 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Colombia Médica, Vol. 41, No. 4, October-December, 2010, pp. 367-372 Dysplasia epiphysealis capitis femoris. Meyer dysplasia Displasia epifisaria de la cabeza femoral. Displasia de Meyer Enrique Vergara-Amador, MD1, Marcela Piña, MD2 1Professor, Orthopaedic department, Universidad Nacional de Colombia, Bogotá, DC, Colombia.
e-mail: enriquevergaraa@yahoo.com Received for publication February 28, 2010 Code Number: rc10053 SUMMARY Introduction: Epiphyseal dysplasia of the femoral head (EDFH) is defined as an
alteration in the development of the child’s hip, characterized
by delayed ossification of the proximal femoral epiphysis. Keywords: Meyer dysplasia; Legg-Perthes disease; Hip. RESUMEN Introducción: La displasia epifisaria de la cabeza femoral (DECF) es definida como
una alteración del desarrollo de la cadera en el niño,
caracterizada por un retraso en la osificación con irregularidad
en el núcleo de osificación de la epífisis
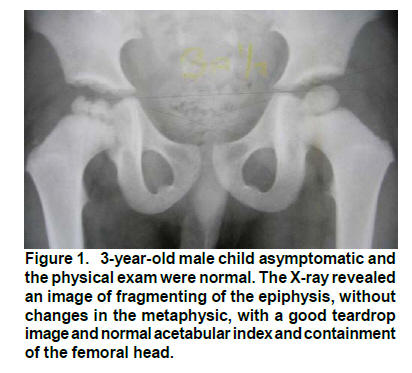
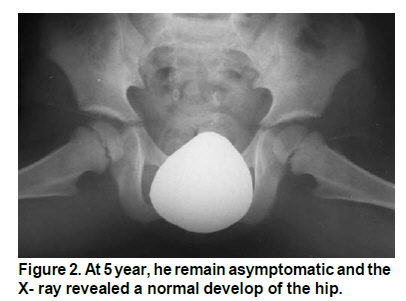
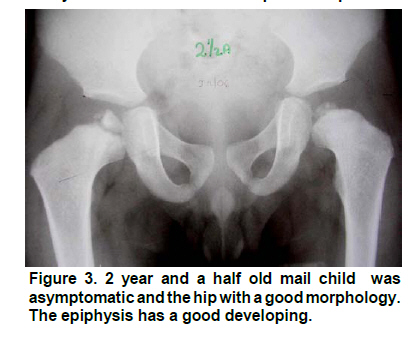
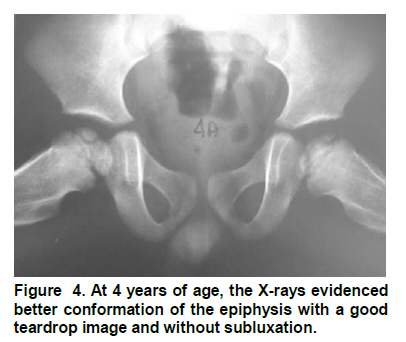
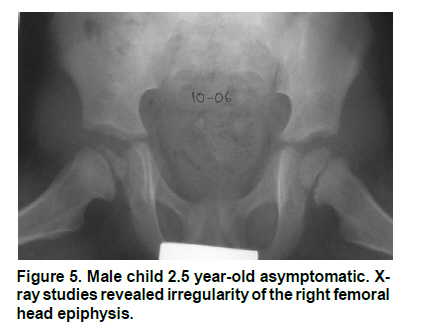
proximal del fémur. Palabras clave: Diplasia de Meyer; Enfermedad de Legg Perthes; Cadera. Epiphyseal dysplasia of the femoral head (EDFH) is defined as an alteration in the development of the child’s hip, characterized by delayed ossification with irregularity in the ossification center of the proximal femoral epiphysis1,2. Normal ossification takes place on the average at 4 months of age, although it may be considered normal up to the 11th month; however, in Meyer’s dysplasia, ossification appears around 15 to 18 months of age as multiple ossification centers, giving the femoral head a modulated epiphysis aspect1. The disease was first described by Pedersen in 19503 and then by Meyer in 19642, to whom the name of the condition is attributed. Meyer estimated that close to 10% of the patients diagnosed with Perthes disease corresponded to a dysplasia and not to a necrosis, unlike Rowe who estimated a 4.4%4 incidence. The etiology of EDFH, unlike Perthes disease, is not established. Several hypotheses have been postulated, among which the one formulated by Meyer2 stands out announcing the theory of ischemic vascular damage as the cause of delayed and irregular ossification, the theory by Batory5 speaks of a congenital vascular defect, and -lastly- the congenital proximal femoral hypoplasia5; however, none of these have been supported by scientific evidence. Epidemiologically, it has been determined that this condition involves boys in greater proportion than girls in a ratio of 5:1 and in those under 5 years of age1,4. The bilateral commitment reported by different studies ranges from 42 to 60%1,2,4,6, much greater than that reported for Perthes disease. Most of these patients have no symptomatology; however, when there is also hip pain, decreased range of motion, and limp stride. Symptoms appear closet o the second year of life lasting from 1 to 3 weeks1,5,6,7. The diagnosis is generally accidental via X-ray examination8. MATERIALS AND METHODS We present six cases of children with epiphyseal dysplasia of the femoral head, seen by the principal author (EVA) during a period of six years with minimum follow up at 15 months. The anatomical pieces were documented with digital photographs and thereafter stored. Data were analyzed through descriptive statistics in Excel 2007. Ethical considerations. The ethical implications of the current study were minimal, given that they corresponded to a study without risk, which used information from the clinical histories, without intervention on the patients. The information obtained was kept strictly confidential and was used exclusively by the researchers. This study was approved by the Ethics Committee at the University mentioned. RESULTS All the cases were diagnosed as a casual finding. None of the children had symptoms or clinical signs in the hip. Only one of the children had a history of hip pain for five days, two months prior, which was diagnosed at the time as transient synovitis. One case was bilateral and the rest were unilateral, for a total of seven hips. Four patients were males and two were females. None of the patients received treatment. At the end of the follow up they continued asymptomatic. Three exemplary cases are shown: Case 1. A 3-year-old male child, referred to consultation with diagnosis of Perthes disease. This child had not reported pain, was asymptomatic, and the physical exam of the hips was totally normal. There was no antecedent of importance, nor the taking of any medication by the patient or by the mother during gestation. The X-ray study of the right hip revealed an image of fragmenting of the epiphysis, without changes in the metaphysis. A good teardrop image and normal acetabular index, along with containment of the femoral head is noted in Figure 1. The initial diagnosis was epiphyseal dysplasia of the femoral head and only observation was recommended. Evolution was positive, remaining asymptomatic with progressive ossification of the femoral head at 5 years of age (Figure 2). Case 2. Male child without antecedents, referred to consultation at 18 months of age with diagnosis of Perthes disease, asymptomatic and with normal physical exam. The patient had an X-ray taken at 3.5 months of age and it was considered normal. At a year and a half, the child continued asymptomatic and X-ray studies showed small and irregular nuclei. At 4 years of age, the patient was asymptomatic and the X-rays evidenced better conformation of the femoral head, good teardrop image without subluxation, lacking ossification in some sites of the epiphysis (Figures 3, 4). Case 3. Male child 2.5 years of age sent for consultation with diagnosis of Perthes disease. The patient was found asymptomatic and with a normal physical exam. X-ray studies revealed irregularity of the right femoral head epiphysis. Because of the clinical and radiological state it was considered compatible with epiphyseal dysplasia of the femoral head or Meyer’s Dysplasia. Results at 6 years of age were promising (Figures 5, 6). DISCUSSION In this situation, we note delay and irregularity in ossification of the proximal femoral epiphyseal nucleus, which does not appear before two years of age4. The nucleus takes on an appearance with a multiple granular pattern, with an ossification center made up of multiple independent nuclei that grow and finally coalesce to form only one9; on average, around 5 years of age5. The first finding is the decrease in the distance of the upper edge of the metaphysis to the Hilgenreiner line, which is generally 9.3 mm ± 1.5 at 7 months of age. In his series, Khermosh found values from 4-8 mm in 2-year-old children; from 4.5 to 9 mm in children at the third year of life, and from 5-10 mm in children at the third year of life, suggesting that the cartilaginous epiphysis is initially smaller than the normal epiphysis5. Scintigraphy study reports no alterations, while magnetic resonance reveals multiple ossification centers of the femoral head with normal signal intensity and decrease in epiphysis size6. All the frames show normal irrigation of the epiphyseal trabecular bone, the physis articular cartilage, and of the cortical bone5. Among the differential diagnoses, the main one is for Perthes disease, which is differentiated by several parameters: age of earlier onset for EDFH (in children below 4 years of age), bilateralism (50% vs. 10%)8, and a calmer presentation in Meyer’s dysplasia; radiological signals in Perthes disease permit staging the disease, while in dysplasia there is no fragmentation, condensation, subchondral fracture, or epiphysis collapse; hence, there are no consequences as with Perthes disease1,4,6,7. Other differential diagnoses point to infectious processes that in some children may be accompanied by elevated erythrocyte sedimentation rate (ESR) and leukocytosis; however, scintigraphy rules out the condition. In cases of bilateral presentation, we must rule out another type of multiple dysplasia and hypotyroidism1,7. Evolution in Meyer’s dysplasia is towards improvement in radiologic changes1,2,6. None of the patients revealed incongruence of the hip or early degenerative changes, indicating excellent prognosis. Many authors consider it a variant of normal ossification of the femoral head. Because of its evolution and good prognosis, treatment has not been determined necessary for these patients. X-ray control is recommended to assess the resolution of the pathology. All patients in this series remained asymptomatic, without clinical signs, agreeing with the literature in that most are asymptomatic. Very few patients had antecedence of synovitis4,6. In conclusion, it is a rare condition, with a benign clinical course, which must be kept in mind in children below five years of age with atypical onset of fragmenting of the ossification center of the femoral head2,4-6. No treatment is required, but the evolution of the development of the femoral head should be closely watched. Conflict of interest. None of the authors has conflicts of interest related to this study. REFERENCES
The following images related to this document are available:Photo images[rc10053f4.jpg] [rc10053f3.jpg] [rc10053f1.jpg] [rc10053f6.jpg] [rc10053f2.jpg] [rc10053f5.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}