 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Revista Colombia Médica, Vol. 40, No. 1, Enero-Marzo, 2009, pp. 43-50 Detection of genes mutations in the K-ras, H-ras and EGFR in samples of blood plasma and cervical smears for patients with cervical intraepithelial neoplasia III and cervical cancer Detección de mutaciones en los genes K-ras, H-ras y EGFR en muestras de plasma sanguíneo y cepillado cervical de pacientes con neoplasia intraepitelial cervical (NIC) III y cáncer de cuello uterino Dabeiba Adriana García, MSc1, Yazmín Rocío Arias, MSc2, Fabio Ancízar Aristizábal, PhD2 1Pontificia Universidad Javeriana, Centro de Investigaciones Odontológicas, Bogotá, Colombia.
e-mail: garciad@javeriana.edu.co yrariasm@unal.edu.co * Project supported by Universidad Nacional de Colombia, Bogotá, Colombia. Received for publication March 31, 2008 Code Number: rc09006 SUMMARY
Introduction: Cervical
cancer is the second most important cancer in women worldwide, and the
second cause of cancer death in women. It has been shown that the
process of cervical carcinogenesis presents as genetic and epigenetic
components as environmental issues. At present, many studies are
addressed in searching for molecular markers such as mutations in
oncogenes and/or tumor suppressor genes that are associated with the
progression of this disease, the most studied candidate genes in
cervical cancer in different populations have been H-ras, K-ras, EGFR
among others. Keywords: Mutation; Cervical cancer; High-grade lesion; Human papillomavirus; H-ras; K-ras; EGFR. RESUMEN
Introducción: El
cáncer cervical es el segundo cáncer más
importante en mujeres a nivel mundial y la segunda causa de muerte en
mujeres por cáncer. Se ha demostrado que el proceso de
carcinogénesis cervical presenta componentes tanto
genéticos, epigenéticos y medio ambientales. En la
actualidad, muchos estudios se encaminan en la búsqueda de
marcadores moleculares como mutaciones en oncogenes y/o genes tumor
supresor que se asocien con la progresión de esta entidad. Los
genes candidatos más estudiados en cáncer cervical en
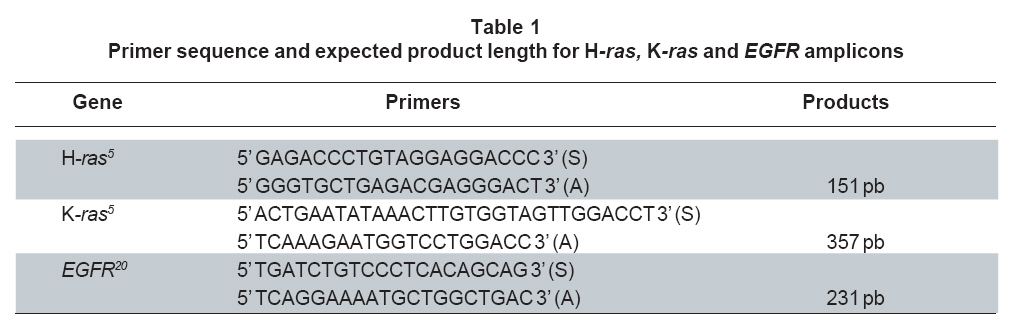
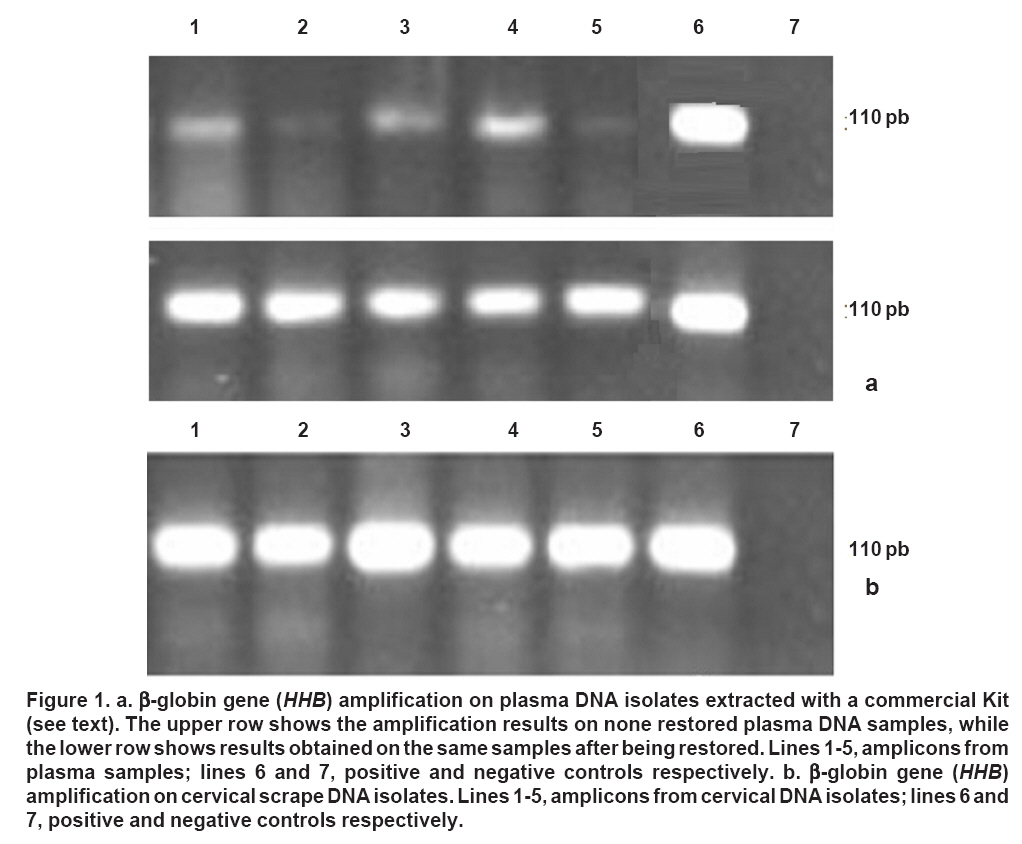
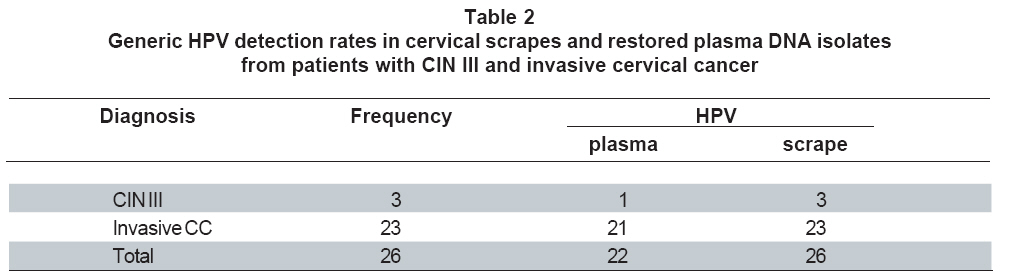
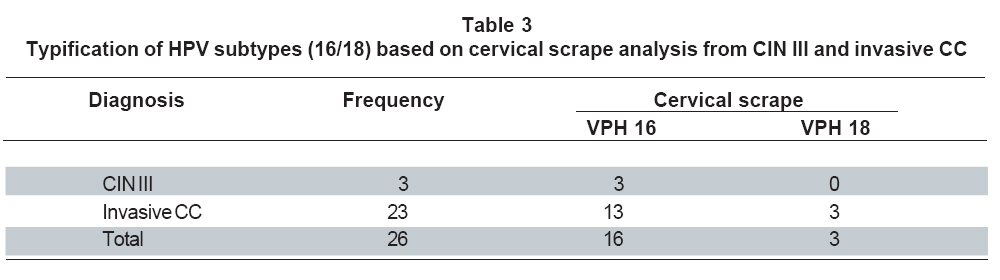
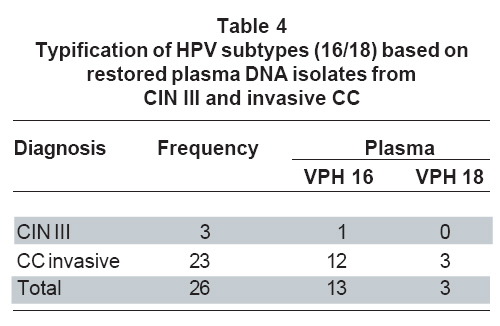
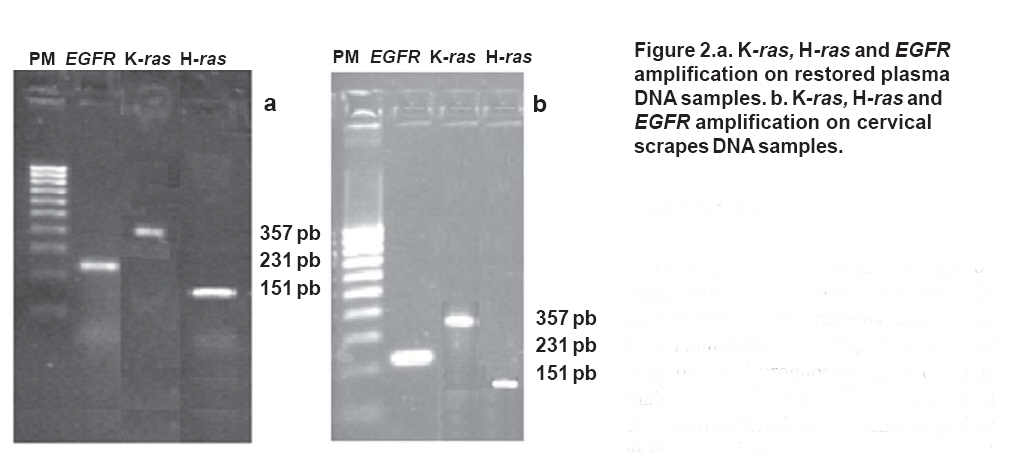
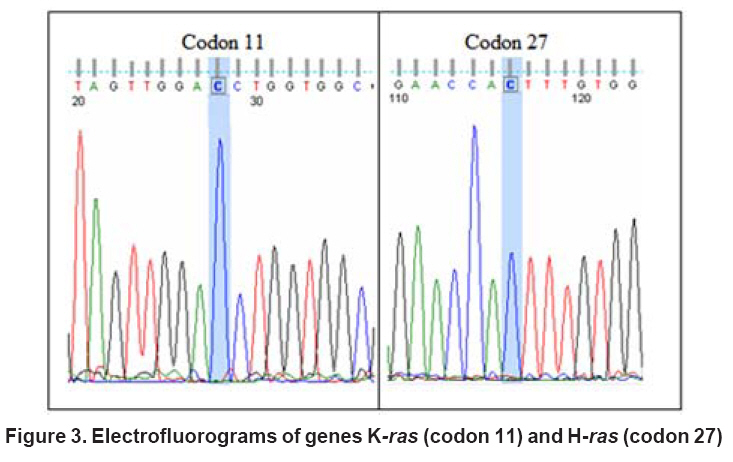
distintas poblaciones han sido H-ras, K-ras, EGFR entre otros. Palabras clave: Mutaciones; Cáncer cervical; Lesión intraepitelial de alto grado; Papilomavirus humano; H-ras; K-ras; EGFR. Cervical cancer is one of the world most important diseases. In Colombia, estimated incidence is 29.4 cases per every 100,000 inhabitants1. Cervical carcinogenesis begins with non invasive squamous lesions that progress to low and high grade intraepithelial squamous lesions; and eventually generate an invasive carcinoma2. However, predicting which of them finally progress and which will reverse is currently impossible as the entire cellular and molecular mechanisms involved in progression are unknown. Even more, in spite of recent advances uncovering several routes leading to cervical carcinogenesis, no molecular marker been closely enough associated with progression or clinical outcome has been identified to date. Multiple findings provide evidence about the increased presence of cellular and viral DNA in plasma from cervical cancer patients3. Patients with various cancers like colon, esophagus, breast, pancreas, head and neck and liver present increased levels of free circulating plasma DNA. In addition to this, many genetic (such as amplified oncogenes, punctual mutations involving Tumor Suppressor Gene, microsatellite instabilities, etc) or epygenetic features (such as TSG methylated promoters) resemble those detected directly in the corresponding tumors4. So, plasma DNA from cancer patients becomes a promising target for detecting molecular cancer associated alterations which could be used as early cancer markers or an ongoing relapse of the disease after the primary treatment. In cervical cancer, mutations in EGFR, H-ras and K-ras, are some of the most frequent genetic changes studied. H-ras (Harvey) and K-ras (Kirsten) are located on chromosomes 11 and 12 respectively. These oncogenes code a 21 kDa protein called p21 which exhibits GTPase activity and is implied in cell cycle regulation5. Constitutive activation of them is mainly caused by punctual mutations at codons 12, 13 and 61, leading to the inhibition of its GTPase activity. High levels of ras function have been demonstrated in lung, bladder, breast, colon and cervical cancer among others. Besides, such mutations can be found in normal looking tissue and pre neoplastic lesions from cervical cancer patients, suggesting an important role in carcinogenesis6. EGFR (ErbB1) codes for a 170 kDa membrane receptor involved in cell proliferation. It is located in chromosome 7 and belongs to the ErbB tyrosine kinase family of receptors. Other members are Her2/neu (ErbB 2), ErbB 3 and ErbB 4. Among the extracellular ligands of EGFR are the EGF and the TGFa7. Ligand binding induces self phosphorylation and dimerization of the receptor with some conformational changes associated which initiate transduction of a transforming, anti-apoptotic, proliferative signal. In addition, mutations at exons 18-24, known to alterate its tyrosine kinase activity, have been found in epithelial tumors such as those on breast and cervix7. Since mutations in K-ras and H-ras GTPase domains have been presented as promising progression associated molecular markers, and so potential tools for relapse/metastasis detection in solid tumors, we decided to search whether mutations found in cervical scrapes from CIN III and cervical cancer patients in genes these loci are accurately resembled by alterations in free circulating plasma DNA from themselves. Presence of HPV was also evaluated in both samples. MATERIALS AND METHODS Patients and sampling procedure. This is a descriptive, crossectional study involving patients conveniently chosen during a 6 months lapse at a third level hospital in Bogotá DC. A cervical scrape and a peripheral blood sample were obtained from 26 patients who had been diagnosed with either a high grade intraepithelial lesion (HSIL) or cervical cancer (CC), during confirmative colposcopy. All of the patients were fully informed and required to sign a written consent before being enrolled in the study. None of them had received any therapy at the time of sampling. When obtained, every sample obtained by cervical scrape was introduced into a tube with Timerosal 0.05% in PBS. The tubes were kept on ice until their arrival to lab for processing. Each blood sample was drained into an EDTA added Venoject® tubes by venopuncture. Upon arrival, each cell suspension was centrifuged at 3000 g for 10 minutes, then the supernatant was discarded and de pellet was suspended in 1 ml of 10 mM Tris-HCl buffer (pH 8.3) and boiled during 10 minutes. After a one minute 3,000 g centrifugation the supernatant was directly used as PCR template source. Blood samples were centrifuged 20 minutes at 3,000 g, the upper plasma face was separated and further centrifuged at 8000 g for 3 minutes to completely deplete cellular debris. DNA extraction was carried out with the QIAamp® DNA Mini Kit (QIAGEN; Germany) following manufactures instructions. DNA isolates were then subjected to a pre-PCR «restoration» treatment as previously described8. Briefly, each plasma DNA sample is incubated at 55°C with dNTPs 200 mM for 1 hour. The treatment is performed in the presence of Tris-HCl 10 mM, 50 mM KCl, 0.1% triton X-100, and MgCl2 3 mM. Then one unit of Taq DNA polymerase is added an incubated 20 minutes more at 72°C. DNA quality. Since DNA in plasma is subjected to multiple degradative conditions it is necessary to that DNA extracted is quality enough to support PCR. Quality of the DNA from cervical scrapes and plasma (restored and non restored) was evaluated by amplification of the b-globin gene (HHB) with primers PCO3 (ACACAACTGTGTTCACTAGC) and PCO4 (CAA CTTCATCCACCTTCACC) with Tris-HCl 10 mM, 50 mM KCl, 0.1% triton X-100, MgCl2 3 mM, 7.5 pmol each primer, 1U Taq DNA pol and 200 mM each dNTP. Reactions were performed in a MyCyclerTM termocycler (BioRad Laboratorios, USA) by running the following cycling program: 95°C - 3 minutes, and 95°C - 20 seconds, 58°C - 20 seconds and 72°C - 20 seconds for 40 repetitions. Products were analyzed by 2% agarose electrophoresis where expected product is 110 bp long. Lymphocyte DNA was used as positive control. HPV detection and typification. Generic detection of HPV was also performed by PCR with primers GP5+ (TTTGTTACTGTGGTAGATACTA) and GP6+ (GAAAAATAAACTGTAAATCATA). Reagent conditions were as follows: Tris-HCl 10mM, 50 mM KCl, 0.1% triton X-100, 3 mM MgCl2, 0.3 mM each primer, 1U Taq DNA pol and 200 uM each dNTP; with the following program: 95°C - 4 minutes; and 95°C - 1 minute, 47°C - 1 minute and 72°C - 1.5 minutes for 40 repetitions. Products were equally analyzed by electrophoresis as described above. DNA isolates from both cervical scrape and restored plasma DNA from HPV positive cases were further assayed for HPV16 and 18 by PCR targeted to the E6/E7 region. Primers used were as follows: HPV16, primers ATCATCAAG AACACGTAGAG and GATCAGTTGTCTCTGGTT GCAAAT; HPV18, primers GATTTCACAACATA GCTGGG and TGCCTTAGGTCCATGCATAC. In both cases the first is the sense primer while the second is the antisense primer. Reagent conditions were identical to those for generic HPV detection, while cycling conditions were: 94°C - 2 minutes; 94°C - 30 seconds, 60°C - 30 seconds y 72°C - 30 seconds. As before, products were analyzed by agarose electrophoresis. Final reaction volumes were 50 ml for generic detection and 25 ml for type specific detection. For all HPV detections plasmids pBR322 Zur Hausen donation containing either HPV16 or HPV18 complete genomes were used as positive controls. H-ras, K-ras and EGFR mutation analysis. PCR products were also generated to verify base identities at codon 12 of H-ras, codons 12 and 13 of K-ras, and exon 21 of EGFR from cervical scrapes and restored plasma DNAs. Primers used are showed in Table 1. Reagent conditions were as used in assays above, and a final volume of 25 ml was used. Cycling conditions were: an initial 94°C - 5 min denaturation step for all the amplicons; 94°C - 30 sec, 60°C - 30 sec and 72°C - 30 sec for H-ras and K-ras; while 94°C - 30 sec, 58°C - 30 sec and 72°C - 30 sec was used for EGFR. Products were purified with the Wizard® DNA Clean-Up System (Promega) according to manufacturer instructions, and sequenced in an ABI 3730 XL sequencer (Applied Biosystems, Foster City, CA) by McLabs in San Francisco CA. Ethical issues. This study was respected the ethic and legal aspects for in humans research stipulated in Resolution 008430 of 1993 (Colombian Ministry of Health), and the 2004 modified Helsinki declaration (1975). The patients enrolled in this study voluntarily accepted to participate after reading and understanding the consent form. This form was approved by the Ethics committees of the Javeriana and National Universities (Bogotá). Statistical analysis. A data base was constructed with patient’s information in an EXCEL file (Microsoft). A one variable descriptive analysis was performed with qualitative variables like the presence of HPV and the presence of mutations in the sequences. Frequency distribution was determined for each one, and association tests were applied (Pearson’s c2) to link cervical scrape and plasma DNA isolates. RESULTS HHB (b-globin) amplification confirmed that DNA isolates from cervical scrapes and plasma were quality enough to generate reliable and reproducible PCR amplifications. Besides, the pre-PCR restoration treatment demonstrated to improve template quality, allowing a more sensitive detection of this single copy gene (Figure 1). In gel measurement of the band relative optical density (ROD), shows a great increase for HHB amplification upon plasma DNA restoration. Initial average ROD was 427.2 while the same parameter raised to 1032.2 after the treatment. Measures showed 286.3 and 183.4 as standard deviation respectively. 100% of cervical scrapes and 84.6% of plasmas were positive for HPV, generic detection targets the L1 region of viral genome coding for the viral capsomer. The stretch amplified is a 142 bp long amplicon (Table 2). Detection of this amplicon in cervical scrapes and plasma showed great correlation as verified by a P value of 0.0374. Specific subtype detection in cervical scrapes revealed 61.5% and 11.5% of incidence for HPV16 and 18 respectively among HPV positive cases (Table 3). HPV16 was demonstrated in 50% of the plasmas while HPV18 was detected in 11.5% of them (Table 4). In two patients, who presented both cervical cancer and a CIN III lesion at colposcopy, subtype specific HPV detection was not possible. In general, though HPV16 detection in cervical scrapes was not fully matched to that in plasmas, results demonstrate concordance (61.4% and 50% respectively). No plasma sample showed a HPV subtype not found in the corresponding cervical scrape. On the other hand, HPV18 showed equal incidence in scrapes and plasmas (11.5%). K-ras, H-ras and EGFR were successfully amplified in both cervical scrapes and plasma DNA from all the cases (Figure 2). Isoform A of EGFR was the sequence found in all the patients. Exon 1 was shown not to be altered in any of the cases. Codon 12 of H-ras didn’t show mutations either; however, two patients showed a third base change at codon 27 (CAT changed to CAC) detected in both cervical scrape and matched plasma DNA. Since it is a silent mutation, it continues to code for Histidine. Besides, no mutations were seen in codons 12 and 13 of K-ras; however, all the patients showed a CCT sequence in codon 11 which codes for Proline, instead of GCT corresponding to Alanine as occurs in the type sequence. Even though both amino acids are non polar, they greatly differ in the contribution they do to higher order protein holding (Figure 3). DISCUSSION Both genomic and viral DNA can be effectively retrieved from plasma from CIN III and invasive CC patients, confirming plasma analysis as an important tool for diagnosis and prognosis3. However, this material could have suffered single and double strand breakage reducing its quality as PCR template. The restoration treatment applied to plasma DNA isolates allows single strand gaps to be filled by using the information of the complementary strand as template, so improving its quality for genetic markers detection. Since the pre-PCR restoration treatment used here does not includes the repetitive synthesis cycles proper of PCR it does not increases the number of copies of the target sequence. The treatment only restores available copies so that primers find them more efficiently8. Regarding HPV detection in cervical scrapes, it was 100% incident among the cases analyzed; this is compatible with the very high association commonly found and supports the causal relationship between HPV and cervical neoplasia9. HPV detection in plasma from CIN III and CC patients allowed to classify 84.6% of the cases as positive, which demonstrate a better detection rate than that presented previously studies by Wei et al.4 and Widschwendter et al.10 where HPV was confirmed in 64.7% and 45% of plasmas from patients with positive detection in tumor respectively. Our better detection rate can be explained by better template integrity after the restoration treatment applied. HPV16 was detected in 61.54% of cases (cervical scrape detection), resembling previous studies by Rabelo-Santos et al.11 in Brazil (57.1%); on the other hand, HPV18 was found in 11.5% of our cases, similarly to detection rates presented by Bosch et al.12 and Muñoz13, whose detection rates were 14% and 13.6% respectively. Specific detection in plasma allowed HPV16 detection in 50% of cases, while HPV18 was found in 11.5% of them. Previous data from assays targeted to plasma indicate a very low rate even for generic detection. Specific detection and typification have been consequently very limited. As an example, results presented by Dong3 were 3.5% for subtype 16 and 2.1% for HPV18. EGFR gene was found unaltered at exon 21 in all our cases. Similar results are reported by Pühringer-Oppermann et al.14 for esophageal cancer. Sequence mutations in codon 12 of H-ras were not found in our cases either resembling reports by Mammas et al.5 in cervical cancer, and Vachtenheim et al.15 for lung squamous carcinomas; however, two of the cases showed a mutation at codon 27 (CAT to CAC) both in scrapes and matched plasmas. Similar results are presented by Lev et al.16 in melanoma cells. K-ras, was not found mutated at codons 12 and 13 either, as reported by Pochylski and Kwasniewska17 in cervical squamous cell carcinomas. However, codon 11 was found to be changed from GCT to CCT (Ala to Pro) in all the cases. This mutation was previously found by Gu et al.18 and Hongyo et al.19 in patients with lung carcinomas and gastric adenomas respectively. In general, a good correlation was observed between sequences of H-ras, K-ras and EGFR found in cervical scrapes and plasmas. As also demonstrated by Dong, et al.3, sequence alterations at specific loci found in plasma DNA isolates from cancer patients closely resemble those present in tumors. We conclude that analyzing free circulating DNA in plasma from cancer patients is a reliable approximation to tumor genetic features, allowing the analysis of numerous genetic markers when obtaining tumor mass samples is not an option. ACKNOWLEDGEMENTS The authors thank the Departamento de Farmacia and the Instituto de Biotecnología of the Universidad Nacional de Colombia (Bogotá, Colombia). The DIB (División de Investigaciones Bogotá) of the Universidad Nacional provided all the funds to afford this project (Code: 2010000). We thank the great help received from doctor Antonio Huertas Salgado (Instituto Nacional de Cancerología ESE, Bogotá) at sequence analysis, and doctor Fabián Carrillo for their assistance in translation into English of this article. REFERENCES
© Copyright 2009 - Revista Colombia Médica The following images related to this document are available:Photo images[rc09006f3.jpg] [rc09006t3.jpg] [rc09006f2.jpg] [rc09006t2.jpg] [rc09006t4.jpg] [rc09006f1.jpg] [rc09006t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}