 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Health Research Bulletin, Vol. 9, No. 3, 2007, pp. 180-185 Placental malaria in Owerri, Imo State, south-eastern Nigeria C.N. UKAGA1*, B.E.B. NWOKE1, O.S. UDUJIH1, O.G. UDUJIH2, A.A. OHAERI1, J.C. ANOSIKE2, B.U. UDUJIH3 and M.I. NWACHUKWU1 1Department
of Animal and Environmental Biology, Imo State University, Owerri Nigeria Code Number: rb07031 Abstract Malaria in pregnancy jeopardizes the outcome of pregnancy, affecting both the mother and the foetus. The prevalence of placental malaria (PM) in women, who routinely attended ante-natal clinics in Owerri, south-eastern Nigeria, was assessed using three hospitals between March 2004 and August 2005. Placental blood was collected in EDTA bottles from incisions made on cleaned basal plate of the placenta, within an hour of delivery. Blood collected was used to assess ABO blood group, haemoglobin level as well as malaria parasitaemia. Malaria parasitaemia was determined from thick and thin smears stained with Giemsa, while the haemoglobin level was measured using the cyanomethaemoglobin method. A total of 586 pregnant women were involved in this study with written consents. Malaria parasites were observed in 175 (29.9%) of the women on delivery. Of these women, 64 (36.6%) were anaemic. A significant relationship at P<0.05 variation, was observed between the prevalence of malaria parasites in the placenta and gravidity, age and blood group. The rate of occurrence of malaria parasitaemia, in the placenta of women who were on a weekly prophylaxis against malaria is alarming and calls for more serious efforts in the prevention of malaria especially in this vulnerable group. Key words: pregnancy, placental malaria, parasitaemia, haemoglobin, prophylaxis, Nigeria Introduction Malaria caused by Plasmodium falciparum is a major health problem in many parts of the world especially in the tropical and sub-tropical countries (Greenwood & Mutabingwa 2002). Over 90% of the 200 million estimated malaria infected people in the world are in Africa (Brabin 1983). The life cycle of the malaria parasites involve phases when the parasites invade red blood cells, and produce proteins which attach themselves to receptors, in the walls of blood vessels. This causes the blood cells to accumulate in organ capillaries, resulting in life threatening symptoms. Individuals who successfully survive P. falciparum malaria episodes in childhood develop natural immunity against the parasite, and by adolescence, they are more or less protected from severe malaria illness (Miller et al., 2002). Adults in endemic areas, who had been infected several times, develop also some immunity as their defence systems gradually start to recognize the parasites' proteins. In women however, this protective immunity is lost at pregnancy due to pregnancy-induced immune-suppression (Steketee et al., 2001). When the placenta is formed, a new environment is introduced with a different set of receptors. This makes available, a new growth niche for a sub-population of the P. falciparum parasites which express an antigenically distinct form of P. falciparum erythrocyte membrane proteins (PfEMP). Multiplication of this phenotype and extensive accumulation of P. falciparum infected red blood cells (IRBC) in the placenta could lead to massive infiltrations of mononuclear cells and induction of pro-inflammatory cytokines, causing severe placental pathology (Ismail et al., 2000). Studies over the years have shown that P. falciparum erythrocyte membrane proteins (PfEMP-1) bind to a wide range of endothelial receptors, such as CD36, intercellular adhesion molecule 1 (ICAM-1), chrondroitin sulphate A (CSA), platelet endothelial cell adhesion molecule (PECAM), vascular cell adhesion molecules (VCAM), hyaluronic acid, heparin sulphate and other molecules, such as complement receptor 1, immunoglobulins G and ABO blood group antigens (Barragan et al., 2000; Beeson et al., 2000; Vogt et al., 2003; Ferreira et al., 2004). Recent studies have indicated that malaria parasites bind to three different receptors in the placenta (Scidev.net, 2006). The adherence of IRBC to the placenta is mediated by Chondroitin-Sulphate A (CSA), which is mediated by Variant Surface antigens (VSA) expressed on the surface of the IRBC (Buffert et al., 1999; Reeder et al., 1999; Maubert et al., 2000). Expression of this particular VSA by parasites binding to CSA in the placenta is thought to be the basis for the higher susceptibility of primigravidae who have little or no antibodies against the VSA to placental malaria. Studies by Ricke et al. (2000) have shown that the multigravid pregnant women from endemic areas tend to have high levels of antibodies against the VSAs expressed by CSA-adhering parasites. With the recent findings that most of the P. falciparum parasites could bind to three different receptors including hyaluronic acid in the placenta, the implication is that the production of a vaccine against the parasite in pregnancy has been made more difficult since it can no longer be based on the principle of one protein to one receptor, as was previously believed. Also important, but most frequently ignored is the role of the host’s genetic factors on the risk of placental malaria infection. The susceptibility of the host to P. falciparum infection is critical for understanding malaria in pregnancy, its consequences for the mother and the baby, as well as for improving malaria control in pregnant women. Yet there is minimal information on the role of blood group polymorphisms in pregnancy outcomes in malaria endemic areas (Loscertales & Brabin 2006). There is however increasing evidence that both the risk of acquiring P. falciparum infection and the development of severe complications are determined by host genetic factors (Fortin et al., 2002). Studies examining the effects of ABO blood group phenotype on malaria risk in non–pregnant subjects have been inconsistent (Pant et al., 1992; Pant & Srivastava 1997; Migot-Nabias et al., 2000). The blood group A has been associated with an increased risk factor in severe malaria, while the blood group O may offer some protection against severity of the disease (Barragan et al., 2000; Pathirana et al., 2005). This study, therefore, was carried out to determine the prevalence of placental malaria in women on routine prophylaxis with anti-malarial drugs, the relationship between gravidity of these pregnant women, their ABO blood groups and infection rate with P. falciparum. Materials and Methods Study area and population This study was carried out in parts of Owerri North Local Government Area (LGA) and Owerri Capital City of Imo State Nigeria. A recent study, malaria prevalence in Owerri North LGA was found to be about 68% (T.P. Okoro unpubl.). The study population were pregnant women who attended the selected routine ante-natal clinics and had their babies in the selected clinics. The women received the routine weekly preventive treatments of proguanil (paludrine) or pyrimethamine (daraprim). Written consents were obtained from the women or the spouses / close relatives of the women involved in this study. The hospitals where this study was carried out included: Federal Medical Centre, St David’s Hospital and Maternity and Holy Rosary Hospital Emekuku, in Owerri. The selected hospitals were the most frequented hospitals with very good ante-natal clinics and highly qualified gynaecologists for pregnant women. Placental blood was collected within an hour after child-birth, by incising the cleaned maternal surface (basal plate) of the placenta, and drawing 5 ml of blood welling from the incision using a sterile syringe and needle. The placental blood was kept temporarily in EDTA bottles and used for thick and thin Giemsa stained films as well as for haemoglobin and blood group estimation. The stained films were examined under a microscope using x100 objective. Parasitaemia was expressed as the number of parasites per microscope field and graded as follows: low (<1 per field), moderate (1-10 per field) and severe (>10 per field). Haemoglobin (Hb) was measured using the cyanmethaemoglobin method, and anaemia defined as an Hb level of <11g/dl (WHO, 1972). Haemoglobin levels were graded as follows: normal (>11g/dl), low anaemia (9-11 g/dl), moderate anaemia (7-8.9 g/dl) and severe anaemia (<7 g/dl). The blood groups were determined using agglutination method. Results A total of 586 women were involved in the study. P. falciparum parasites were found in the placenta of 175 women (29.9%) (Table 1) Table 1: Gravidity of the study population, number and percent infected
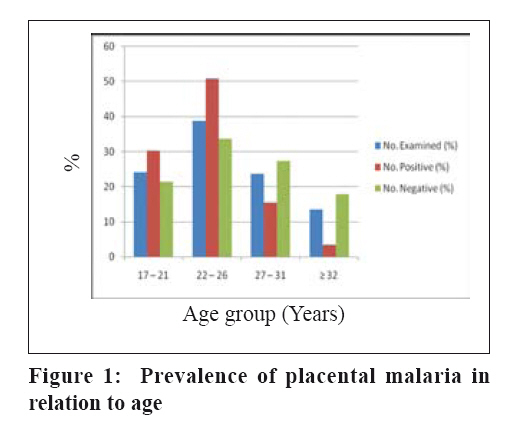
The primigravids were the largest group sampled and were the most infected. Multigravids were the least infected (4.9%), followed by the secundigravidae (9.6%) and primigravidae (15.4%) There as a significant relationship (X2= 18.403) between gravidity and presence of P. falciparum in the placenta. The relationship between age of the pregnant women and the presence of P. falciparum indicative of placental malaria is shown on Figure 1. P. falciparum in the placenta was found to have occurred most (142; 81.1%) in the age groups 17-26 years old, where incidentally, most of the study population (368; 62.8%) belonged to. A significant relationship was observed using Chi-square analysis between the age of the women in the study population and placental malaria (X2 = 39.446). The younger women appeared more vulnerable to placental malaria than their older counterparts. The determination of the different blood groups of the women under study was done to ascertain a possible relationship between blood groups and the prevalence of placental malaria (Table 2). Table 2: Prevalence of placental malaria in relation to blood groups
The blood group O+ was the most predominant and recorded the highest number of cases of placental malaria (63.4%) (Table 3). The next highest group was the A+ blood group followed by the B+. The number of women with the negative Rhesus factor in the study population was rather small. There was however a statistically significant relationship between blood group and the prevalence of placental malaria (X2= 20.633). Table 3: Parasitaemia and anaemia in the study population
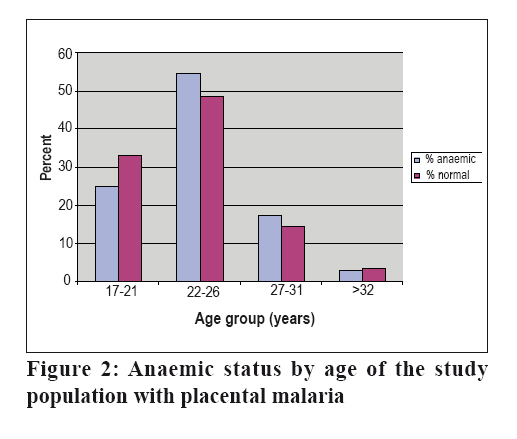
Key: w = severe anaemia; x = Moderate anaemia; y = low anaemia; z = normal Severe anaemia was found in 2 (13.3%) of the women with high P. falciparum parasitaemia in their placenta. Amongst the women with placental malaria only 15 (8.6%) were found with high parasitaemia. Most of these women (53.7%) had low parasitaemia (<1 per field)(Table 3). The women with low, moderate and severe anaemia were all classified as anaemic. This picture is made clearer by examining the anaemic state and age of the women in the study population Most of the anaemic women belonged to the 22-26 age group (Figure 2). This age group also had the most of the non-anaemic group. A significant relationship between the age of the women and anaemia was not observed. Anaemia was found to be related to the level of parasitaemia (Table 3). Discussion In areas of stable transmission, where women have developed acquired malaria immunity, malaria during pregnancy often does not cause symptomatic infections, although it increases the risk for maternal anaemia or death, as well as low birth weight (Ordi et al. 1998; Menendez et al., 2000). Placental malaria prevalence found among women who were asymptomatic for malaria and who lived supposedly in Owerri, with access to the relatively best medical services in the State is alarming. This result is an indication of the picture that would be found in the poor villages where the pregnant women have neither the medical facilities nor the medics to attend to them and are very much dependent on the village health attendants or traditional birth attendants most of whom had no formal training. Many women lose their lives during pregnancy from malarial complications in the remote villages and many babies die also (allAfrica.com 2006). It has been established that around 100,000 infant deaths occur annually in malaria endemic areas in Africa due to pregnancy associated malaria (Guyatt & Snow 2004). In these areas, primigravidae have higher prevalence of placental malaria and its associated complications (McGregor et al., 1983; Steketee et al., 1996). The malaria interventions for pregnant women often fail to reach the target women in the remote villages and when they do are not well utilized because of lack of appropriate information on how to use them as well as their importance. The results of this study are in line with other studies that the primigravids are the most afflicted by placental malaria. Studies have shown that in malaria endemic areas, such as in the study area, the increased risk of P. falciparum infection during pregnancy, which is associated with placental parasitaemia, imposes a heavy burden on the health of mothers and newborns, contributing to maternal anaemia, low birth weight and infant mortality especially among the primigravidae (Brabin et al., 2001; Guyatt & Snow, 2004; Loscertales & Brabin, 2006). Age of the women was significant for placental malaria infection. Age in the study by Zhou et al. (2002) was found to be a major risk factor in younger women aged ≤20 years of age, who were 1.8 and 3.4 times more likely to have malaria than older ones. This is in line with the findings from this study. The results from the ABO blood groups of the women afflicted with placental malaria showed an interesting pattern with the O blood type being the most afflicted. Blood group O has been associated with an increased prevalence of active placental infection as was found in this study, in the primigravidae, with a reduced risk of placental malaria in multigravidae (Loscertales & Brabin, 2006). Studies have shown that the blood group A has been implicated as a risk factor in severe clinical malaria (Fischer & Boone, 1998) in non-pregnant women while in this group, the blood group O individuals have been associated with reduced prevalence of severe clinical malaria (Fischer & Boone, 1998; Barragan et al., 2000). In conclusion, placental malaria as was found in this study is related to gravidity, age and blood group, while anaemia was found to be related to parasitaemia. There is need to ensure that malaria interventions such as insecticide treated mosquito nets as well as intermittent preventive treatments using the sulfadoxine-pyrimethamine for malaria during pregnancy is made available to the women in the remote areas who are most in need of these interventions in order to reduce mortality due to placental malaria. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07031f2.jpg] [rb07031f1.jpg] | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||

{kind=link}
{kind=link}