 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Tanzania Health Research Bulletin, Vol. 9, No. 3, 2007, pp. 202 - 206 Suicidal ideation and associated factors among in-school adolescents in Zambia A.S. MUULA1, L.N KAZEMBE2, E. RUDATSIKIRA3 and S. SIZIYA4* 1Department
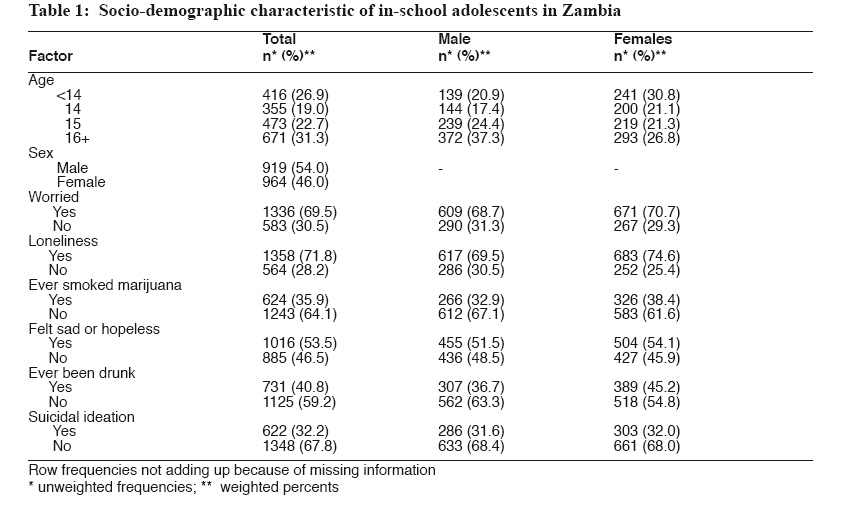
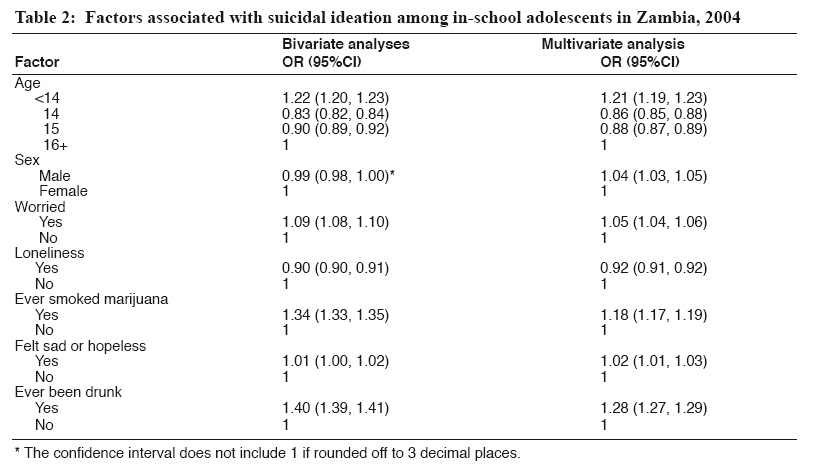
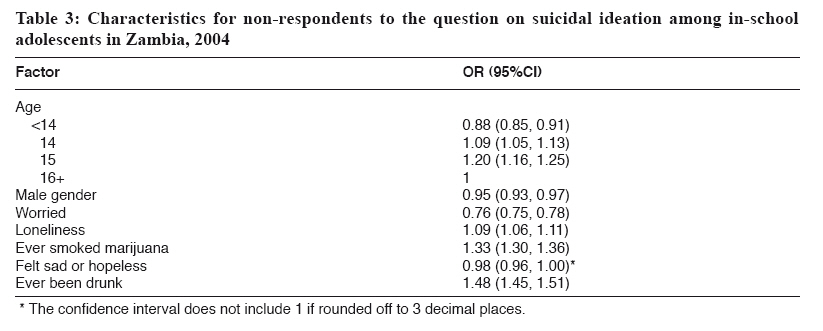
of Community Health, College of Medicine, University of Malawi, Blantyre, Malawi Code Number: rb07035 Abstract A cross sectional study was conducted to estimate the prevalence and correlates of suicidal ideation among in-school adolescents in Zambia. Backward logistic regression analysis was conducted to assess the association between relevant predictor variables and suicidal ideation within the last 12 months. A total of 1970 in-school adolescents who participated in the Zambia Global School-Based Health Survey in 2004 responded to the question on suicidal ideation. Overall, 54.0% were males, 40.8% were current drinkers, and 35.9% ever smoked marijuana (cannabis). Altogether 31.3% reported suicidal ideation in the past 12 months (males= 31.1%; females= 31.4%). Being male (OR=1.05; 95%CI 1.03, 1.05); being <14 years old (OR=1.21; 95%CI 1.19, 1.23), having been drunk (OR=1.28; 95%CI 1.27, 1.29), worried (OR=1.05; 95%CI 1.04, 1.06), sad or hopeless in the past 12 months (OR=1.02; 95%CI 1.01, 1.03) and ever used marijuana (OR=1.18; 95%CI 1.17, 1.19) were positively associated with suicidal ideation. Loneliness appeared to be protective (OR= 0.92; 95%CI 0.91, 0.92). All the results, except for ever smoked marijuana and ever been drunk, may have been biased due to non-response to the question on suicidal ideation. A series of cross sectional studies should be conducted to monitor changes in behavioural factors among others ever smoked marijuana and ever been drunk in order to broaden our understanding of factors that may be causing adolescents to seriously consider committing suicide. Keywords: Zambia, suicidal ideation, illicit drugs, alcohol, burden of disease Introduction Adolescent mental health is a neglected but increasing public health issue in developing countries, including Zambia. It has been estimated that HIV and AIDS, ischaemic heart disease and mental disorders will be the three leading causes of burden of disease in the world by 2030 (Mather & Loncar, 2006). In 2001 mental disorders were among the ten leading causes of deaths globally (Lopez et al., 2006). Suicide is responsible for about one million deaths annually in the World (National Center for Injury Prevention and Control, 2002). In the United States, for instance, suicide contributes to unintentional injury deaths among adolescents having been reported at a rate of 4.5/100,000 adolescents (10 to 19 years old) between 1999 and 2002 (Bernard et al., 2007). Despite the huge burden that mental health exacts on global burden of disease, it still remains a neglected area of research especially in Africa where greater emphasis and effort is directed towards infectious diseases such as tuberculosis, malaria and HIV and AIDS. Moreover, information on suicidal behaviour, including ideation, attempts and completed suicides in Africa is lacking. Although not all suicidal ideation materialize into suicide attempts or suicide, it is the first step on the path to suicide. While there have been reports on the prevalence and correlates of suicidal ideation in the developed world (Vinas et al., 2002; Joe et al., 2006), data from the developing world are limited. We therefore carried out this study to estimate the prevalence and assess socio-demographic correlates among in-school adolescents in Zambia. We believe such information is useful in understanding the burden of mental health to adolescent health. This information may also be useful in targeting scarce public health resources in the provision of intervention that may reduce the occurrence of suicide in Zambia. Materials and Methods The study involved secondary analysis of data from the Zambia Global School-Based Health Survey (GSHS) conducted in 2004. The GSHS was developed by the World Health Organization (WHO) in collaboration with UNICEF, UNESCO, and UNAIDS with technical assistance from the Centres for Diseases Control and Prevention, Atlanta, Georgia, United States. The purpose of the survey was to provide data on health and social behaviours among in-school adolescents aged 13 to 15 years. In the Zambia GSHS, students from grades 7 to 10 were recruited. A total of 3021 in-school adolescents were eligible to participate in the survey but only 2257 eventually participated, giving a response rate of 75%. The GSHS used a two-stage probability sampling technique. In the first stage of sampling, the primary sampling units were schools and these were selected with a probability proportional to their enrolment size. In the second step of sampling, a systematic sample of classes in the selected schools was obtained. All students in the selected classes were eligible to participate regardless of their age. A self-completed questionnaire was used and study participants completed the questionnaire within one class period. Students were encouraged to answer all questions but also told that they were free not to answer any question they felt uncomfortable with. Trained research assistants supervised the process. Study participants were asked their age, gender and the following questions: During the past 12 months, how often have you felt lonely? During the past 12 months, how often have you been so worried about something that you could not sleep at night? During the past 12 months, did you ever seriously consider attempting suicide? During the past 12 months, did you ever feel so sad or hopeless almost everyday for two weeks or more in a row that you stopped doing usual activities? During your life, how many times have you smoked marijuana? During your life, how many times did you drink so much alcohol that you were really drunk? Data analysis The main outcome variable was history of suicidal ideation in the past 12 months defined as having responded yes to the question: During the past 12 months, did you ever seriously consider attempting suicide? All predictor variables were reduced to binary variables in which >1 in response to any of the questions was coded 1, and 0 otherwise. Considering the design of the study a weighting factor was used in the analysis to reflect the likelihood of sampling each student and to reduce bias by compensating for differing patterns of non response. The weight used for estimation is given by the following formula: W= W1*W2*f1*f2*f3*f4 Where: W1 = the inverse of the probability of selecting the school We obtained frequencies as estimations of prevalence rates of factors. A Backward logistic regression analysis using SPSS version 11.5 was conducted to assess the associations between relevant predictor variables and suicidal ideation within the last 12 months. We report both unadjusted and adjusted odds ratios for selected predictor variables while suicidal ideation as the dependent variable. Results A total of 2257 in-school adolescents participated in the Zambian Global School-Based Health Survey in 2004. Of the 2257 adolescents in the survey, 1970 responded to the question on suicidal ideation. Among the respondents, 54.0% were males, 40.8% had ever been drunk, and 35.9% had ever smoked marijuana. Most respondents, 37.3% males were of age 16 years or more and 30.8% females were of age less than 14 years (Table 1) Overall 31.3% (males=31.1%; females= 31.4%) reported suicidal ideation in the past 12 months. All the significant factors in bivariate analyses remained significant in a multivariate analysis (Table 2). Reported life-time experience of being drunk (OR=1.28; 95%CI 1.27, 1.29) or smoking marijuana (OR=1.18; 95%CI 1.17, 1.19) were positively associated with suicidal ideation. Furthermore, being <14 years old (OR=1.21; 95%CI 1.19, 1.23), reporting being worried that could not sleep at night (OR=1.05; 95%CI 1.04, 1.06), and even feeling sad or hopeless that stopped doing usual activities (OR=1.02; 95%CI 1.01, 1.03) were positively associated with suicidal ideation. Gender was not associated with suicidal ideation, while having felt lonely (OR=0.92; 95%CI 0.91, 0.92) was negatively associated with the outcome. A total of 166 adolescents did not respond to the question on suicidal ideation. Non-respondents tended to be older than 13 years, females, not worried, lonely, ever smoked marijuana, not to have felt sad or hopeless and ever been drunk (Table 3). Discussion Our study found the 12 months prevalence of suicidal ideation among in-school adolescents in Zambia in 2004 of 32.2%. The prevalence of suicidal ideation among males and females was similar. Male adolescents who reported being worried, reported smoking marijuana or having been drunk, and those that sadness and hopeless interfered with functioning were more likely to have reported suicidal ideation. Interestingly, loneliness was protective. The 12 months prevalence of suicidal ideation found in the current study of was much higher than that reported by Liu et al. (2005) among Chinese adolescents (19.3%). However the difference with the Chinese study was that study participants were asked to report 6 months suicidal ideation while in our study participants were asked for a much longer time of 12 months. It is not known whether our prevalence and the Chinese study would have been comparable had the period of recall been the same. The finding that males were more likely to have seriously considered committing suicide than females contradicts the results obtained by Liu et al. (2005) who reported a higher prevalence of suicidal ideation among females compared to males (22.0% vs. 17.5%). Similar findings of female predominance were also reported by Ovuga et al. (2005) in Uganda. In South Africa, it has been reported that the majority of callers to a suicide toll free phone hotline were female adolescents (Meehan & Broom, 2007). In a study comprising 45 patients in Namibia, 53% of patients who had committed suicide or para-suicide were females (Ikealumba & Couper, 2006). Globally however actual suicide deaths occur more among males than females (Holder et al., 2001), and this finding accords our result from the multivariate analysis which was adjusted for possible confounding factors. We found that marijuana use and having been drunk were associated with suicidal ideation. This finding corroborates findings reported from United States (Burge et al., 1995) that alcohol or cannabis use was positively associated with suicidal ideation among high school students. Although these associations exists, it is not possible in a cross sectional study to ascribe causation. It may be possible that adolescents who are likely to experience suicidal ideation were more likely to self-medicate with alcohol and cannabis (Lynskey et al., 2002). However, Bovasso (2001) and Roberts & Chen (1995) have reported that cannabis abuse is a risk factor for major depressive disorders. We also observed that adolescents who reported being sad or worried were more likely to have experienced suicidal ideation. Surprisingly we found that adolescents who reported being lonely were less likely to have experienced suicidal ideation. Stravynski & Boyer (2001) have previously reported on the association between suicidal ideation and loneliness. Adolescents <14 years were more likely to have seriously considered committing suicide. This finding is different from Liu et al. (2005) who found increasing age to be correlated with suicidal behaviour. We do not know why younger study participants reported higher likelihood of suicidal ideation. It is possible though that younger participants may not have developed problem solving skills and as such were more likely to consider committing suicide than older peers. Differences in the above findings may be as a result of our finding being biased due to non-response. This study was based on data collected in a cross-sectional survey and relied on recall of information over a period of 12 months. Due to the cross sectional nature of the design, we cannot determine the causal relationships between the identified factors and adolescent suicidal ideation. As the data were dependent on recall, it is possible there may have been misreporting due to inability to recall or deliberate or intentional misreporting. In order to minimize intentional misreporting questionnaires were self-completed anonymously. Questionnaires were also completed under the supervision of trained research assistants and not the class teachers. However accurate reporting cannot be guaranteed even with the assurance of confidentiality. Furthermore, the results from this study may not be applicable to out of school adolescents. In conclusion, we have estimated a 12 months prevalence rate of suicidal ideation among adolescents of 31.3%. We suggest that a series of cross sectional studies be conducted to monitor changes in behavioural factors among others ever smoked marijuana and ever been drunk in order to broaden our understanding of factors that may be causing adolescents to seriously consider committing suicide.. Acknowledgements We are grateful to the students who participated in the Zambia Global School-Based Health Survey (GSHS). We also thank the Zambian Ministries of Health and Education, the Center for Disease Control and Prevention (Atlanta, Georgia, United States) and the World Health Organisation, Afro Region for permission to conduct the study, funding for data collection and other logistical support. References
Copyright 2007 - Health User's Trust Fund (HRUTF) The following images related to this document are available:Photo images[rb07035t1.jpg] [rb07035t3.jpg] [rb07035t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}