 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Revista Colombia Médica, Vol. 41, No. 3, 2010, pp. 235-239 Evidence in Colombia of 625G>A polymorphism in the short chain acyl-CoA dehydrogenase gene, a variation which could cause glutaric aciduria in our populations Evidencia del polimorfismo 625G>A en el gen de la acil-CoA deshidrogenasa de cadena corta en Colombia, una variación que podría causar aciduria glutárica en algunas poblaciones del país José Henry Osorio, PhD* * Department of Basic Sciences for Health, Research Laboratory in Clinical Biochemistry and Molecular Pathology, Universidad de Caldas, Manizales, Colombia. e-mail: jose.osorio_o@ucaldas.edu.co Received for publication June 12, 2009 Code Number: rc10034 SUMMARY Introduction: Short-chain acyl-CoA dehydrogenase
(SCAD) is a homotetrameric mitochondrial flavoenzyme that catalyzes the initial
reaction in short-chain fatty acid β-oxidation. The SCAD gene is located
on chromosome 12q22 and is approximately 13 kb long with 10 exons and 1236
nucleotides of coding
sequence. Hereditary SCAD deficiency has been reported and only a few cases
of this disorder have been described. Keywords: Short-chain acyl-CoA dehydrogenase; 625G>A polymorphism; Ethylmalonic aciduria; β-oxidation. RESUMEN Introducción: La acil-CoA deshidrogenasa
de cadena corta (SCAD) es una flavoenzima
homotetramérica mitocondrial que cataliza la reacción inicial de
la â-oxidación de los ácidos grasos de cadena corta. El gen
SCAD se ubica en el cromosoma 12q22, con una longitud de 13 kb, con 10 exones
y 1236 nucleótidos de secuencia
codificadora. Se ha informado la deficiencia hereditaria de
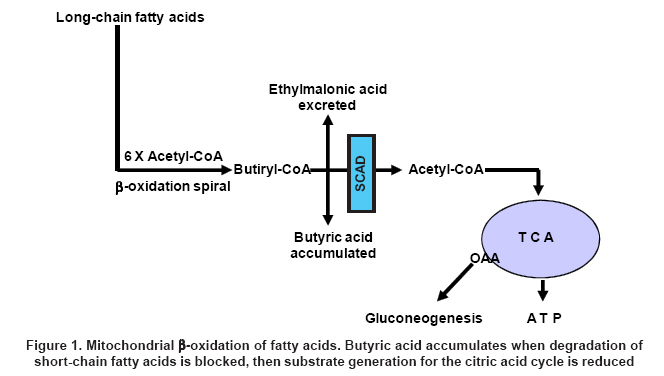
SCAD y se han descrito pocos casos de la deficiencia. Palabras claves: Acil-CoA deshidrogenasa de cadena corta; Polimorfismo 625G>A; Aciduria etilmalónica;β -oxidación. All the currently identified mitochondrial fatty acid (FA) β-oxidation defects are autosomal recessive. The clinical manifestations result from the inability of FA-oxidising tissues to keep up with increased energy demands; therefore, target organs of FA oxidation defects include skeletal and cardiac muscles in addition to the liver1. Hypoketotic hypoglycaemia is present in nearly all the defects, and usually occurs following an intercurrent illness, but may occasionally be seen after a short fast. In general, FA oxidation disorders should always be included in the differential diagnosis of unexplained hypoglycaemia, metabolic acidosis, Reye’s like syndrome, myopathy, recurrent myoglobinuria, and cardiomyopathy2. Laboratory findings reinforce the clinical diagnosis, levels of intermediary metabolites in urine (glucose, ketone bodies, lactate, pyruvate), and blood (non-sterified FA)3; urinary organic acid profile4; body fluids and tissue acylcarnitine analysis5; enzyme measurement and pathway intermediates in cultured cells and leukocytes6,7, and DNA analysis8 are used to confirm the diagnosis of any alteration. Short-chain acyl-CoA dehydrogenase deficiency is a poorly characterized mitochondrial fatty acid β-oxidation disorder with a very variable clinical picture and at least 35 inactivating mutations and some polymorphic variants have been reported in the SCAD gene9. Hereditary SCAD deficiency was first reported in 198410 and only few cases of this disorder have been described for either classic SCAD deficiency or variant SCAD10-13. A clinically reliable diagnosis requires either a muscle biopsy for the measurement of the enzymatic SCAD activity or molecular genetic analysis of the SCAD gene, both only available in research laboratories. This situation is further complicated by the presence of the mainly two variants (625 G>A and 511C>T) in the SCAD gene that are frequent in the European population, and have been reported to confer disease susceptibility14. In the 625G>A variation the polymorphic site is a transition from G to A at position 625 (A625) of the coding region of the cDNA, changing a glycine to serine at amino acid position (G185S) of the precursor protein. The variant 625G>A has been shown to be associated with ethymalonic aciduria and other biochemical findings15. Because urinary ethymalonic acid (EMA) elevation most likely reflects a cellular accumulation of butyryl-CoA16, which is secondary to reduced SCAD catalytic activity, these patients are correctly considered as possibly having SCAD deficiency. Despite the fact that most patients with EMA aciduria have not had their SCAD activity determined, an association between elevated EMA and SCAD has been documented by the presence of either or both of two SCAD gene susceptibility variations in 69% of patients with EMA aciduria17. The 625G>A variant shows homozygous prevalence of 60%, as SCAD protein presents reduced stability compared to the control SCAD protein18. As SCAD is a key enzyme in the oxidation of fatty acids, which serve as substrates for the gluconeogenesis (Figure 1), reduced SCAD activity because of the 625G>A variant for fasting hypoglycaemia, and ethymalonic aciduria as shown in the SCAD deficiency. The present study was conducted to determine the possible presence of the 625G>A variation in the short-chain acyl-CoA dehydrogenase gene in Caldas, Colombia, as the 625G>A and 511C>T variations are present in 14% of some populations studied, sometimes causing its deficiency. MATERIALS AND METHODS The present study is descriptive. Blood samples used in this study were from 300 adult, healthy volunteers between 18 and 49 years of age (120 men and 180 women), all born in Caldas, Colombia, apparently none suffering from any inherited inborn error of metabolism. According to the number of persons visiting our laboratory, samples were collected between January 2006 and January 2009, which means that samples were obtained by convenience, and all participants signed written consent. Blood samples were extracted in tubes containing EDTA. DNA extraction was performed according to Gustafson et al.19, with some modifications. The polymorphism was identified by comparing the polymerase chain reaction (PCR) and amplified cDNA from a previously studied person carrying the polymorphism with the apparently healthy volunteers. A single-stranded conformation polymorphism (SSCP) assay, based on the following primers was used: Sense primer: 5’-GCAGCTCTGAGAAAACCAC. Antisense primer: 5’-ATGTCC AGGGTTTGCTGT. PCR Conditions: 3 min at 94°C, 40 sec at 94°C, 30 sec at 55°C, and 2 min at 72°C for 35 cycles with 500 ng of purified genomic DNA as template and 75 ng of each primer. When DNA fragments were subjected to electrophoresis in 8% acrilamide/bisacrilamide (19:1), 7.5 M urea gel, at room temperature for 3 hours, the single-base change at position 625 was clearly detected after silver stain. The results were confirmed by direct bidirectional cycle sequencing using DNA. According to Article 11 on its literal a from Resolution N° 8430 promulgated by the Ministry of Health for Scientific, technical and administrative guidelines for health research, the present study is considered without risk. The study was approved by the corresponding ethics committee. RESULTS After analyzing DNA samples from the 300 participants, the polymorphism was identified in four apparently healthy adult volunteers -all in heterozygosis. The first case was a 21-year-old male who was born from non-consanguineous parents, another two individuals were identified as carriers of the polymorphism; they are the parents of a family who presented two cases of sudden infant death after two consecutive pregnancies and they are cousins. After a third pregnancy, a baby was born and after 2 years she is still alive without problems; she did not present the 625G>A polymorphism. A fourth person was identified as carrying the polymorphism, an apparently normal 22-year-old woman. The four persons are from families without antecedents of any disease that could be related to some fatty acid oxidation disorder; the acylcarnitine analysis was normal for all of them. DISCUSSION Colombia is divided into 35 regions with an approximate total population of 45-million inhabitants, presenting racial mixture. Data obtained from the 2005 census shows that Caldas (a Colombian region) has a population of 968,740 inhabitants distributed within 29 municipalities20. For us, it is very important to detect the presence of this polymorphism to demonstrate the presence of fatty-acid-oxidation inherited diseases among us, and it is a valuable contribution for the future understanding of geographical distribution and ethnic origin elucidation of SCAD deficiency, as no previous reports have been published showing the presence of this polymorphism in these countries, while being mainly reported in Europe and the United States21. The first person presenting this variant in our study has a very interesting genetic charge for these kinds of works, as his father is from Tumaco, a region of black population and his mother is from the north of Antioquia, a place characterized by the presence of a strong Spaniard white genotype. The other 3 persons are from the centre of the country. There are reports of ethnic differences observed with respect to the 625G>A variant, while the allele frequency was similar between Caucasians and Hispanics (25 and 30%, respectively), African-Americans and Asians carried the 625G>A variant less frequently (9 and 13%, respectively)22. Corydon et al.14, found the 625A variant allele in homozygous form in 60% of 135 patients with elevated EMA excretion, analysed because a suspicion of a metabolic disorder, compared with 7% occurrence in the general population. That is why, since about 10-14% of the general population is homozygous 625G>A or 511C>T or compound heterozygous for both, it is necessary to have some other indication that they are disease-associated. It is generally accepted that some biochemical analysis can be performed to confirm if the person carrying the polymorphism is suffering the disease. Because these patients are phenotypically diverse, the analysis of blood acylcarnitines is a good tool for diagnosing SCAD deficiency. The acylcarnitine profile in these patients is characterized by high blood concentrations of butyrylcarnitine (C4-acylcarnitine). The acylcarnitine profile for our patients was normal; hence, they are carrying the polymorphism without suffering the disease. CONCLUSION Short-chain acyl-CoA dehydrogenase (SCAD) deficiency is a clinically heterogeneous disorder. The clinical phenotype varies from fatal metabolic decompensation in early life to subtle adult onset, and some patients remain asymptomatic. Two mutations (511C>T; 625G>A) have been described in exons 5 and 6 of the SCAD gene, respectively. These variants are not true disease-causing mutations but can confer disease susceptibility because they alter the structural and catalytic properties of the SCAD protein. Although the prevalent finding for SCAD deficiency is neurological abnormalities, such as hypotonia and seizures accompanying general developmental delay, the population of patients with ethylmalonic aciduria with a high frequency of the 625A variant allele in the homozygous form also showed diverse phenotypes, typically neuromuscular symptoms, and hypoglycaemia. The acylcarnitine analysis is an important tool in diagnosing the disease, given that a high concentration of C4-acylcarnitine is consistent with a biochemical diagnosis of SCAD deficiency. This kind of study is important for us because it shows the presence of mutations or polymorphisms, which can cause some metabolic alterations related to enzymatic dysfunction of some biochemical ways, not reported or treated among us. We need to continue studying our populations to know the real frequency of this polymorphism because the principal studies have been performed mainly in Caucasoid populations. Conflict of interest. None of the author had conflicts of interest related to this study. REFERENCES
Copyright 2010 - Colombia Médica The following images related to this document are available:Photo images[rc10034f1.jpg] |
| |||||||||
{kind=link}