 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Revista Colombia Médica, Vol. 41, No. 3, 2010, pp. 248-255 Latissimus dorsi transposition for sequelae of obstetric palsy Transferencia del músculo dorsal ancho en secuelas obstétricas del plexo braquial Enrique Vergara-Amador* *Associate
Professor, Hand surgeon and Pediatric orthopedist, Department of Orthopedics,
Universidad Nacional de Colombia, Bogotá, DC, Colombia. Ancient
resident, Institut Francais de la Main, Paris, France. Received
for publication July 23, 2009 Code Number: rc10036 SUMMARY Background: In obstetric palsy, limitation
in the external abduction and rotation of the shoulder is the most frequent
sequelae. Glenohumeral deformity is the result of muscular imbalance between
the external and internal rotators. Releasing the contracted muscles and
transferring the latissimus dorsi are the most common surgeries in this case. Keywords: Obstetric palsy; Transfers muscular shoulder; Latissimus dorsi; Subscapular. RESUMEN Introducción: Las limitaciones
en la abducción y la rotación externa del hombro son
las secuelas más frecuentes en la parálisis obstétrica.
Se encuentra deformidad de la articulación glenohumeral como resultado
del desequilibrio que existe entre los músculos rotadores externos
e internos. Dentro de las cirugías más usadas para corregir
las deformidades del hombro están las liberaciones musculares y la
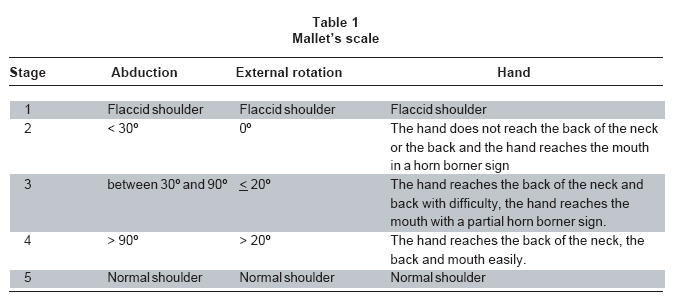
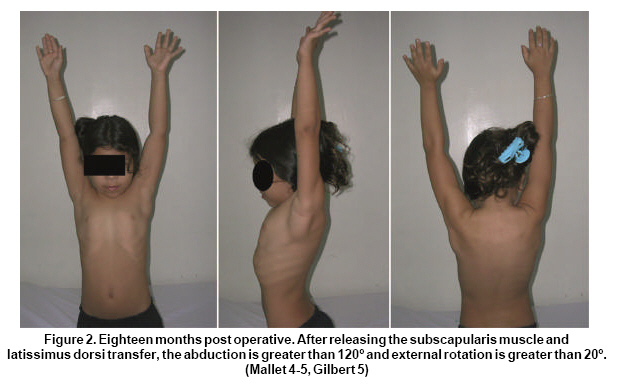
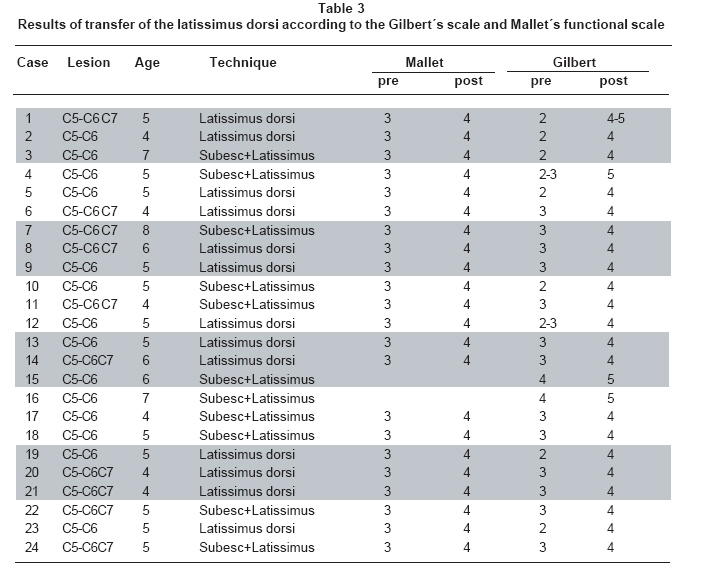
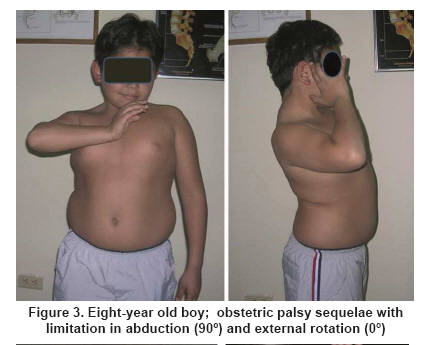
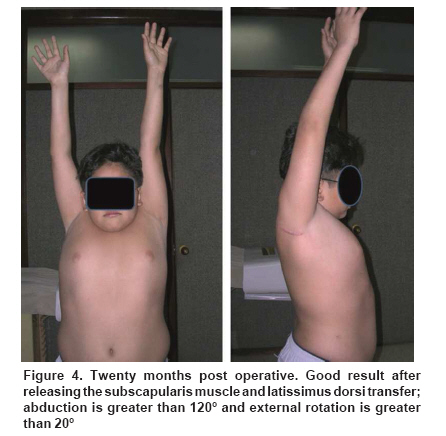
transposición del músculo dorsal ancho. Palabras clave: Parálisis braquial obstétrica; Transferencia muscular; Dorsal ancho. In obstetric brachial plexus injuries, most patients recover spontaneously without surgery. The nerve roots frequently compromised by typical Erb’s palsy are C5 and C6, where an absence of abduction and external rotation of the shoulder, flexion of the elbow and supination of the forearm are found. When the C7 nerve root is affected, a deficit in the extension of the hand is gene-rally found. Many of the total injuries at the beginning recovery of the lower roots and remain a definitely lesion of the upper plexus. Non-recovery of the bicep flexion against gravity before 3 to 4 months of age or of the deltoids has been an indication that plexus exploration is necessary1-3. This indication has been extended to 6-9 months by different authors who have argued that nerve reconstruction procedures are useful up to the first year of age4,5. Good functioning is expected for children who recover anti-gravity biceps strength before the age of 6 months. In the case of children whose biceps recover before the age of 6 weeks, it is possible to achieve total recovery6. Limitation in abduction and external rotation caused by weakness in the deltoid muscles and the external rotators of the shoulder are the most frequent secondary deformities. Contracture in adduction and internal rotation could appear early due to the lack of opposition to the muscle forces generated by the subscapularis, pectoralis major, teres major and latissimus dorsi. This difficulty in performing external rotation will produce posterior subluxation of the humeral head in the long term, causing it and the glenoid to become deformed. This will in turn bring about limitation in mobility and pain in the long run7,8. Early reconstruction, along with the release of the contracted tendons and tendinous transfers, will improve passive and active mobility and retard deformities in the glenohumeral joint9,10. Releasing the compromised structures includes elevation of the subscapularis muscle. This can be done on the tendinous part of the muscle but it is not generally recommended because of the risk of residual instability. It can also be done through the posterior approach by releasing the muscle on the anterior surface of the scapula5,11-13 and releasing the teres major and the pectoral major. The transfer of the latissimus dorsi muscle is done to improve external rotation and the abduction at the same time. In 1934, L’Episcopo14 described the transfer of the latissimus dorsi and teres major to the lateral humerus to improve external rotation. Hoffer10 described the transfer of the latissimus dorsi by taking it posterior and superior in a rotator cuff to allow greater external rotation and abduction with a functional deltoid. When a good latissimus dorsi does not exist, transfers of the trapezium or of the scapula elevator may be considered12,15,16. The purpose of this article is to describe the results in a case series with in the transfer of the latissimus dorsi with the elevation of the subscapularis muscle off the anterior surface of the scapula in children with obstetric palsy sequelae. PATIENTS AND METHODS There were 24 patients with obstetrical brachial plexus sequelae who had operations performed by the same surgeon (EVA), between 1997 and 2006, to transfer the latissimus dorsi, which, in the cases of 11 children, was associated with elevation of the subscapularis muscle. There was a minimum follow up of 2 years. Movement of the shoulder was limited in all cases, especially in abduction and external rotation, which made it difficult to carry out some ordinary daily activities like getting dressed, combing the hair, and lifting objects to the face or mouth. Six patients had an operation on the plexus before they were one year of age and 18 had not received any surgical treatment. A transfer of the latissimus dorsi to the infraspinous and supraspinous tendon was done on all of the patients. Releasing the subscapularis muscle was done at the same time on 11 patients except for one who had been operated on at 3 years of age to elevate just the subscapularis muscle. The criteria for releasing the subscapularis muscle was external passive rotation of less than 20º. All the patients had normal morphology in the X-rays. When there was a poor image on the X- ray, a CT scan was taken. The average age at the time of surgery was 5.1 years of age (ranging from 4 to 8 years of age). The minimum age for surgery was 4; patients were evaluated before and after the operation based on Mallet’s scale and the scale for the shoulder described by Gilbert (Tables 1, 2). Surgical technique. The patient is placed in lateral decubitus position under general anesthesia. An approximately 5 cm axial incision is made on the lateral border of the scapula when a release of the scapula is being planned. When only a transfer is planned, the incision is made in the posterior axillary fold; it is dissected subcutaneously and the interval of the latissimus dorsi with the teres major is located on the external border of the scapula. If the latissimus dorsi is of poor quality, the teres major will be added to the transfer. Because the teres major is smaller with a lesser excursion than the latissimus dorsi, the teres major is released from the latissimus dorsi and sutured to the same muscle more proximally, thus, integrating the two muscles to the transfer. The dissection towards the humerus is performed with extreme care. It is not necessary to see the radial nerve. This last part can be done with blunt dissection up to the insertion of the latissimus dorsi into the humerus. The muscle is released and lifted while being careful not to exert tension on the vascular-nervous pedicle. With the latissimus dorsi lifted, we reach the lateral border of the scapula and the subscapularis muscle is lifted subperiosteally, starting on the lateral and inferior border and continuing towards the medial and superior border with a periosteal elevator. It is important to release the medial corners because, if not, the subscapularis muscle cannot slide well. After that, the shoulder should rotate 30º externally. If it is not possible to achieve good external rotation at the moment, consider releasing the anterior capsule of the shoulder and of the coracohumeral ligament (CHL) without cutting the subscapularis muscle tendon. The latissimus dorsi tendon goes under the deltoids and it is sutured to the infraspinous on the lateral superior part. A fast anchor was not used in any case. If abduction improvement is rendered, the latissimus dorsi is sutured to the supraspinatus tendon with the arm at maximum external rotation and an abduction of 90 to 120º. The wound is closed in two layers with absorbable suture. The arm is immobilized in a position of minimal abduction of 90º degrees and with external rotation in the Statue of Liberty position for 5 weeks. When rehabilitation is started, immobilization is continued at night for three more weeks. RESULTS Overall, we obtained good results; there were no hematomas, neurological or vascular injuries, nor infection. Of 22 patients scored on Mallet’s functional scale, all were at 3 points before surgery and improved to 4 points. Based on Gilbert’s scale, 13 patients were at 3 before surgery and improved to 4. Seven patients were at 2 and improved to 4. One patient was at an intermediate classification between 2 and 3 and improved to 4. One patient went from 3 to 5, and two patients went from 4 to 5. In other words, all of the patients improved in the two scales (Figures 1, 2; Table 3). The parents of the patients were satisfied with the functional results (Figures 3, 4). DISCUSSION External rotation and abduction of the shoulder with progressive contracture in internal rotation and adduction are the most important sequelae for the shoulder in obstetric paralysis. The muscular imbalance between the weak external rotator (infraspinous) and the strong internal rotators (teres major, latissimus dorsi, pectoral major, and subscapularis) is the main factor for deformity in internal rotation and adduction of the shoulder. The subscapularis is the largest of the four rotator cuff muscles. Einarsson et al.17, demonstrated the abnormal mechanical properties of the subscapularis muscle in individuals with obstetric brachial plexus palsy when they analyzed the passive mechanical characteristics of biopsies from the subscapularis muscle obtained through open surgery. Secondary deformities such as the elongation of the coracoids, flattening or deformation of the humeral head with subluxation or posterior dislocation and flattening or retroversion of the glenoid may be found7,8. Hoeksma et al.7, reported a 56% prevalence of contractures greater than 10% and a 33% prevalence of osseous deformity in a series of 53 patients treated without surgery. Waters et al.9, say that the natural history of obstetrical brachial paralysis with muscular weakness is glenohumeral deformity because of muscular imbalance. Using computed tomography (CT) or magnetic resonance imaging (MRI) to evaluate the gleno scapular angle (retroversion) on a series of 42 patients, the healthy side showed -5.5 on the average and the affected side, -25.7 with 62% of the patients presenting posterior subluxation and increased deformity with age. Bahm et al.18, noted that although the muscular imbalance might explain most of the progressing deformities of the glenohumeral joint, it was necessary to be aware of the rare cases of connatal traumatic subluxations of the humeral head, which can cause a rapid contracture requiring immediate surgery. The anterior release of the subscapularis muscle has been used extensively but has the drawback of causing anterior instability in the shoulder. Carlioz and Brahimi11 improved the external rotation of the shoulder by releasing the subscapularis muscle off the anterior surface of the scapula through a posterior approach. This is indicated when the patient still has a congruent glenohumeral joint13,19. If the external rotator muscles are weak, transfer of the latissimus dorsi should be done immediately, as well. This transfer will improve active abduction of the shoulder given that it stabilizes the rotator cuff and makes the deltoids more effective13,16. Pagnotta et al.13, evaluated 203 patients who had undergone operations on their shoulders followed by long-term follow up. This showed that individuals benefiting most from the surgery were children who had C5 and C6 paralysis and those who scored 2 and 3 on the Gilbert scale. According to the authors, six years after the surgery some patients presented loss of abduction but kept external rotation. It is possible that the cause of this is functional exclusion on the part of the child and lack of rehabilitation. All of the children in this report improved in abduction and external rotation. Our follow up is relatively short and loss of abduction has not been observed. All of the children improved on the functional scales. The 22 who were evaluated based on Mallet’s scale improved one degree. Eight patients improved two degrees and 16 patients improved one degree based on Gilbert’s scale. Two children could not be correctly classified on Mallet’s scale prior to surgery. They had more than 90º of abduction but a deficit of external rotation of 0º and -20º. We noticed patients who were not easily classified. There were children who were found between Mallet’s classifications of 3 and 4. There were patients whose degrees of abduction were greater than 90º, but whose external rotations were less than 20º or negative, making it impossible to classify them. Gilbert’s classification gives us a closer approach to reality than Mallet’s, although there are some patients whose recovery of abduction and external rotation are dissociated. For example, case 16 presented abduction greater than 120º, but an external rotation of 0º. Currently, patients who are classified into stages 3, 4, and 5 on Gilbert‘s scale are being evaluated and sub-classified. The breakdown we used for this sub-classification is the following:
The patients have to be carefully selected. Good passive mobility in abduction, a minimum external rotation of 20º and no joint deformities are required for the transfer of the latissimus dorsi. When an external rotation of 0º or negative is found, releasing the subscapularis muscle is considered. At the same time, we evaluated whether or not it was necessary to release the major pectoral muscle. Sometimes, though not in this series, it is necessary to release the anterior capsule of the glenohumeral joint through an anterior approach or the coracohumeral ligament. When there is posterior subluxation or glenohumeral joint deformity in older children, other methods are recommended such as rotational osteotomy of the proximal humerus20. No benefits in any form have been received or will be received from any commercial party related directly or indirectly to the subject of this article. REFERENCES
Copyright 2010 - Colombia Médica The following images related to this document are available:Photo images[rc10036t3.jpg] [rc10036f3.jpg] [rc10036t1.jpg] [rc10036f2.jpg] [rc10036t2.jpg] [rc10036f4.jpg] [rc10036f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}