 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Revista Colombia Médica, Vol. 38, No. 3 , Jul./Sep. 2007, pp. 191-196 Sexual intercourse among adolescent students of Santa Marta, Colombia: a cross-sectional survey* Relaciones sexuales en adolescentes escolarizados de Santa Marta, Colombia: una encuesta transversal Guillermo Augusto Ceballos, Psicol.1, Adalberto Campo-Arias, M.D.2 * This study was financed by Fonciencias, University of Magdalena and the Autonomous University of Bucaramanga (Agreement 030, 2006).
1. Profesor Auxiliar Ocasional, Grupo de Estudio del Suicidio y Conductas de Riesgo Sexual, Universidad del Magdalena, Santa Marta, Colombia. e-mail: gceballos@unimagdalena.edu.co
Recibido para publicación abril 18, 2007 Code Number: rc07041 SUMMARY
Background: Among teenagers, the prevalence of sexual intercourse
(SI) varies from one country to another, and within the same country- from region
to region. Information regarding SI in teenagers is unknown for a representative
portion of students in Santa Marta, Colombia. Keywords: Sexual behavior; Prevalence; Students; Adolescents; Cross-sectional study. RESUMEN
Antecedentes: La prevalencia de relaciones sexuales (RS) en adolescentes varía de un país a otro e, incluso, dentro del mismo país, de una región a otra. No se conoce esta información
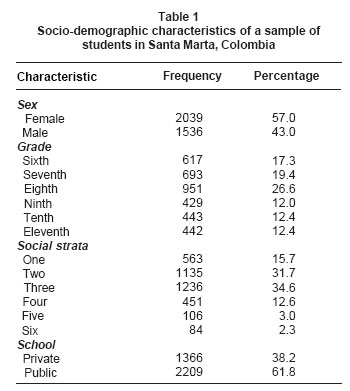
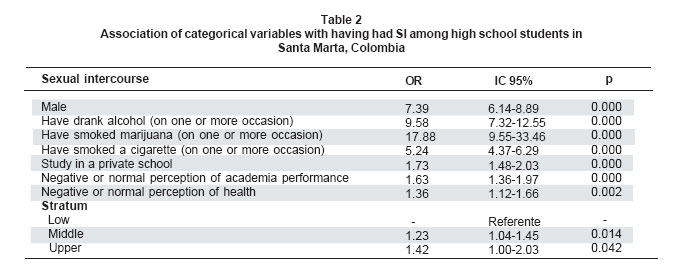
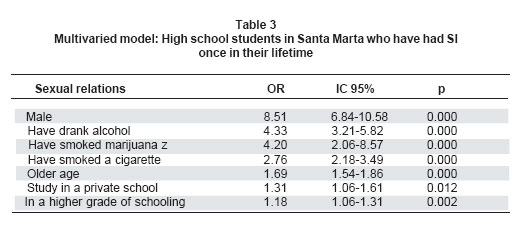
en una muestra representativa de estudiantes de Santa Marta, Colombia Palabras clave: Relaciones sexuales; Prevalencia; Estudiantes; Adolescentes; Estudios transversales. In the past few decades, studies on sexual relations (SR) in adolescents have been numerous due to the proliferation of un-planned pregnancies and sexually transmitted diseases (STDs), including HIV and AIDS, an epidemic that affects the youngest groups of the population (1,2). The age of first sexual encounter varies between different countries, ranging from 15 to 19 years (3-5). However, some studies indicate earlier ages for first SI (6,7). It goes without saying that amongst adolescent students, the greater the age, the greater the probability of having had SI (8-10). In Colombia and in Latin America, women experience first SI at a later age than their male counterparts (3). The prevalence of SI in relation to class grade varies from study to study, however, all agree that the higher the class grade, the greater the prevalence (11-13). The same can be said of the socio-economic status of the parents, some studies demonstrate a link between lower socio-economic strata and a higher prevalence of sexual intercourse (14-16) while others note no relation between the two (17). Very few studies have drawn an association between the type of school (private or public) to having had SI (7). Nevertheless, results are contradictory, since one study found that students studying in private schools had their first SR at a later age (18); while another investigation indicated that studying in public or private school did not influence the age of first SR (6). Adolescence is also the stage of the life when people are most at risk of participating in the consumption of legal and illegal substances (19,29). Studies show a positive association between consumption of substances, both legal and illegal, and having had SI (7,9,10,21-23). In Santa Marta, Colombia, two studies have shown that approximately 25% of the adolescent students affirmed to having had SI. It was documented that having had SI was linked to being male, being older, being in an upper grade of schooling, smoking and consuming alcohol; studying at public or private school was seen to be irrelevant. However, these studies were carried out on relatively small stratified samples taken at convenience (24,25). The general aim of the study was to determine the prevalence of SI and relating factors such as age, sex, grade of schooling, type of school (public or private) and consumption of legal and illegal substances in a random sample of students in Santa Marta, Colombia. METHOD This cross-sectional study was conducted with the permission of the directors of the chosen schools, the parents/guardians and the participating students. The objectives of the study and the low risk involved were explained, participation was entirely voluntary and complete anonymity was guaranteed (26,27). A random sample of schools was conducted, so that all secondary schools in the District of Santa Marta had the same chance of being selected, be they public or private, urban or rural. The participants filled in the surveys in private. The surveys were composed of 30 questions relating to: socio-demographic aspects, sexual conduct and health. The type of questionnaire used has proved to be very reliable when surveying adolescents in other countries (28). In the present study the dependent variable was having had SI, and the independent variables took into account: age, sex, grade of schooling, type of school (public or private) and consumption of legal and illegal substances. The data were analyzed using the program statistical package for social sciences (SPSS 13.0) (29). Appropriate statistical measures were taken for every type of variable (qualitative or quantitative), when it was necessary confidence intervals of 95% (IC 95%) were established. In the bivariate analysis, reasons for disparity (OR) were determined at IC 95%. The multivariate analysis was conducted by means of logistic regression in accordance with Greenland’s recommendations (30). Probabilities of less than 5% were taken to be of significant difference. RESULTS A total of 4000 students took part in the survey. A group of 425 of the questionnaires were dismissed: 187 (47%) due to incompletion and 238 (6.9%) due to inconsistencies. This report is based on 3,575 complete and consistent questionnaires. The age of the group ranged from 9 to 20 years old, with an average of 13.6 years (SD=1.9). Students of all grades took part, with an average of 8.2 years of schooling (SD=1.6). Other socio-demographic characteristics appear in Table 1. Among students 804 (22.5 %) answered affirmatively to having had SI once in their lifetime. The age of first SI ranged between 7 and 18 years, with an average of 13.3 years (SD=1.8), with a median and mode of 13 years. The number of sexual partners in a lifetime was between 1 and 20, with an average of 2.9 partners (SD=3.3), a median of 2 partners and a mode of 1 partner. In the bivariate analysis, students who affirmed to having had SI had an average age of 14.8 years (SD=1.7) compared to those who denied it, who had an average of 13.3 years (SD=1.9) (t=21.5; lg=3573; p=0.000). The students who affirmed to having SI showed on average a schooling of 8.9 years (SD=1.4) compared to those who denied it, 8.0 years (SD=1.6) (t=14.9; lg=3573; p=0.000). The associations with categorical variables appear in Table 2. In order to avoid possible confusion within the results, a multivariate model was used by means of logistic regression. In the final model the variables of perception of health, perception of academic performance and social stratum were excluded as they bore no significant influence and they did not produce a variation greater than 10% in the closest of associations. The model is given in Table 3. DISCUSSION The investigation shows that 22.5 % of adolescent middle- and high school students of Santa Marta have had SI in their life. Having had SI was associated with being male, being older, being in an upper grade of schooling, studying at a private school and having unhealthy habits; consumption of alcohol, cigarettes and cannabis. The study reports that approximately one in every four students has had SI. Similar results were found in stratified sampling in Santa Marta (24,25) and among students of a public school in Bucaramanga (9). Nevertheless, it is significantly less than the 33 % of students (from grades 9-11) from several public schools in Barranquilla (31) and the 58% of high school and university students of Bucaramanga (32) who have had SI. The prevalence of SI amongst adolescents varies considerably, for example, in Japan 20% (22), in Nigeria 34 % (14), in Ecuador 43% (12), in Switzerland 45% (33), in USA 22% to 52% (34-36), among African Americans and Hispanics 41%37. Results recorded in Chile and Mexico regarding SI amongst adolescents diverge from the aforementioned results at 11% (11) and 18.4%, respectively (13). These differences can be attributed to inherent social and cultural factors of the population studied (38). As in the present study, a large number of studies at both national and international level indicate that, in general, male adolescents affirm more frequently to having SI than female adolescents (3-5,7-10,13-15,24,25,32). This can be attributed to power relations that arise in a society of double moral standards (with regards to sex), namely in the different sexual freedoms and rights assigned to men and women, tacitly giving rise to sexual activity in boys and abstinence in girls. However, the existing differences with respect to gender tend to disappear at approximately 24 years of age (21). This study concurs with other studies indicating that the greater the age the more likely that an adolescent will have had SI (8,9,24,25). Equally this demonstrates that the greater the year of schooling the more probable it is that the adolescent will have had SI (11-13). This is plausible as the higher the school grade, the greater the chronological age, and the prevalence of SI increases with age (21). The study observed that the higher the socio-economic stratum the greater the probability of having had SI which supports similar information documented in previous studies (39,40). Nevertheless, another report indicates that in economically unfavourable situations the prevalence of SI is higher (23). In general it is noted that the norms of sexual behaviour, in almost all the aspects, are more flexible to those from a higher socio-economic stratum (18,41). But, in some lower-economic social strata there is an unusually high prevalence of SI which could be explained by lack of parental supervision; which indisputably plays a definitive role in social and cultural contexts (39). The data have shown that studying in a private school is a factor related to having had SI, a similar result was also documented in another study (40). Nevertheless, a greater number of studies show that having had SI is linked to studying in public schools (6,14-16,23). It is clear that public and private schools are heterogeneous in many aspects; it is much more probable that other characteristics of the population studied bear more influence (38). The given information is concurrent with other studies relating to SI, that acknowledge its close link with habits considered harmful to one’s health for example smoking cigarettes, consumption of alcohol and cannabis (7,9,19-20,22,24,25,42). Among adolescents this kind of behaviour may be considered part of the formation of personality, related to the search for new and pleasurable experiences (43). Up to this point, no link between the perception of academic performance and the perception of health to SI has been found. However, if an affiliation were to exist, it would be spurious or indirect given that it has been observed that the students who affirm to having had SI, frequently smoke cigarettes and are more likely to have drink problems. The last group of students reported a poor perception of academic achievement, possibly due to the presence of symptoms of depression (44,45). Symptoms of depression in adolescents have been related to unsafe sex practices leading to the risk of HIV and un-planned pregnancies (46-48). From the results, it is possible to see that it is necessary for Colombian organisations working in sexual health development in secondary schools, to design campaigns for the promotion of safe sex and the prevention of STIs/STDs and unplanned pregnancies with the integral plan taking gender, social and cultural aspects in to account. Furthermore, these programmes should involve students of primary age, since a significant number of children have had their first sexual encounter before entering secondary school (49,50). The present work corroborates other information observed in stratified samples of adolescent students in Santa Marta. However, due to random sampling employed, this study is invaluable as it better represents a greater number of the adolescent student population of Santa Marta, Colombia. Nevertheless, this study also presents some limitations; the cross-sectional design does not allow for the estimation of direction of causality. Also, other possible variables that can influence the sexual behaviour of adolescents were not studied, for example, the presence of symptoms of depression, religious affiliation, etc. In conclusion, approximately one in five high school students in Santa Marta has had sexual intercourse, the frequency is higher in males, in students of private schools, in students of a higher school grade, in students of higher socio-economic strata and who have unhealthy habits for example consumption of alcohol, smoking cigarettes and cannabis. It is recommend that further studies be carried out regarding the sexual behavior of adolescents not attending school, primary school students and other studies similar to this one but using other variables. ACKNOWLEDGEMENTS With special thanks to Karina Ceballos Moreno, Business Administrator, University of Magdalena for her support in data transcription. STATEMENT OF INTEREST During the period of data collection in this study, Doctor Adalberto Campo-Arias held a position at the Autonomous University of Bucaramanga. REFERENCES
© Copyright 2007 - Revista Colombia Médica The following images related to this document are available:Photo images[rc07041t3.jpg] [rc07041t2.jpg] [rc07041t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}