 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
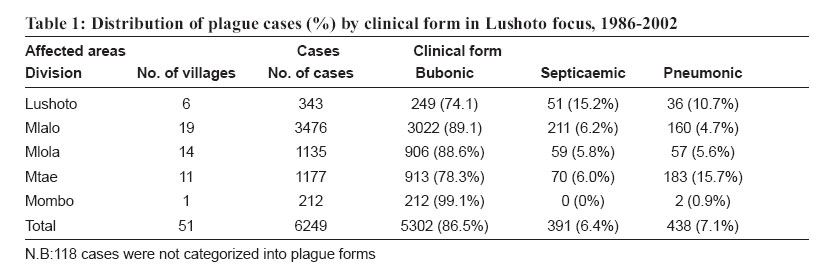
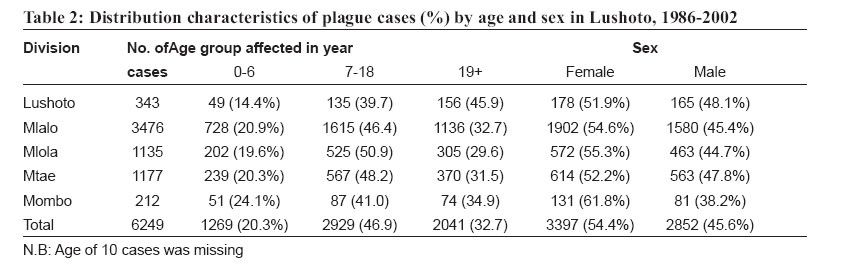
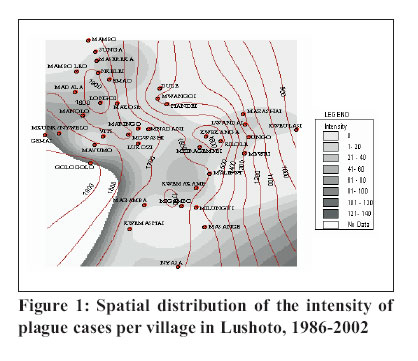
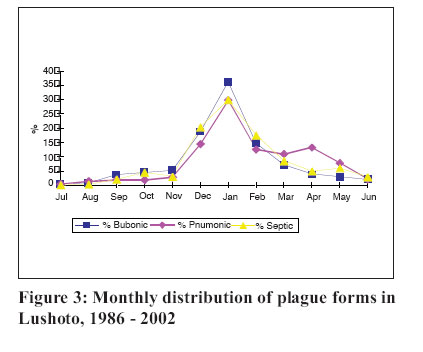
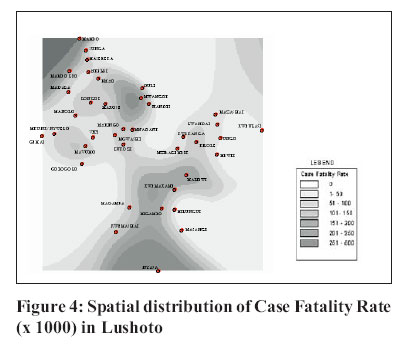
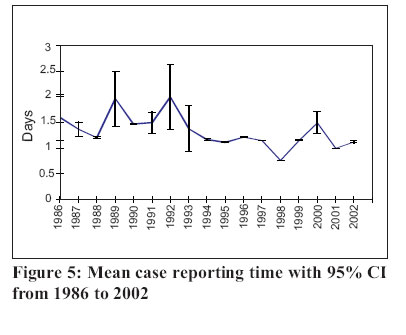
Tanzania Health Research Bulletin, Vol. 9, No. 1, 2007 pp. 12-17 Pattern and spatial distribution of plague in Lushoto, north-eastern Tanzania M.L. KAMUGISHA1*, S. GESASE1, D. MINJA1, S. MGEMA2, T.D. MLWILO1, B.K. MAYALA3, S. MSINGWA2, J.J. MASSAGA1 and M.M. LEMNGE1. 1National Institute for Medical Research, Tanga Medical Research Centre, P.O. Box 5004, Tanga, Tanzania Code Number: rb07002 Abstract: A review of plague records from 1986 to 2002 and household interviews were carried out in the plague endemic villages to establish a pattern and spatial distribution of the disease in Lushoto district, Tanzania. Spatial data of households and village centres were collected and mapped using a hand held Global Positioning System and Geographical Information System. During the 16-year period, there were 6249 cases of plague of which 5302 (84.8%) were bubonic, 391 (6.3%) septicaemic, and 438 (7.0%) pneumonic forms. A total of 118 (1.9%) cases were not categorized. Females and individuals aged 7-18 years old were the most affected groups accounting for 54.4% (95% CI: 52.4–56.0) and 47.0% (95% CI: 45–49) of all reported cases, respectively. Most cases were found in villages at high altitudes (1700-1900m); and there was a decline in case fatality rate (CFR) in areas that experienced frequent outbreaks. Overall, there was a reduction in mean reporting time (from symptoms onset to admission) to an average of 1.35 days (95% CI: 1.30–1.40) over the years, although this remained high among adult patients (>18 years). Despite the decrease in the number of cases and CFR over the years, our findings indicate that Lushoto district experiences human plague epidemic every year; with areas at high altitudes being more prone to outbreaks. The continued presence of plague in this focus warrants further studies. Nonetheless, our findings provide a platform for development of an epidemic preparedness plan to contain future outbreaks. Key words: plague, epidemics, pattern, spatial distribution, Tanzania Introduction Human plague is among the three epidemic-prone diseases that are still subject to international health regulations and notifiable to the World Health Organization (WHO, 1994, 2000). The disease is caused by Gram-negative coco-bacilli known as Yersinia pestis. The mode of transmission is through a bite by an infective flea that is harboured by rodents, from person-to-person through aerosols in the case of pneumonic form and by contact with infective fluids of infected animal or human (Lwihula & Kilonzo, 1996; Denis et al., 1999; WHO, 2000). Plague remains the oldest infection in human history and was responsible for many deaths in the three great pandemic in Europe and Asia (Denis et al., 1999; WHO, 2000). Natural foci for sylvatic plague exist in all continents except Australia and the rodent population harbouring the flea vector are responsible for maintaining transmission (Denis et al., 1999). In Tanzania, human plague is an important public health problem since pre-colonial times, and was first documented in 1886 in Iringa region. Afterwards, several foci were identified in different parts of the country, but most of them have remained dormant for many years except for the Lushoto and Karatu foci (Kilonzo et al., 1997). The first outbreak in the Lushoto focus was reported in 1980 involving two neighbouring villages. The disease started in Nywelo as focal point and later spread to the neighbouring Gemai village. Since then there have been a recurrence of epidemics every year involving numerous villages. Bio-medically, plague is characterised by three main clinical forms known as bubonic, pneumonic and septicaemic plague; depending on the mode of transmission and elapsed time from onset to medical intervention (Denis et al., 1999; WHO, 2000). In Lushoto area however, there is a fourth form, recognized by the natives as “Nyungu””plague, which is attached to superstition. It is claimed that this form of plague invariably starts by affecting women though it may later involve other members of the household, depending on if the first victim wished other members to succumb to the disease (Lwihula & Kilonzo, 1996). Based on cultural beliefs, Nyungu plague is best managed by traditional health practitioners through provision of local herbs and observation of some rituals for protection of survivors to bereaved families (Lwihula & Kilonzo, 1996). Lushoto focus has been studied extensively and the pattern of plague epidemic has previously been reported (Kilonzo et al., 1992, 1997; WHO, 2004). Deliberate multi-sectoral control approaches have been undertaken focusing on preventing occurrence of epidemics with an ultimate goal of eradicating the disease (Kilonzo, 1994). Despite these efforts, annual epidemics have been experienced, causing social and economic distress to the general public. Persistence of plague outbreaks in this focus is associated with numerous factors including socio-cultural, economical, as well as ecological and climatical factors (Njunwa et al., 1989; Kilonzo, 1994). It is envisaged that early detection of epidemic is important to prevent loss of lives. Not withstanding this, concrete data to predict plague outbreaks is scarce. On recognising the knowledge paucity and the urgent need for planning meaningful control measures and to develop appropriate tools to predict epidemic occurrence, we therefore, conducted a retrospective review of human plague case records in Lushoto district for the period of 17 years from 1986-2002. Materials and Methods Study area and population The study was conducted in Lushoto district (40 20’S; 38o00’E) in the Western Usambara Mountains, in northeast Tanzania. The altitude ranges from 200m in the lowland to above 2000m in the highland. The district is divided into eight administrative divisions: Mlalo, Mtae, Mlola, Lushoto, Soni, Mgwashi, Umba and Bumbuli. The average annual rainfall ranges from 1400 to 1800mm. The mean annual temperature and relative humidity are 14oC and 70%, respectively. According to national census the total population of the district is 419,970 (URT, 2002). Ninety six per cent of the district population lives in rural areas and their main activity is subsistence farming of vegetables, fruits, maize, Irish potatoes and beans. Most of the inhabitants are the Wasambaa with majority being Moslems. Other ethnic large groups include Wapare and Wambugu. In rural areas most of the houses are made of mud with corrugated iron sheets/tins and about 25% are thatched with bark of cedar trees. The floor and walls are plastered using special clay soil. Due to socio-cultural behaviour and shortage of beds, a slight majority of the population, particularly from large families and those with polygamous marriages, women and preschool children sleep on the floor (Kilonzo et al., 1997). Traditionally, cereals are normally stored in a local ceiling inside the house. Guatemala grass is usually planted along the farmland to prevent soil erosion and also provides pasture for zero grazed cattle. All these provide food and favourable harbourage for rodents in and close to human habitations. Health profile and plague in Lushoto Lushoto district is served by two hospitals, three rural health centres, and 33 dispensaries. In some areas, there are village health posts. During plague outbreaks, temporary treatment camps are established to manage plague cases within the affected area. The leading health problems in the district include acute respiratory infections, plague, diarrhoeal diseases, malaria and intestinal worms. The district has experienced plague outbreaks since 1980. Historically, for the Lushoto focus it is scientifically believed that sylvatic plague existed for many years deep in the natural montane forest of the Western Usambara Mountains; affecting rodents that were permanently harboured within the forest. Human involvement was brought about as a result of ecological disturbance that was prompted by political decisions to open up more land from this forest for agricultural activities, timber industry and human settlement (www.ovc.uoguelph.ca). Data collection methods The study was conducted between January and July 2003 by adopting both retrospective and cross-sectional survey approaches whereby two types of data sets were collected: secondary and primary data. Primary data comprised of spatial and household structured interviews. Spatial data (longitudes, latitudes and altitudes) of households, village centres and health facilities in plague epidemic prone areas were collected using a hand held Global Positioning System (GPS) receiver. Due to influence of recall bias and population migration, structured interviews were limited to households reported to have had experienced plague in the year 2002. During the survey, information on homestead number, name of household head, family size, sex, number of cases per household, type of house, type of walls, type of floor and roof, number of beds and type of bedding materials and food storage were obtained. Secondary data on morbidity and mortality from the district hospital were collected through review of human plague epidemic surveillance register forms for 17 years (1986 to 2002). Social demographic information, data on disease onset to admission, type of clinical forms of disease on admission, duration of hospitalisation and treatment outcomes (cured or dead) were extracted. Data analysis Data on plague outbreaks were double entered into a computer and validated using Epi Info programme version 6.4d. Any differences were resolved by cross checking against the original case record form. Main data analysis was done using Stata version 7 and SPSS version 11 statistical programmes. Descriptive analysis was done to show the distribution of each study variable. Bivarient and multilevel analysis was done to assess the relationship between variables (mean case reporting time, hospitalization duration, age and sex, clinical condition on admission, treatment outcome and year of epidemic reporting). Poisson and linear regression approach was conducted to explore the relationships between relative risk of fatal cases versus other variables adjusted to priori confounding variables. The database was designed after identifying all the entities and attributes required. All plague incidence data were stored in the database to allow for easy retrieval, update, analysis and use. The coordinates were compiled by MS-Excel and saved as dbase (IV) format before being imported into GIS databases and displayed into ArcView GIS Software as point maps. GIS analysis of the stored data was performed by ArcView GIS software after linking spatial data collected by GPS and the attribute data. Through spatial analysis in the ArcView GIS software, contours around the villages and hamlets were created and digital maps displaying human plague distribution pattern were produced. Ethical consideration The study was approved by the Medical Research Coordinating Committee of the National Institute for Medical Research, Tanzania. During the interview and GIS survey, consent to participate in the study was obtained from each participant. All information collected was treated with confidentiality. Results Plague distribution During the 17-year period, a total of 6249 human plague cases were reported from all four affected divisions in Lushoto district and in 1 division in a nearby Korogwe district. Mlola division was the most affected, accounting for 55.7% (3482/6249) of all reported cases (Table 1). Bubonic plague was the most frequently diagnosed clinical form with a prevalence of 86.4%. Out of the total number of plague cases, 6239 (99.8%) had their ages properly recorded. Individuals aged between 7 and 18 years were the most affected group (46.9%). Females accounted for a significantly higher proportion, (54.4%) of all reported cases (P=0.001) (Table 2). The highest number of cases (intensity) (121-140 occurrence per village per thousand populations) occurred in villages located at high altitudes (17001900masl) close to the natural and artificial forests (Figure 1). A positive correlation was observed between intensity and altitude (r=0.52). A unit increase in altitude showed a significant increase in intensity by 0.06 (95% CI: 0.03 – 0.09, P=0.001). Case Fatality Rate Most of the cases were reported during the 1991 epidemic with 19.7% (1228/6249) plague cases (Figure 2). During this outbreak, there were 5.6% (69/ 1228) deaths out of which 18.8% (13/69) were due to the pneumonic form. The disease outcome was available for 97.4% of the recorded cases. The overall CFR was 6.8% (415/ 6086) of which 4.6% (241/5260), 28.3% (121/427) and 13.6% (53/391) were due to bubonic, pneumonic and septicaemic forms, respectively. Over the years, CFR was highest during the 1989 outbreak with a total of 5 (20.8%) deaths out of 29 cases. Based on available data, peak season for plague outbreak was observed in the month of January (Figure 3). The annual trend indicates that human plague outbreak starts around August/September and then declines by May. Villages that experienced sporadic outbreaks had higher number of case fatality rates. Controlling for the effect of altitude, CFR showed to decrease by 1.22 with a unit increase in intensity (95% CI: -2.45 – 0.01, P=0.051) (Figure 4). Case reporting time From the health seeking behaviour pattern, it was noted that the overall mean reporting time (MRT) to health facility/treatment centres from 1986 to 2002 was 1.25 [95% CI: (1.22 – 1.28)] days among 6004 cases (Figure 5). The MRT for bubonic form was 1.20 [95% CI: (1.17 – 1.23)], pneumonic form 1.65 days [95% CI: (1.48–– 1.81)] and septicaemic form 1.60 days [95%CI: (1.42–– 1.80)] among 5132, 366 and 361 cases, respectively. Comparing with the MRT of 1986 epidemic, there has been a significant decrease, [F (16, 5967) =7.42, P=0.001] during the successive epidemics except for the year 1989 and 1992. The MRT for bubonic cases was significantly shorter than for either septicaemic or pneumonic form, [F (2, 5856) =36.98, P=0.001]. Contrast analysis indicated a significant difference in MRT between septicaemic and pneumonic forms, [F (2, 5856) =36.89, P=0.001]. The MRT was 1.17 [95% (CI: 1.10 – 1.24), 1.21 (95% CI: 1.16 – 1.25)] and 1.35 [95% CI: (1.30 – 1.40)] for those aged 1-6, 7-18 and >18 years, respectively. The mean difference was statistically significant, [F (2, 5994) =15.50, P=0.001] whereby those aged >18 years had prolonged MRT. Examining the effect of year of epidemic form of plague and sex on the association of age and mean reporting time, Log likelihood ratio test (LHR) was used by fitting saturated and unsaturated model. The association of age and MRT was not influenced by sex [LHR, c2 =0.08, P=0.773]. Relating reporting time and disease outcome (cured or died), the mean difference was statistically significant (0.46 days, 95% CI: 0.28-0.64, P=0.001). A prolonged MRT was found among those who died after adjusting for sex, age, year of epidemic, hospitalization period and clinical forms of the disease at admission. When adjusting for hospitalization period, age, sex, and year of epidemic, patients with pneumonic form were observed to have prolonged mean days of reporting time (1.91 days, 95%CI: 0.93 – 2.88, P=0.001) compared to other clinical forms of plague. Discussion Our findings indicate that human plague is firmly established in the Lushoto focus with at least an epidemic reported annually since 1986. All the clinical forms exist in the area in varied proportions and the less severe bubonic form, which biologically occurs as a result of infective fleabite, being the most predominant. Similar findings have been reported by Kilonzo et al. (1992, 1997). Bubonic form is an early clinical stage of human plague spectrum; hence the high incidence of this form as compared to the advanced stage of clinical spectrum (septicaemic and pneumonic forms) could be due to early reporting by infected individuals to health facilities or treatment camps. Such an improvement in case reporting and reduced number of cases in some villages over time could be attributed to the existing multi-sectoral involvement in plague surveillance system and other intervention measures. It is most likely that the existing surveillance system might have improved not only community awareness of the disease leading to prompt health-seeking behaviour but also full commitment in the fight against the disease as it has been reported by Kilonzo et al. (1997). It is also likely that man-to man transmission through aerosol is rare given the low proportion of pneumonic form reported in the period under review. Overall, females and school age group population (7-18 years) were mostly affected by plague. This is likely to be associated with socio-cultural behaviour and economic activities of the local population. In Lushoto, females and children are actively involved in productive activities such as collecting firewood from the nearby forest, farming and looking after zero grazed livestock. Socially, it has been documented that females and children in large families with inadequate number of beds, do sleep on the floor (Lwihula & Kilonzo, 1996; Kilonzo et al., 1997). This habit might contribute to predisposing the group to fleabites and hence, the high infection rate. Despite an initial decline in the incidence of plague in Lushoto focus, the number of cases during the 1991 was high. This was contributed by marked increase in rodent population, which led to most individuals applying Zinc Sulphide as a rodenticide. This rodenticide led to fast killing of rats that resulted on fleas searching for an alternative host (S. Mgema, unpublished data). Cases were few in subsequent years after reinforcement of by-laws and encouraging use of slow killing rodenticides such as Bromodialine®. However, there is still a problem of sustainability in the control measures. It appears that the current interventions are not routinely maintained and thus allow for potential subsequent outbreaks. The sustainability of these interventions could be achieved through bottom up approach, involving community members in the planning and implementation of control measures with minimal support from the district and the Ministry of Health. Interestingly, spatial distribution of human plague epidemics indicated that most cases were observed in villages located at high altitudes. This pattern could be due to ecological predisposing risk factors including proximity of villages to natural and artificial forests, and residential houses close to farmlands. It is thought that at high altitude patchy of montane forests still exist, and they harbour different species of rodent population, which are the main reservoir for human plague (Njunwa et al., 1989; Makundi & Kilonzo, 1994). As for the farmland, Guatemala grass is usually grown on the steep slopes to prevent soil erosion and provision of pasture to zero-grazed cattle, is likely to provide good shelter, breeding site and source of food for rodent population. In terms of spatial distribution, the results revealed a characteristic seasonality pattern in plague outbreaks throughout the period under review, with peak outbreaks in January and December. Such a seasonality pattern could either be attributed to climatic factors or socio-economic activities that expose human hosts to infective vectors. Findings from other investigators (Njunwa et al., 1989; Makundi & Kilonzo, 1994) have similarly correlated seasonal pattern on human plague with rodent and fleas population. In terms of control, this seasonality offers a potential opportunity for the district administration and other stakeholders for epidemic preparedness and timely response. Mean reporting time was observed to decline over the years and was associated with decrease in plague CFR. The promising achievement in reduction of CFR and early treatment seeking behaviour among plague cases might have been accelerated by improved knowledge on the disease through multi-sectoral plague control approach. The role of self-medication with antibiotics which is practiced in the area (Lwihula & Kilonzo, 1996) might have contributed to the decline of CFR. Nevertheless, this practice could contribute to evolution of drug resistances due to suboptimal dosage. It should be noted that the findings reported here have limitations and should be interpreted with cautions. This is mainly because reliability of the information given depends on history narrated by the patients/guardians regarding symptoms onset to the time of admission. In conclusion, plague outbreaks occur annually in the Lushoto focus, usually starting in August or September, and that areas at high altitudes are at the highest risk. This calls for sustainable multi-sectoral control approach to eradicate the disease in the foreseeable future. With the annual plague epidemics in Lushoto, there is need to strengthen the district surveillance system and develop an early warning system that can be used to detect an impeding epidemic in future. The database that was developed in study provides a baseline that could be utilized in the monitoring plague epidemics in the district. Acknowledgements The authors acknowledge with many thanks the technical assistance of Messrs Aza Kimambo, Benson Swai and Hebert Kivunga, and Ms. Christina Mpalahole. The authors would also like to thank the Lushoto District Council Health Management Team, village leaders and village members for their cooperation and enthusiasm. Prof. Chris Curtis of London School of Hygiene and Tropical Medicine and Dr. Leonard Mboera of National Institute for Medical Research, Tanzania, are thanked for their comments on the earlier version of the manuscript. We are grateful to Dr. Andrew Kitua, Director General, National Institute for Medical Research for the logistical support and permission to publish these results. This study received financial assistance from the Ministry of Health and Social Welfare, Tanzania. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07002f2.jpg] [rb07002f4.jpg] [rb07002f5.jpg] [rb07002f3.jpg] [rb07002t2.jpg] [rb07002t1.jpg] [rb07002f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}