malnutrition, with proper case management (WHO, 1999). Proper case management is expected to reduce mortality to less than 5% (WHO, 2002). The most common complications, which kill patients with severe malnutrition, include hypoglycaemia, hypothermia, infections, dehydration and electrolyte imbalance (WHO, 2002). Our findings indicate that co-infections were associated with majority of deaths among the malnourished children, particularly at Muhimbili Hospital. Oedema is known to cause congestive heart failure and pulmonary oedema (Ashworth et al., 2004). At Kilifi Hospital, most deaths were noted among patients with septicaemia. Deaths among patients with severe malnutrition have been attributed to bacteraemia (Berkowitz, 1984). The higher prevalence of severe malnutrition observed after the sixth month of life is mostly due to weaning and introduction of other staple foods. In conclusion, severe malnutrition is associated with infections and is common among children hospitalised in East Africa. Prompt and appropriate management of the coinfections is of paramount importance to reduce case fatality rates. References
Copyright 2006 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb06036t2.jpg] [rb06036t1.jpg] |
| |||||||||

{kind=link}
{kind=link}