 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Health Research Bulletin, Vol. 9, No. 3, 2007, pp. 186-189 Antimicrobial susceptibility of Shigella flexneri and S. dysenteriae isolated from stool specimens of patients with bloody diarrhoea in Mwanza, Tanzania M.M. TEMU*, G.M. KAATANO, N.D. MIYAYE, S.N. BUHALATA, M-L. SHUSHU, C. KISHAMAWE and J.M. CHANGALUCHA National
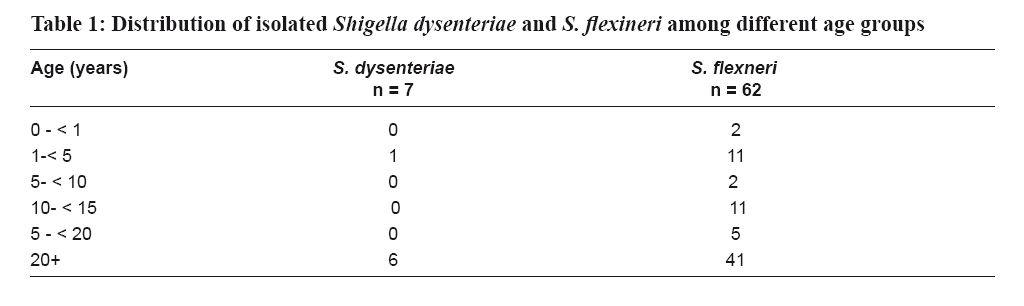
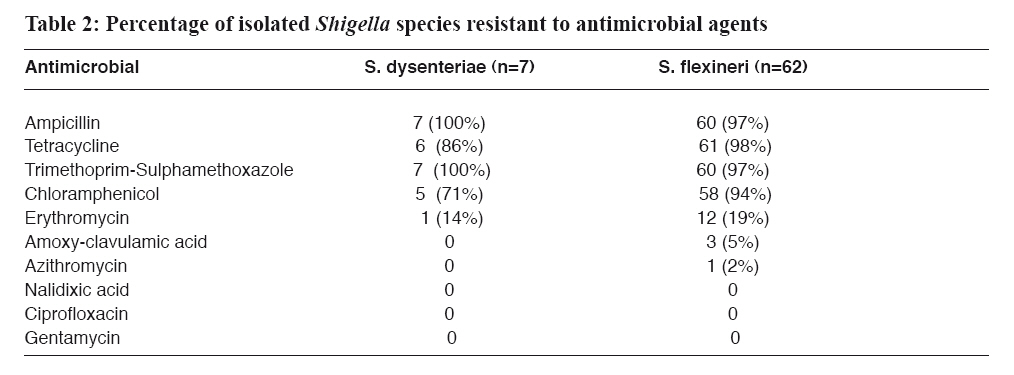
Institute for Medical Research, Mwanza Research Centre, P.O Box 1462, Mwanza, Tanzania Code Number: rb07032 Abstract This study was conducted to determine frequency and pattern of antimicrobial susceptibility of Shigella species isolated from stool specimens collected from patients presenting with bloody diarrhoea in Mwanza City, Tanzania. The study was carried out from October 2004 to October 2005 and involved patients attending Sekou Toure Regional Hospital and Butimba Health Centre. Bacteriological cultures were done at the National Institute for Medical Research laboratory. A total of 489 patients (median age= 20 years) participated in the study and were able to provide stool specimens. Shigella species were isolated from 14% (69/489) of the stool specimens collected. Of the sixty nine strains of Shigella spp isolated, 62 (90%) were S. flexneri and 7 (10%) were S. dysenteriae. All Shigella strains isolated showed high resistance to ampicillin, tetracycline, trimethoprim-sulphamethoxazole and chloramphenicol, drugs commonly used for management of shigellosis in Tanzania. However all isolates were fully susceptible to ciprofloxacin, nalidixic acid, erythromycin, cefuroxime and gentamycin. S. flexneri showed resistance to amoxy-clavulanicacid and azithromycin in 5% and 2% of isolates, respectively. None of the S. dysenteriae isolates were resistant to these two drugs. Entamoeba histolytica, Giardia lamblia and Schistosoma mansoni were microscopically detected in 16.5%, 4.4% and 5.3 % of patients, respectively These findings suggest that there is a need to carry out extensive susceptibility studies in different parts of the country with view of re-appraising the current guidelines for management of bloody diarrhoea in Tanzania. Keywords: patients, diarrhoea, Shigella species, antimicrobial susceptibility, Tanzania Introduction Diarrhoealdiseases account for approximately 25% of all deaths in < 5 years old children in developing countries (Sack et al, 1997). Infectionscaused by Shigella species are an important cause of diarrhoealdiseases in both developing and developed countries. Shigella species are members of the family Enterobacteriaceae, classified on the basis of biochemical and serological characteristics, namely; Shigella dysenteriae (group A), Shigella flexneri (group B), Shigella boydii (group C) and Shigella sonnei (Group D). Shigella species are transmitted by ingestion of contaminated food, water or through person to person contact (WHO, 2001). Flies especially Musca domestica, are also considered to play an important role in the spread of Shigella (Dupont et al., 1989). Dysentery is characterized by blood, pus and mucus in stools which indicates colorectal inflammation (Kausar et al., 1998). Shigella flexneri and S. sonnei can survive in linen for 9 – 46 days, in water for up to six months and in various foods from three weeks to six months (Moyenuddin et al., 1987). Worldwide,it is estimated that shigellosis causes around 600,000 deathsper year, two-thirds of these occurring in children under 10 yearsof age. S. dysenteriae and S. flexneri are the predominantspecies in the tropics, while S. sonnei is predominantin industrialized countries(Preston & Borczyk,1994). Shigellosis is one of diarrhoeal diseases for which antimicrobial therapy is effective and beneficial. However, antimicrobial resistance by enteric pathogens is of major concern because of indiscriminate use of antimicrobials (Navia et al., 1999). Available evidence suggests that members of this genus could develop resistance to any antimicrobial agent if used intensively (Tauxe et al., 1990). Thus, Shigella species like any other bacteria have progressively developed resistance to antimicrobials over time and this has become a challenge in the management of shigellosis (Sack et al., 1997). Currently there is limited knowledge on susceptibility pattern of Shigella species to commonly used antimicrobials in Tanzania. This information is necessary in order to re-appraise current dysentery management guidelines. This study was therefore, was conducted to determine the frequency and susceptibility of Shigella spp isolated from stool specimens collected from patients presenting with bloody diarrhoea at selected health facilities in Mwanza City, Tanzania. Materials and Methods Study area and population This study was conducted at Sekou-Toure Regional Hospital and Butimba Health Centre in Mwanza City, Tanzania between October 2004 and October 2005. Mwanza City has seen a rapid increase in population size in recent years. The inadequate and poor infrastructure for waste disposal provides favourable conditions for the spread and outbreak of diarrhoeal diseases. The main occupation of the people in the city includes business, commercial fishing, textile industry, and employment in both public and private sectors. Parasitological and bacteriological procedures Patients (children and adults) presenting with bloody diarrhoea at the two health facilities were recruited into the study after obtaining informed consent. Patients who consented to participate had demographic information recorded on study forms and were requested to provide a stool specimen. Immediately after obtaining stool at the recruiting centres a portion of it was examined microscopically for trophozoites or cysts of Entamoeba histolytica, and Giardia lamblia, and Schistosoma mansoni ova. The remaining stool specimens were transported in a Cary-Blair transport medium to the bacteriology laboratory of the National Institute for Medical Research in Mwanza for culture. For optimal isolation of Shigella and Salmonella species three different media and an enrichment medium were used. Stool specimens were inoculated onto MacConkey (MAC) agar, xylose-lysine deoxychocolate (XLD) agar and salmonella-shigella (SS) agar and incubated at 370C overnight. Enrichment was done in Selenite F broth and incubated at 370C overnight. Sub-cultures from selenite F broth were made on MAC, XLD and SS media and were incubated at 370C overnight. Blood free selective (BFS) medium was used for the isolation of Campylobacterand incubation was done in a micro-aerobic atmosphere at 420C for 48-96 hours. Identification of isolates Colonies resembling non-lactose fermenting bacteria (Salmonella or Shigella spp) were identified biochemically by the following media and tests: Fermentation of sugars, Kligler’s iron agar, mortility-indole-urea agar and SIM. Campylobacter was identified by growth on BFS medium at microaerophilic condition, growth at 420C, its positive oxidase reactions and negative Gram- staining. Salmonella spp were confirmed by agglutination test with polyvalent antisera and Shigella isolates were serogrouped by the slide agglutination test using commercially available polyvalent O antisera for S. dysenteriae, S. flexneri, S. boydii and S. sonnei. Drug susceptibility test Antimicrobial susceptibility tests were performed by the Stokes comparative disk diffusion technique. Zones of inhibition were measured in millimetres using a vernier calliper and results were interpreted according to National Committee for Clinical Laboratory Standards (NCCL) recommendations. The antibiotic discs (Oxoid Limited, Basingstoke Hampshire England) were ampicillin (30µg), tetracycline (30µg), chloramphenicol (30µg), trimethoprim-sulphamethoxazole (25µg), nalidixic acid (30µg), ciprofloxacin (5µg), amoxy-clavulamic acid (30µg), erythromycin (15µg), gentamycin (10µg), cefuroxime (30µg), and azithromycin (15µg). The control organism was E. coli ATCC 35218 (supplied by Remel Europe Limited Dart ford, Kent DA2 6PT UK). Ethical consideration Scientific and Ethics approval for the study was obtained from the Medical Research Coordinating Committee of the National Institute for Medical Research. Results A total of 489 patients participated in the study and were able to provide stool specimens. The age range of participants was 2 months to 85 years and median was 20 years (Table 1). The majority of patients (62.4%) were ≥10 years old. Twenty-seven percent of the subjects were inpatients and the rest were outpatients. Shigella species were isolated in 8.7% of patients aged <10 years and in 17.0% of those aged ≥10 years. E. histolytica, G .lamblia and S. mansoni were microscopically detected in 16.5%, 4.4% and 5.3% of the patients, respectively. Salmonella and Campylobacter species were isolated from 0.8% and 0.6% of stool specimens, respectively. Overall, Shigella species were isolated from 14% (69/489) of the patients with bloody diarrhoea. Of the 69 isolates, Shigella flexneri were 62 (90%) and S. dysenteriae were 7 (10%). All Shigella isolates showed high degree of resistance to ampicillin, tetracycline, trimethoprim-sulphamethoxazole and chloramphenicol, drugs commonly used in the management of shigellosis in Tanzania. All isolates were fully susceptible to ciprofloxacin, nalidixic acid, erythromycin, cefuroxime and gentamycin (Table 2). Five and two percent of S. flexneri isolates were resistant to amoxy-clavulanic acid and azithromycin, respectively. None of the S. dysenteriae isolates were resistant to these two drugs. Discussion Shigella species were the dominant bacteria isolated among patients presenting with bloody diarrhoea in Mwanza City. This is similar to observations made from other studies in Africa and Asia (Sack et al., 1997; DeMol et al., 1978). S. flexneri and S. dysenteriae are thought to be predominant Shigella species in the developing world. In this study S. flexneri was more frequently isolate than S. dysenteriae. These results are similar to those reported from elsewhere (Paton et al., 1991); suggesting that that both Shigella species and E. histolytica are likely to be the major aetiologies of bloody diarrhoea in Mwanza City, Tanzania. In this study antimicrobial susceptibility testing showed a high degree of resistance to the easily available and affordable antibiotics, namely tetracycline,ampicillin, co-trimoxazole, and chloramphenicol. Similar observations have been reported from south-east Tanzania (Navia et al., 1999). The drugs to which the Shigella species were fully susceptible are expensive and not easily available. In the present work Shigella strains isolated from patients with bloody diarrhoea were sensitive to nalidixic acid and rarely susceptible to ampicillin and co-trimoxazole which is also similar to the results of other studies (Donald et al., 1985; Bennish et al., 1985). However, the use of quinolones in children, in whom bacillary dysentery most commonly occurs, is not recommended because of evidence of cartilage toxicity (Shaukat et al., 1998). The spread of multi-resistant Shigella strains among a population in which the diarrhoeal diseases are among the major cause of child morbidity and mortality requires greater attention to the appropriate use of antibiotics, the establishment of hygienic measures to prevent or decrease transmission and development of new effective drugs that can be safely used by children. Moreover the guidelines for the treatment of shigellosis in developing countries, including Tanzania, should be updated since in this study co-trimoxazole, one of the recommended antimicrobial agents for the treatment of shigellosis have shown to be ineffective against Shigella species. In many places of Tanzania, home and self medication and purchase of drugs without prescription are common practices (Nsimba et al., 2002). It is very possible that the misuse of drugs might have contributed to the observed antibiotic multi-resistant Shigella strains. In conclusion, antibiotic resistance in Shigella infections should be of great concern to clinicians and public health authorities. Additional data about multiple drug resistance of Shigella strains are epidemiologically significant for planning shigellosis control strategies in Tanzania. It is therefore, recommended to establish an antimicrobial surveillance system to monitor the distribution and resistance patterns of Shigella species over time and in the different regions of Tanzania. Acknowledgements We thank all patients who agreed to participate in this study. We also thank staff of Sekou-Toure Hospital and Butimba Health Centre for the enthusiasm and technical assistance. This study received financial assistance from the Ministry of Health and Social Welfare, Tanzania. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07032t2.jpg] [rb07032t1.jpg] |
| |||||||||

{kind=link}
{kind=link}