 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
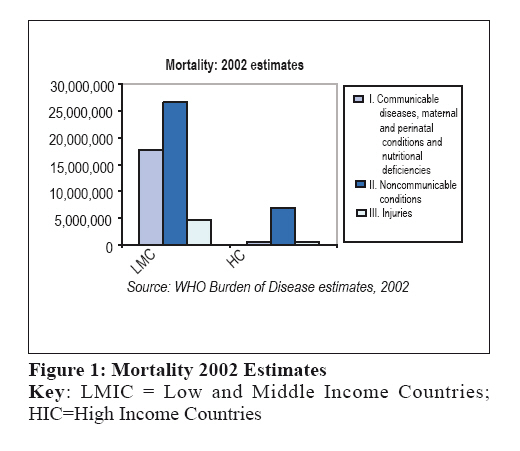
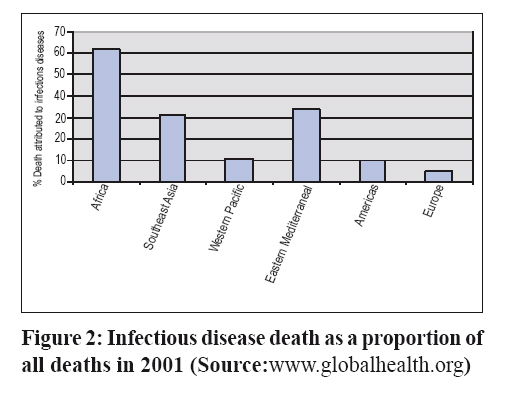
Tanzania Health Research Bulletin, Vol. 9, No. 3, 2007, pp. 147-153 Health research agenda for East Africa in the new millennium: looking ahead A.Y. KITUA National Institute for Medical Research, P.O. Box 9653, Dar es Salaam, TanzaniaE-mail: akitua@nimr.or.tz;akitua@hotmail.com Code Number: rb07025 Abstract The Regional East African Health Research agenda was presented as a keynote speech during the first East African Health and Scientific Conference, held in Kampala, Uganda from 28th to 30th March 2007. The agenda was developed through a critical analysis of the global, African and Regional East African health challenges and mitigating strategies, taking into account the Millennium Development Goals (MDG), the Abuja declaration and the New Partnership for African Development as background environment, within which the Agenda will operate. It is proposed to: establish a joint mechanism for research coordination, promotion and regulation; establish stronger collaborative mechanisms for research and training; create a joint Regional East African Community health research and development fund; create joint intellectual property rights protection mechanism, enhance patenting and link research to industry; create a mechanism to enhance translation of research to policy and practice; strengthen clinical research capacities; and strengthen innovation and discovery research capacities. Effective implementation of this agenda will greatly raise the profile and quality of research in the region and improve the health status of the East African populations. Key: health research, agenda, challenges, disease burden, East Africa Introduction The proposed Regional East African Health Research agenda, presented in this paper, was developed through a critical analysis of the health challenges and mitigating strategies. The analytical process began at the global level, descending to the African, and finally the Regional East African Community (REAC) level. This is because, for it to be practical and produce the desired effect, it has to operate within the Global and African environments. The analysis took into consideration the current status of Health Research in the REAC in terms of existing strengths, weaknesses, opportunities and imminent or remote threats. It recognizes the need for attaining a high level of competitiveness and hence comparative advantages in this era of globalization. The discussions evolve around what I believe to be the three sides of the health triangle namely the population health status (indicated by the disease burden), the health system, and the health research organization (research and academic institutions), which dictate upon the research environment. The Global disease burden and challenges At the entrance into the 21st Century, the global community adopted the United Nations Millennium Declaration (UN, 2002a), and translated it into global commitments, the so-called Millennium Development Goals. These goals were set to meet the global challenges of accelerating human development and eradicating poverty (UN, 2002b). Three of the eight goals address health and these are Goal 4: Reduce child mortality, Goal 5: Improve maternal health and Goal 6: Combat HIV/AIDS, malaria and other diseases. This is testimony of the importance of health for development in the New Millennium and the need to break the vicious cycle of poor health, poverty and poor health. Achieving these goals requires strong advocacy, mobilization of global resources and the implementation of well planned effective interventions, because the challenges are enormous and their mitigation will require huge investments. Global efforts should recognize that there is a great variation in the levels of economic power and disease burden between and within different regions of the world as well as between and within countries. Indeed global estimates in 2002 indicate that low and middle income countries bore more than two thirds of the global disease burden (WHR, 2002; Kitua, 2005; Jone et al., 2003), caused by communicable diseases, maternal and perinatal conditions, and malnutrition (Figure 1). All these conditions are preventable through access to and effective use of scientifically proven interventions like children immunization and water sanitation. Hence attention should be directed at a more equitable allocation of the available global resources. Countries with limited resources could therefore not be expected to meet the Millennium Development Goals alone, simply because the disease burden bearing on them is enormous and would require much more resources beyond what they can afford. Unfortunately, Africa bears the greater portion of this burden. Child mortality in Africa (under five years probability of death) is above 160 per 1000 live births while no other continent or region has child mortality exceeding 100 per 1000 live births (WHR, 2003). Adult mortality (probability of death between age 15 and 60 years) is similarly unacceptably high in Africa, being over 500 per 1000 population while no other region exceeds 200 per 100 population6. Sub-Saharan Africa, and hence the REAC countries demonstrate the worst global statistics concerning both child and adult mortality (Figure 1, 2, and 2; Table 1). Global resource mobilizations and allocation The global response has been positive, and efforts initiated and led by Kofi Annan, the former United Nation’s Secretary General, have established a global facility “the Global Fund for HIV/AIDS, Malaria and Tuberculosis”, which by May, 2005, had signed grant agreements worth US$ 2.4 billion for 279 grants in 125 countries. The Bill and Melinda Gates Foundation has provided substantial contributions to fight the same diseases, and the President's Emergency Plan for AIDS Relief (PEPFAR) has further contributed globally US$ 8.3 billion during the period 2004-2006 and most of it has gone to Africa. The long standing UNICEF/UNDP/WORLD BANK/WHO Special Programme for Research and Training in Tropical Diseases (TDR) has increased its biennial fund allocation from US $ 60 million in 2000/2001 to US $100 million in 2006/2007 (TDR, 2006). Furthermore, the European Commission has catalyzed the formation of the European Developed Countries Clinical Trials Partnership (EDCTP), to strengthening South North and South-South partnerships, and to enhance the capacities of African countries to conduct quality clinical research required to improve clinical practices. Moreover, the Netherlands Organization for Scientific Research strategy is to contribute to the realization of the Millennium Development Goals and hence its research agenda will focus on poverty and hunger, global health and health system, sustainable environment and global relationships (www.wotro.org) Table 1: The burden of Childhood Disease
*Diseases preventable with currently available vaccines in the Expanded Programme on Immunization: diphtheria, pertussis, tetanus, polio, measles (Source: WHO Ad-Hoc Committee) There is indeed substantial increase in the global expenditure for health research (GFHR, 2004). The estimated global expenditure for health research in 1986 was US$30 billions, which rose to US$84.9 billions in 1998 and had reached 105.9 billions in 2001. However, currently resources are not reaching those who need them most. As already revealed in 1996, there is still gross imbalance in the allocation of globally available funds for health research, termed the 10/90 gap, whereby over 90% of the Global funds are used by high income countries, towards 10% of the global disease burden, leaving the low and middle income countries to share only 10% of the funds to meet 90% of the remaining burden (WHO, 1996; GFHR, 2002). Throughout this period the expenditure for research in Low and Middle Income Countries has not exceeded ten percent of the available funds (Matlin, 2005). Hence there remains the challenge of equitable fund allocation requiring proportional allocation according to the gravity of the burden of ill health, ensuring that interventions reach those who need them most. The African response The Millennium Development Goals have been translated into the Abuja Declaration (ADF, 2000)) reaffirming African countries commitments to meet the challenges, as declared by the African heads of states: “We gathered in Abuja to undertake a critical review and assessment of the situation and the consequences of these diseases in Africa, and to reflect further on new ways and means whereby we, the leaders of our Continent, can take the lead in strengthening current successful interventions and developing new and more appropriate policies, practical strategies, effective implementation mechanisms and concrete monitoring structures at national, regional and continental levels with a view to ensuring adequate and effective control of HIV/AIDS, Tuberculosis and other related infectious diseases in our Continent (ADF, 2000). The Abuja Declaration emphasizes the public health approach of reaching over 60% coverage of vulnerable populations with effective interventions. In order to maximize the economical power and effective use of limited resources, Africa has established an Integrated Social Economic development framework called the New Partnership for African Development (NEPAD) (NEPAD, 2005), whose primary objectives are: (i) To eradicate poverty; (ii) To place African countries, both individually and collectively, on a path of sustainable growth and development; (iii) To halt the marginalization of Africa in the globalization process and enhance its full and beneficial integration into the global economy; and (iv) To accelerate the empowerment of women. While two of the four NEPAD (2005) objectives address health from the capacity building and human development angle, with focus on health education, technology and skills development, the health sector strategic direction follows a comprehensive, integrated approach with seven components namely: Strengthen commitment by and the stewardship role of government; build secure health systems and services; strengthen programmes to reduce the burden of disease; provide skilled care for pregnancy and childbirth; enable individual action to improve health; Mobilize and effectively use sufficient sustainable resources; and strive for equity for the poor, displaced and marginalized. African disease burden Available statistics show that the proportion of under nourishment has remained above 23% while the absolute numbers have increased substantially. There has been a gradual increase in proportion and absolute numbers of wasted children and the proportion of stunted children has remained above 30% while the absolute numbers have increased significantly from 36.4 million to 48.5 millions (UN, 2004). Africa presents high level of iodine deficiency (U1<100 mg/l) in general population and in school aged children 6-12 years respectively being 324 millions (43.0%) and 60 millions (42.7%). This picture is a reflection of the level of poverty in Africa. It is estimated that the number and percentage of people living under a dollar per day in 1990 and 1999 is respectively 241 Millions (47.4%) and 315 millions (49.0%). Table 4: Nutritional Status Trends for <5 in Africa
Source: Adopted from the Standing Committee on Nutrition (SCN) 5th Report on World Nutrition Situation (2004) East African health burden and challenges The REAC member states bear similar levels of the health burden and together portray almost a mirror image of the African health burden. Life expectancy at birth is similarly low in all the three East African Countries indicating that people die very young (range 44-51 years). Maternal Mortality ratio remains above 500 per 100,000 live births in the three countries and infant mortality is above 60 per 1000 live births – both being unacceptably high. Crude death rate, maternal mortality, infant mortality and under five mortality remain unacceptably high (Table 5). Table 5: Health Status Indicators 2005
The GDP per capita ranges between US $ 500 and 1500 and the three countries of Tanzania, Kenya and Uganda are all classified as low income states by World Bank standards. Table 6: Health indicators (in percent) for the East African Countries in 2005
The prevalence of underweight, stunting and wasting in the population of Tanzania, Kenya and Uganda is 31%, 42.2% and 6% respectively (de Onis et al., 1997) (Table 7). The intolerable high level of undernourishment in the population of East Africa further shows that except for minor variations there hasn’t being any marked improvement in the nutrition status over the period between 1990 and 2001. The situation is also similar to the malnutrition status among the population of Burundi (49-70) and Rwanda (41-50%), the central African countries that joined the East African Community recently. Table 7: Number and percent of undernourishment in the population of East Africa
The main Regional East African challenges can be classified into seven specific areas namely:infectious and parasitic diseases burden; maternal and perinatal conditions; under five mortality; respiratory infections; nutritional deficiencies; emerging non communicable disease epidemic; and communicable disease epidemics such as viral haemorrhagic fevers. HIV/AIDS, malaria and tuberculosis are still of great concern to the region. Currently there is an emergency of Rift Valley Fever (http://www.phschool.com/science/planetdiary/archives07/ and the threat of Birds Flu is real given that human cases have been documented in Africa. The three countries face disease transitional changes especially in urban populations where Non Communicable Disease (NCD) conditions like obesity related cardiovascular complications and diabetes are on the increase. The EA Countries face severe human resource shortages in health, a situation aggravated by the conditions imposed upon these countries by the International Monetary Fund in the early 1990s, not only to halt health workers recruitment, but also retrench and downsize the workforce in existence then. The rural communities are worse hit. Poor infrastructure coupled with poor remuneration of health professionals and lack of differential incentives makes it extremely difficult to attract well-trained personnel to work in rural areas. Access to quality health services is therefore a major challenge especially concerning rural populations. The major five challenges in health systems include: severe shortage of human resources for health; Inequity in distribution of health services; the urban rural divide; availability of quality health services; access to quality health services; and coverage with effective health interventions. It has been recognised that a socially complex health interventions requires not only that health systems manage their current functions better, but also demands new kinds of performance from these systems. For instance, with the current HIV/AIDS pandemic, health delivery needs to be oriented from acute to chronic disease care. It is important to note that access to health care in most developing countries cannot occur on any substantial scale without health system strengthening (Schneider et al., 2004). The bulk of health research conducted within any one of the REAC member state is not yet proportionate to the health burden and hence research needs. There is inadequate coordination and institutional collaboration in health research between and within member countries. Member states lack effective strategies to meet the severe shortage of health personnel and research scientists. Data to guide strategy formulation is missing partly due to inadequate funding of priority research. Donor dependency continues to prevails even though member states have long recognized the value of research and own well established national research institutions. It follows that the main challenges for sustaining robust and quality competitive research in East Africa include: research coordination and collaboration between and within countries; production and retention of highly qualified research scientists; availability of adequate specialized and well equipped laboratories; capacity for basic innovative research (product development capacity); capacity for testing tools (clinical and intervention studies); link between research and policy and practice; link between research and industry (patenting and patent selling/holding); and adequate funding for research. The proposed agenda The objectives of the proposed Regional East African Health Research agenda should therefore focus on addressing the above highlighted challenges in a concerted manner so as to register measurable impact as quickly as possible. These eight objectives are: to strengthen partnership and collaboration in health research among the member states; to accelerate the production of quality scientists to maintain the critical mass for researchers and scientists within the region; to improve and maintain quality research standards; to strengthen regional competitiveness in innovation and discovery; to ensure the conduct of sufficient societal relevant and demand driven research to meet the urgent regional needs; take greater stewardship and active participation in seeking solutions to our common health problems; to promote research and utilization of research results for policy and practice and to; maximize use and impact of limited resources for research and development. I therefore propose the following research agenda for the Regional East African Community: a) Establish a
joint mechanism for research coordination, promotion and regulation. Under each agenda item are a number of activities, which are felt to be realistic, focused, achievable and have potential for major impact, in the ambits of limited resources. Agenda 1: Establish a joint mechanism for research coordination, promotion and regulation. 1.1 Establish
the REAC Health Research Council/commission Agenda 2: Establish stronger collaborative mechanisms for research and training. 2.1 Establish
consortia/partnerships and networks for the design and conduct of focused joint
research and training activities facilitating access to globally available
funds Agenda 3: Create a joint REAC health research and development fund 3.1 With
Member states contributions Agenda 4: Create joint IPR protection mechanism to enhance patenting and link research to industry. 4.1 Establish
joint training programme/curricula on Intellectual Property Rights Agenda 5: Create a mechanism to enhance translation of research to policy and practice. 5.1 Establish
and support a central coordination mechanism for research to policy and
practice Agenda 6: Strengthen clinical research capacities 6.1 Establish
Centres of excellence in clinical research and training Agenda 7: Strengthen innovation and discovery research 7.1 Establish
regional reference laboratories Discussion It is realised that the challenges ahead of us in our endeavour to improve the health status of our populations. To meet these challenges requires the guidance of quality and innovative research. Indeed research has to run ahead of policy and decision-making, as well as guide the implementation of health interventions and practices. Countries can and should allocate a greater proportion of their national budgets for health and similarly a higher proportion of their health budgets for health research. Efforts should be strengthened to achieve the target of allocating 1% of national GDP per capita on health and 5% of partner support towards health research. Ministries of health should ensure to allocate a minimum of 2% of the health budget for health research. Recognizing the need and desire to improve the health of the East Africans, the Community has recently, established an institutional mechanism (to operate under the East African Health Research Commission) to bridge the gap between evidence and health policy and practice. It is envisaged that this initiative will greatly improve the information available to policy makers and policy making bodies to establish evidence-informed health policy. In conclusion, the Community is the vehicle in which we can move forward faster towards our goals and targets. It will mobilize regional resources to provide the fuel for running the engines. We are the Community brains. We must determine the direction in which the Community should move and clear obstacles so that it can move with the highest possible speed. It is our responsibility to take the driving seat and guide the vehicle of our destiny and the destiny of our future generations. This proposed Agenda is meant to provoke our resolve and strengthen implementation of our commitments in the Abuja declaration, and hence accelerate our speed towards achieving the Millennium Development Goals. Acknowledgements This works received financial and logistic support from the East African Community Secretariat. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07025f2.jpg] [rb07025f1.jpg] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}