 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Health Research Bulletin, Vol. 9, No. 3, 2007, pp. 174-179 Onchocerciasis situation in the Tukuyu focus of southwest Tanzania after ten years of ivermectin mass treatment C.N. MWEYA1, A.K. KALINGA1, B. KABULA1, K.D MALLEY1,M.H. RUHISO2¥ and B.T.A. MAEGGA1* 1National
Institute for Medical Research, Tukuyu Station, P.O. Box 538, Tukuyu, Tanzania Code Number: rb07030 Abstract A purposive cross-sectional epidemiological study was conducted in the Tukuyu Onchocerciasis focus in south-western Tanzania in 2004, ten years after launching the ivermectin mass treatment programme, and 23 years after establishing focal parasite prevalence. The objective was to assess contemporary Onchocerciasis clinical and parasitological situation and assess community knowledge about the disease and its control. From historical data, five villages with high parasite prevalence were selected, two each on the Lufilyo and Kiwira Rivers and one on lower Lumbira River. Skin biopsies were taken from the iliac crest on the left and right buttocks, for examination of Onchocerca volvulus microfilariae. Onchocercal skin lesions were checked using natural light, while nodules were palpated from head to ankles and scored. A structured questionnaire was administered to participants.A total of 438 persons (age=16-99 years) were examined. No skin microfilariae (mf) were detected. Onchocercal skin symptoms were found in 170 (38.8%), of which 30 (6.9%) had nodules, 48 (11.0%) chronic onchodermatitis and 92 (21%) itching. One-third (34.5%) had correct knowledge that black flies ("tusunya") are vectors of onchocerciasis. Half of the respondents (n=217) confirmed taking ivermectin for onchocerciasis treatment, and 428 (97.7%) were willing to continue for any duration. It is concluded that the undetectable skin microfilariae in the study sample was partly attributable to the consequences of ongoing ivermectin mass treatment. It is recommended that the control efforts, as well as monitoring and evaluation be sustained to determine its long term impact, and that a more sensitive technique be used to check O. volvulus skin mf prevalence. Keywords: Onchocerciasis, ivermectin, CDTI, microfilaria, Knowledge, Tanzania Introduction Human onchocerciasis is a parasitic disease caused by a filarial nematode, Onchocerca volvulus. Globally, onchocerciasis affects approximately 18 million people, the majority of them in Sub-Saharan Africa, where it is responsible for the loss of 1 million DALYs annually (WHO, 2002). The endemic zone stretches across a broad middle band, covering 28 countries, from Senegal in the west to Ethiopia in the East, on its northern limits and in the south, from Angola to southern Malawi. While in west and central parts of the continent, the disease has more continuous distribution owing to the relatively uniform land terrain, in Eastern Africa, it is more focal in distribution due to the variations in the land relief, brought about by the influence of the Great Rift Valley and associated blocks of mountains. In Tanzania, the disease is endemic in 15 districts, with an estimated 4 million persons at risk. The foci are closely associated with series of Block Mountains that run in an arc-like chain, from Northeast Tanzania to Northern Malawi, from Tanga region to Ruvuma and south-western Mbeya regions (Raybould & White, 1979; Maegga, 1991). In Morogoro and Ruvuma regions, all district have hyperendemic communities, while in Iringa, Mbeya and Tanga, only some districts are endemic and others are not. In the highlands of Iringa region, onchocerciasis was initially known from Ludewa district, in an area contiguous with Mbinga district of Ruvuma region. However, recently, meso- and hyperendemic communities have been found on the slopes of southern Udzungwa Mountains in Mufindi and Njombe districts (B.T. Maegga unpubl.), bordering Kilombero district. In 1993, it was estimated that about 650,000 people were infected with O. volvulus in Tanzania (WHO, 1995), but by 1997, those at risk were estimated to be approximately 4 million persons, while slightly over one million were already infected (MoH, 1997). Mwaiko et al, (1990) reported wide variations in the disease prevalence in different foci, being high in the Bwakira area, southern Uluguru Mountains (63.6%) in Morogoro, Mahenge (58.6%), and Ruvuma (31.9%); and low in Amani (22.4%) and Tukuyu (22.8%). However, in some foci, the endemicities have changed considerably in recent years due to continuous changes in the demographic characteristics coupled with local environmental and global climatic changes. Due to the high onchocercal blindness in the dry savannah zone of West Africa, the first large scale control initiative based on vector control approached (Onchocerciasis Control Programme) was launched in 1974. This seven country programme was soon extended to include eleven countries in West Africa, to curb vector re-invasion from the outside surrounding areas (Cheke & Garms, 1983; Yameogo et al., 1996). The programme involved aerial spraying of 50,000km of river stretches to clear the vector and succeeded in stopping disease transmission from its core area in the Sahelian countries (Davies, 1994; Yameogo et al., 1996). Vector repopulation would occur once insecticide treatment ceased because large areas to the east of the programme zone still supported vector breeding in similar ecological habitats (Davies, 1994). Thus frequent insecticide treatment was sustained for a long time. With the introduction of ivermectin (Mectizan R), the chance for reducing the parasite reservoir in the communities while vector control was implemented became available, in the 1980s. The combined vector control and ivermectin mass treatment successfully eliminated onchocerciasis both as a public health problem and hindrance to socio-economic development in the former West African Onchocerciasis Control Programme (OCP) countries. Ivermectin was adopted for large scale population treatment, first in the OCP countries and later, in all the endemic countries of tropical America and Africa. For its many advantages of ivermectin mass chemotherapy for the control and prevention of onchocerciasis became the method of choice instead of the relatively expensive vector control campaigns. African Programme on Onchocerciasis Control (APOC) was launched in December 1995, and became fully operational in 1997. Its main goal was to use mass ivermectin treatment to eliminate onchocerciasis as a public health problem and a hindrance to socioeconomic development in all endemic communities in Africa. APOC adopted Community Directed Treatment with Ivermectin (CDTI) for implementing the mass drug administration as the best option for long term sustainability. In Tanzania the strategy was adopted in 1997, when its implementation began with Mahenge focus, and later extended to Ruvuma (1998), Tanga and Tukuyu (1999), Kilosa (2003), Morogoro (2004) and finally to Tunduru (2005). These individual projects compose the National Onchocerciasis Control Programme. In common to all foci, no pre-treatment baseline data exists for monitoring and evaluation of the programme impact. However, Tukuyu focus had historical onchocerciasis epidemiological data including quantitative transmission indices that predated drug distribution. Tukuyu ivermectin mass treatment was started in 1994, as a vertical programme, with drug distribution executed by a mobile team. From 1999 onwards, the project was converted to “Community Directed Treatment with Ivermectin” (CDTI), and was simultaneously integrated into the primary health care system of the district (PHC). In 2002, out of the estimated eligible 92,530 people in the focus, 63,540 (69%) were treated (Annual Report 2002, Ministry of Health, unpubl.). The current study was aimed at assessing the impact of ivermectin mass treatment in selected communities for any tangible changes since the last historical epidemiological data was collected. The specific objectives were to assess the parasitological and clinical status of the disease following annual ivermectin mass treatment, and to assess the level of community knowledge, and attitudes towards the disease and its control. Materials and Methods Study area Tukuyu Onchocerciasis focus is located largely in Rungwe District, but parts of it lie in Kyela, Ileje and Ludewa districts. The approximate focal geographical boundaries lie between 9015’S, and 9045’S; and 33030’E and 34000’E in south-western Tanzania. Rungwe is highly mountainous, with Rungwe and Kyejo dormant volcanic summits in the north, in a high altitude zone reaching over 3000 meters above seas level. There are the Undali and Umalila mountain ranges running in a north–south-western direction to the west while the Kipengere and the Livingstone Mountain ranges run north–south-eastern direction towards its eastern side, these form the dividing line of the drainage systems to the west and the east of the area. Many rivers originate from the north flowing towards Lake Nyasa in the south, providing abundant suitable breeding sites for Simulium black flies. Study design and sampling procedures This was a purposive cross-sectional study in which a multistage sampling procedure was used. Villages selected according to endemicity status, being meso- and hyper-endemic onchocerciasis, and in the vicinity of dense vector breeding stretches, with comparatively high transmission indices (Pedersen & Kolstrup, 1986; Pedersen & Maegga, 1985). From each district the indicator villages were chosen on the basis of onchocerciasis endemicity levels and nearness to rivers sections with S. damnosum dense vector breeding, from historical data (Pedersen & Kolstrup, 1986; Pedersen & Maegga, 1985) for Rungwe and Kyela. Villages in Ludewa and Ileje were selected on the criterion of closeness to potential vector breeding and proximity to high prevalence villages in the other two districts. Subsequently, households were randomly selected. The selected villages were from Kifunda, Kisegese and Lutete wards in Rungwe, Lumbira in Ludewa and Kapeta in Ileje districts. Adequate community mobilization and sensitization was done, and then a total of 438 persons (age=16-99 years) were recruited for study, after obtaining an oral informed consent. From randomly selected households, individuals of 15 years and above, both sexes, were interviewed, and outcome recorded. Two Village leaders in each village were also interviewed. Interviews involved a structured questionnaire to assess participants’ awareness and knowledge of onchocerciasis disease, its signs and symptoms, its treatment, how they viewed the treatment and willingness to continue treatment indefinitely. All persons were examined clinically for skin signs and symptoms of onchocerciasis, which were dully recorded on a chart. Nodules were palpated from head to the ankles according to Ngoumou & Walsh (1993). Females were examined by a trained female nurse. Individuals were also asked if they had any palpable nodules on their bodies. Additional signs and symptoms recorded included “leopard and lizard skin”, darkened skin (chronic onchodermatitis), scratch marks, papular skin rash signs of acute onchodermatitis. Two skin biopsies were taken from left and right iliac crests, using a single use razor blade as a safety precaution to avoid contamination. The skin specimens were individually incubated in physiological saline in sterile micro-titration trays, with adequate labelling. Specimens were first checked under a low power magnification of a dissecting microscope after 30 min. and if negative, repeated after 24h for the presence of O. volvulus microfilariae, and recorded. Data analysis Data collected were entered into the computer and managed using Epi-Info version 6.4d. Descriptive analysis was done to explore cross relationship between variables. Appropriate statistical packages were used to determine the difference in distribution of disease symptoms between age groups and villages. Where necessary all levels of statistical significance were determined at P<0.05. Results A total of 438 (males=220; females= 218) people were examined and interviewed. The mean age was 40.4 years (range =16 to 99 years). The majority (96.1%) were subsistence farmers, with few fishermen and petty traders. Literacy rate was moderately high. Of the respondents, 68.5% (300/438) could read and write while 69.4% (304) have had formal education. Table 1: Distribution of onchocercal nodules, chronic and acute skin lesions in five villages surveyed in 2004
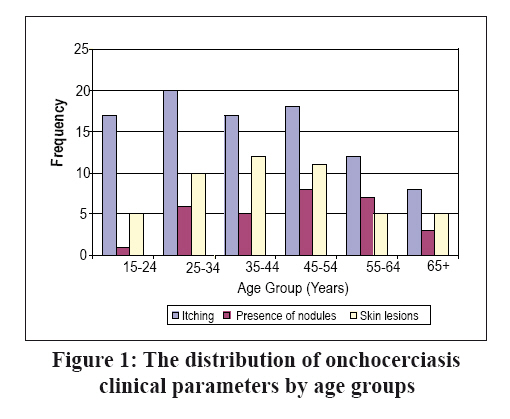
The two biopsies taken and examined from 438 participants were negative for O. volvulus microfilariae. Of persons clinically examined, 170 (38.8%) had one or more of the common symptoms of onchocerciasis. Nodules and chronic skin lesions (e.g. leopard or elephant skin) were observed in 30 (6.9%) and 48 (11.0%) respondents, respectively. Severe itching was reported by 92 (21%) participants (Table 1). The distribution of onchocerciasis clinical manifestations by age group is shown in Figure 1. Prevalence of symptoms varied significantly between age groups (P=0.04) and between villages (P=0.003).During the baseline survey in 1981, the microfilariae prevalence was highest (62.8%) at Kilugu and lowest (41.1%) at Kipapa. However, none of the examined individuals had skin mf after 10 years of intervention (Table 2). Table 2: Onchocerca volvulus skin mf prevalence in villages before and following the start of mass treatment with ivermectin in 1994
Key: NS= Not sampled at the time Onchocerciasis was not ranked among the top five health problems as mentioned by 37 (9.5%) of the respondents, while malaria was rightfully ranked as the number one health problem by 86% of the respondents. On the other hand, 260 (59.4%) claimed to have heard about “Usubi”, which is the Kiswahili name for onchocerciasis. The respondents knew common signs and symptoms of the disease such as persistent itching of the skin, insomnia, leopard-like patches on the skin, hyperpigmentation, hardened, rough lizard-like or elephant like skin, general body weakness and persistent headaches. The main sources of information about the disease were health personnel (including members of the council health management team) and radio. Other sources included leaflets and newspapers. Knowledge of the diseases was also attained through experiences of affected persons who could be friends and / or relatives, and village leaders. A total of 151 (34.5%) of the respondents mentioned black-flies as the main vector of the disease. Many of the respondents knew the blackfly by its vernacular name “tusunya”, and that it bites near rivers, in gardens and farming plots where most of the subsistent activities are carried out. To control of the disease, 310 (70.8%) persons knew they were required to take ivermectin tablets once a year and 50% claimed to have taken it more than twice before this study, as a means of treatment of the disease. However, 214 (48.92%) persons who took ivermectin regularly did not seem to know what its use was, whereas 224 (51.1%) claimed to have been educated about onchocerciasis and the use of ivermectin to treat and control it. Only a few people knew that killing the blackflies could be used to control the disease, as 18 (4%) persons mentioned insecticide spraying into rivers as one way of controlling the disease by killing the vectors. About one-third (37.5%) of the respondents claimed to have experienced adverse reactions after taking ivermectin for the first time. The adverse reactions included swelling of the whole body or that of some parts (N=58), severe intense itching (N=56). Other less frequently mentioned reactions were fever, vomiting, headaches and general malaise by 59 people. Of those who experienced adverse reactions during their first treatment cycle, 52.6% (91/173) sought help from health facilities while others recovered spontaneously. The majority of respondents 428 (97.7%) professed to be willing to continue taking ivermectin for many years, even for as long as they live, and 310 (70.8%) knew they have taken it once a year several times already, while 50% claimed to have taken it for more than two years before this study. Discussion In the current study, no skin microfilariae were detected in the study population which initially had relatively high microfilariae prevalence as shown in the historical data of 1981 and 1997. The general trends indicate reduction of skin mf counts during the ivermectin mass treatment period, compared to the pre-treatment period of 1981. In other studies, skin mf were reduced to detectable levels for several months following ivermectin administration, and transmission was noticeably reduced within three to six months period. While it is quite possible that the method used was not sensitive enough to pick microfilariae at low skin counts, the absence of positive skin biopsy is partially attributed to the reduction of mf reservoir in the communities treated. The evidence that skin mf was still present during part of the treatment period was confirmed by infected and infective flies captured during 2001 to 2003 (B.T.A. Maegga, unpubl). On the other hand, if mass ivermectin treatment had taken place within the period of 3 months before the study, this would result in periodic clearing of skin mf for up to 3-6 moths. This implies that following that duration, skin mf count could slowly increase so long as there are fertile, viable adult worms in nodules and the reservoir becomes available for transmission by the vector black flies. There were palpable nodules in 6.8% of the total examined, the proportion varying from village to village. It is known that low skin mf count can be missed in the skin biopsy using the sclero-corneal punch, and possibly also while using a razor blade method (Collinset al., 1980). Often, vector flies manage to pick up parasites even at low count. Consequently, there is a need to countercheck the findings using more sensitive techniques, while at the same time monitoring transmission indices in the vicinity of surveyed villages. In addition, onchocercal clinical manifestation indicators were still quite visible, and acute onchodermal lesions, including itching were reported. This was also another evidence of continuing transmission. As long as there are palpable nodules, and transmission is still detectable, there is need to strengthen an active surveillance and sustain mass treatment. Very little systematic work has been done on the socio-economic impact of onchocerciasis and its intervention measures in Tanzania, in general, and especially, in the Tukuyu focus. Lakwo (2006) studied factors associated with non-adherence to community directed treatment with ivermectin (CDTI) for onchocerciasis control in the focus, and observed that, although the knowledge on the disease was relatively high, knowledge on its causes was rather low, while about one-third of those interviewed had no idea of its cause. The author found that there was generally inadequate health education in the communities, and local negative beliefs and alcoholism contributed to non-adherence to treatment schedules. These factors will affect treatment coverage and the ultimate success of the CDTI programme. Information generated from the assessment of the knowledge, and perceptions of villagers with regard to onchocerciasis and ivermectin treatment will be very useful in the development of appropriate community health education materials. In this study, it has been shown that the level of knowledge about the disease was reasonably high with regard to skin symptoms, as many respondents could identify affected people on basis of their skins lesions. However, this was unfortunately not demonstrated with respect to its cause and mode of transmission as well as disease progression. The health education messages should address this area with a view to averting possible misconceptions that may arise. With regard to the attitude towards ivermectin treatment community members were positive about the drug, notwithstanding the side effects experienced. There is need for continuing appropriate and adequate health education and communication messages to community members on the various aspects of the disease, its signs and symptoms, its ecology and life history and the current interventions, in order for them to see logic in the need for long term treatment with ivermectin. Acknowledgements We gratefully acknowledge the financial support of the National Institute for Medical Research, and technical and administrative contributions of Rungwe District Council Health Management Team. We also acknowledge the support and friendly cooperation of the local communities and their leadership. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07030f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}