 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Revista Colombia Médica, Vol. 39, No. 3, Jul-Sept, 2008, pp. 227-234 Conduction between left superior pulmonary vein and left atria and atria fibrillation under cervical vagal trunk stimulation Conducción entre la vena pulmonar superior izquierda, la aurícula izquierda y la fibrilación auricular bajo el estímulo del tronco cervico-vagal Hou Yuemei, MD, PhD*, Zhang Xiaoqin, MD, PhD*, Song Jianguo, MD*, Na Jina, MD* * Cardiovascular Research Institute, First Teaching Hospital, Xinjiang Medical University, Urmuqi City, China.
Received for publication July 11, 2007 Code Number: rc08048 SUMMARY Objective: The effect
of cervical vagal trunk stimulation on conduction between left superior
pulmonary vein and left atria and atria fibrillation have not been
systematically studied. We attempted to investigate the electrical
conduction between LA and LSPV in dogs with cervical vagal trunk
stimulation and evaluate the possible underline substrates for local
reentry and initiation and maintenance of AF. Keywords: Electrical conduction; Atria fibrillation; Left atria; Left superior pulmonary; Cervical vagal trunk. RESUMEN Objetivo: El efecto del
estímulo del tronco nervioso cervico-vagal sobre la
conducción entre la vena pulmonar superior izquierda (LSPV,
siglas en inglés), la aurícula izquierda (LA, siglas en
inglés) y la fibrilación auricular (AF, siglas en
inglés), no se ha estudiado sistemáticamente. Se
intentó investigar la conducción eléctrica entre
la LA y la LSPV, con el estímulo del tronco nervioso
cervico-vagal y evaluar los posibles substratos subyacentes para la
reentrada local, la iniciación y el mantenimiento de la AF. Palabras clave: Conducción eléctrica; Fibrilación auricular; Aurícula izquierda; Vena pulmonar superior izquierda; Tronco nervioso cervico-vagal. Atria fibrillation is the most common cardiac arrhythmia, getting more prevalent with age1, and with an increased long-term risk of stroke, heart failure and all-cause motality2. The focal source hypothesis, incorporating automaticity and/or local reentry is consistent with a dominant role for the LA in human AF. Previous studies showed that ectopic beats originating from the PV propagated to the LA with characteristically long conduction time, often with conduction delay or block within the PV or at the PV-LA junction3. In canine models vagal stimulation shortens the effective atria refractory period as well as triggers and maintains AF. However, the detailed conduction patterns between LA and PV and inducibility of AF under abnormal parasysmpathetic activation are poorly understood. We hypothesized that cervical vagal trunk stimulation and fast pacing will produce abnormal conduction from LA across the PV-LA junction to PV, which will play an important role in maintains AF originating from the PV. METHOD Surgical preparations. In 12 mongrel dogs (18 to 25 kg), anesthesia was performed with sodium pentobarbital (initial bolus 25 mg/kg IV, 5-10 mg/kg as needed for maintenance, every 2 hours). Intubation and mechanical ventilation with oxygen (2 l/min) was given. Two bipolar electrode catheters were inserted through right jugular vein and femoral vein to both right atria and right ventricular for electrophysiological study. After left lateral thoracotomy, the heart was exposed in a pericardial cradle. Multielectrode catheter was placed along the left superior pulmonary vein, a quadripolar catheter in the HIS, a quadripolar catheter in the left atrial appendage (LAA), and a multielectrode catheter was inserted into the coronary sinus. Surface ECG lead II/aVR and intracardiac tracings were recorded by use of a HELLE Cardio-2000 system, filter setting ranged between 0.1 and 250 Hz, whereas bipolar electrocardiograms were filtered at 30-250 Hz. Cervical vagal trunk stimulation. For cervical vagal trunk stimulation (CVTS), an self-made bipolar silver electrodes with 2-5 mm distance was inserted into the vagosympathetic trunk in a parallel way. Electrical stimuli was delivered by X-VI type stimulator (East Electronic Company, China) at 60 ms (1000 bpm), the voltage chosen was between 1-4V. Effective CVTS stimulation response was defined as: the sinus arrest lasting >2 seconds or complete atrioventricular AV block, or a 50% reduction in heart rate was used as the definition of adequate vagal response. The effective CVTS stimulation response was kept constantly during entire experiment. Measurement of ERP, conduction and AF inducement. For measurement of ERP, conduction and inducibility of AF, a ten-polar electrode catheter was placed along LSPV, a bi-polar electrode catheter at high right atria (HRA), and a bi-polar electrode catheter at left atria appendage. The conduction sequences across PV-LA junction, within left superior pulmonary vein and the inducibility of AF were assessed before and after vagal stimulation by 60 ms (1000 bpm) continuous electrical pulse pacing at the LA, middle and distal part of LSPV in 10s, 30s and 60s different duration with 30s interval in each time. Effective refractory period (ERP) of LSPV, PV-LAj, HRA and LAA was investigated by 5 ms decremented stepwise S1S2 200 ms pulse of electrical stimulation, with voltage 1-8 V, two times diastolic threshold. AF inducibility was assessed and recorded before and after cervical vagal trunk stimulating. The AF persistent was defined as: AF induced lasting more than 5 min. AF could be stopped automatically or defibrillated by cardioversion or clamped at left atria appendage if it last more than 30 min. Statistical analysis. Results are expressed as mean ± standard deviation (SD). Statistical comparisons between groups were done with Student’s t test. An index of ERP heterogeneity for each dog was obtained by calculating the coefficient of variation of the 4 regional ERP values. All data were analyzed in software SPSS 11.5. A 2 tailed value of p<0.05 was considered statistically significant. All animal studies were approved by the Animal Use and Care Committee of Department of Animal Research Institute of Medical Center, Urumuqi City, Xinjiang. RESULTS Heart rate. The average heart rate before vagal stimulation was 156±34 bpm and 75±34 bpm during supramaximal CVTS, (p<0.05 n=12). The heart rate decreased gradually with voltage increased from 1 to 4V, while the heart rate will not be reduced any more once the maximal vagal response reached by 4v stimulating. The maximal vagal response was constant during the entire procedure without fatigue phenomenon. ERP and ERP heterogeneity. The ERP of HRA, LAA, PV-LAJ, LSPVm and LSPVd sites be shortened from baseline on average, 112.8±11.2 ms to 92.6±12.4 ms (p<0.05, n=12) during supramaximal CVTS. The ERP shortening at each site is illustrated in Table 1. Local effective refractory period (ERP) was measured and spatial heterogeneity (dispersion) between each recording sites was evaluated before and after CVTS (dispersion was calculated as the ERP difference between the maximum and minimum value of HRA, LAA, PV-LAJ, LSPVm and LSPVd distant recording sites). The overall conduction vilocity (CV) for each dog was calculated from the average of each of HRA, LAA, PV-LAJ, LSPVm and LSPVd regional CV values. An index of CV heterogeneity in each dog was obtained by calculating the coefficient of variation (COV CV=SD/mean x 100%). The heterogeneity was measured by COV-ERP was 3±3% baseline vs. 30±13%,on average, with CVTS, p<0.05; n=12). The activation sequence and electrical conduction between LA and LSPV with vagal response:
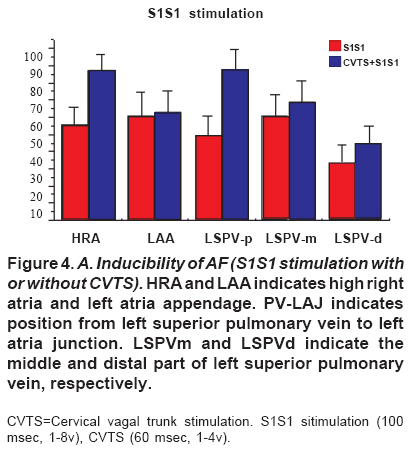
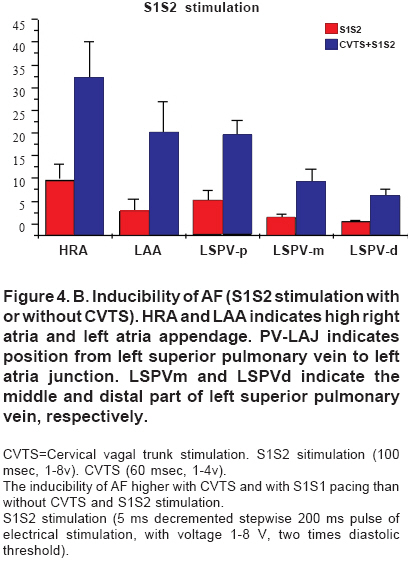
Inducibility of atria fibrillation. Spontaneous AF could not be induced by CVTS in all 12 dogs. The duration of AF induced varied from animal to animal. On average, the rate of induction of AF was baseline 49.86% with S1S1 100 ms pacing and 3.7% with S1S2 5 ms decremented stepwise pacing at HRA, LAA, LSPV. While the rate of induction of AF could be increased to 70.9% by S1S1 100 ms burst pacing and to 43.5% by S1S2 premature pacing at HRA, LAA, LSPV with vagal response (CVTS by S1S1 60 ms, 1-4V). The distal part of LSPV was the site with lower AF induction rate both at CVTS or without (Figure 4 A, B). Vagal AF usually, but not always, spontaneously converted to sinus rhythm. DISCUSSION Currently, ablation strategies for AF consist of pulmonary vein (PV)
isolation with or without additional ablation lines in the left atrium
and/or targeting the complex electrocardiograms characterized by a
short cycle length, fractionation, and/or continuous electric activity.
The reported immediate success rate is higher than 90%. The long-term
success rate ranges from 60% to 90% in patients with paroxysmal AF, but
it is lower in patients with chronic AF4-6. The
effectiveness of catheter ablation is related to the precision of the
atrial lesions created around the PV which aims to eradicate the
triggers, isolate the PV, and modify the substrate for AF maintenance.
However, these lesions create large areas of scarring in the atria that
might become a substrate for the late onset of atria tachyarrhythmias
and depress the left atria contractility7, and they may
involve more ablation than necessary in some patients. Further more,
ablation along the posterior left atrial wall is associated with the
risk of a lethal complication involving an atrioesophageal fistul8. Therefore, new techniques for the ablation of AF are continually evolving.
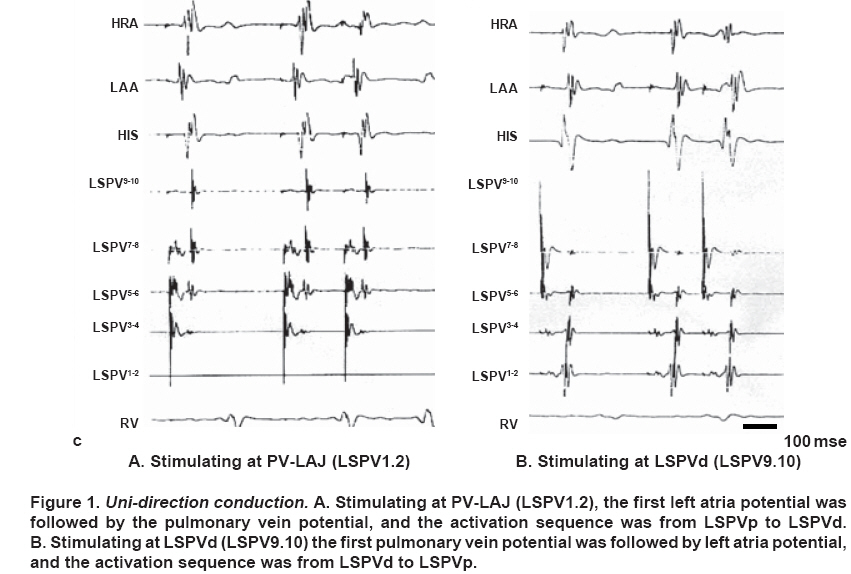
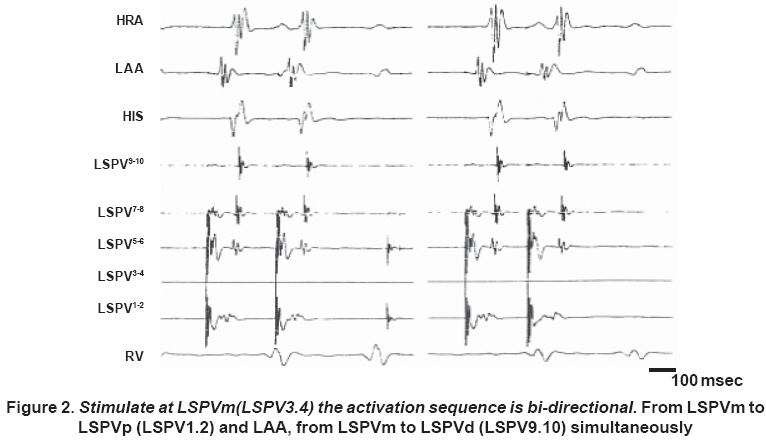
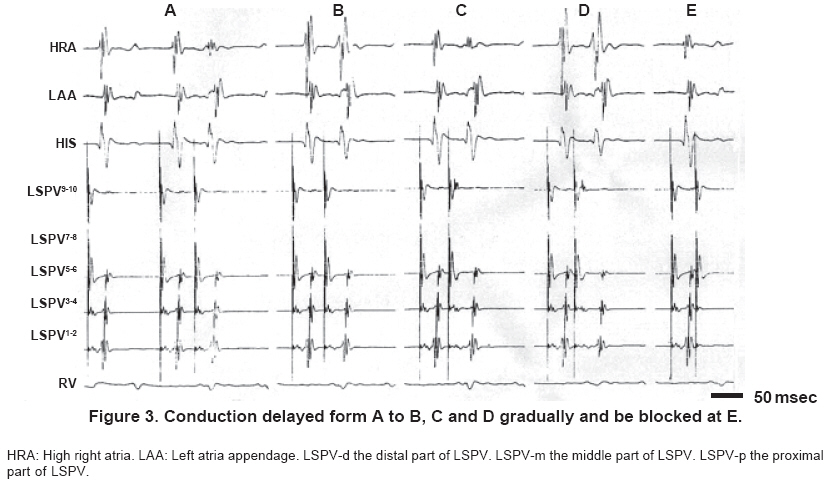
The conduction between left superior pulmonary vein and left atria with vagal response. Almost 25% paroxysmal AF will develop to chronic AF eventually. Ectopic beats initiating PAF originate from mainly (95%) left pulmonary vein, especially from left superior pulmonary vein (LSPV)14-17. Precisely locating the ablation targets and exactly finding the end point of ablation PV will be certainly useful in reaching higher ablation successful rate, reducing recurrence and complication of AF by pulmonary vein (PV) isolation. Investigating the foci in pulmonary veins, activation conducting characteristics of pulmonary veins will provide us more information of conduction traveling through left atrium to PV-LA and within LSPV. It has been shown that physiologically the muscular wall of the left atrium may extend up to a few centimeters around the pulmonary veins, more so in the superior than the inferior pulmonary veins. There is one single or dual-input electric conduction back and forth from LSPV, which might produce more than one breakthrough. Previous studies showed that ectopic beats originating from the PV propagated to the LA with characteristically long conduction time, often with conduction delay or block within the PV or at the PV-LA junction18-20. However, the detailed conduction patterns within the PV and across the PV-LA junction with vagal reponse remained unclear. In our study, with vagal response and by endocardiac mapping, we found that the potentials of LA and PV at LA, PV-LAJ, LSPVm and LSPVd were overlapped with sinus rhythm, were separated by pacing at each sites mentioned above, and were separated remarkably by stimulating at the distal part of LSPV. We also demonstrated that unidirectional (activation conduction sequence was from LA to PV-LAJ, and finally to LSPV by pacing at LA, from LSPV to PV-LAJ, and to LA by pacing at LSPVd) and bi-directional conduction (activation conduction sequence was from LSPVm to both PV-LAJ and LA as well as to LSPVd simultaneously by pacing at LSPVm), bi-directional decremented conduction as well as slowed retrograde conduction (from LSPV to LA) within LSPV and delayed conduction or conduction block from stimulation signal to local tissue potential before AF. These results remind us activation conduction sequence differs by pacing near LA or within LSPV from that sinus rhythm. The unidirectional, bi-directional and decremented or blocked conducting characteristics within LSPV as well as across PV-LAJ in both with or without vagal response condition remind us that the totally isolation PV form LA in AF ablation will be reached only by blocking activation conduction both in sinus rhythm and also in pacing at PV site. INDICATION Our study suggested that the pronounced ERP shortening at PV-LAJ and within LSPVS, significantly increased ERP heterogeneity within LSPV, abnormal activation conduction within LSPV and across PV-LAJ, and different response to cervical vagal trunk vagal stimulation played an important role in local reentry, which might be the underlying mechanism for initiation and maintenance of AF. Our results indicated that vagal denervation, eliminating focal fast firing and blocking activation conduction around PV are the ideal approaches to treat AF and effective way in preventing AF recurrence. LIMITATION The present study investigated the electrical conduction characteristics of LA, PV-LAJ and LSPV, ERP of HRA, LAA, PV-LAJ and LSPV, ERP heterogeneity within LSPV and the inducibility of AF by cervical vagal nerve trunk stimulating. We found that the ERP of HRA, LAA, PV-LAJ LSPVm be reduced significantly, ERP heterogeneity within LSPV and the inducibility of AF increased, and the activation conduction sequence at LA, PV-LAJ and within LSPV was different by pacing at LA from that at LSPV. Despite the promising early results, there were some limitations. Firstly, our data came from anesthetized dogs, thus the ERP of LA,PV-LAJ and LSPV, ERP of HRA, LAA, PV-LAJ and LSPV, and the inducibility of AF might be affected on. Secondly, our results could be used only to explain the possible mechanism of AF, which was no structure heart diseases. Finally, we did not pay our attention to sympathetic effect, which might be exist in cervical vagal nerve trunk stimulating. CONCLUSION The rapid focal firing within or near LSPV as well as abnormal conduction between LA and PV and within PV under abnormal parasympathetic tone was happy to produce AF. Thus, the higher successful rate of AF ablation, the lower recurrence rate of AF and less complication could be reached only by totally blocked conduction between LA and PV, which could be conformed by comparing the conduction in sinus rhythm with that in pacing at PV site, by eradicating the fast focal firing (triggers) within PV and by modifying autonomic nerve function, which might be the substrate for AF initiating and maintenance. Our research be supported by the grants from Chinese Nature and Science Fund and post-doctor fellowship from The First Teaching Hospital Foundation. Urmuqi City, Xinjiang, China. REFERENCE 1. Tsang TSM, Miyasaka Y, Barnes ME, Gersh BJ. Epidemiological profile
of atrial fibrillation: a contemporary perspective. Prog Cardiovasc
Dis. 2005; 48: 1-8. © Copyright 2008 - Revista Colombia Médica The following images related to this document are available:Photo images[rc08048f3.jpg] [rc08048f4b.jpg] [rc08048t1.jpg] [rc08048f4a.jpg] [rc08048f2.jpg] [rc08048f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}