 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Colombia Médica, Vol. 42, No. 1, January-March, 2011, pp. 39-47 Children affected with HIV/AIDS: Information of HIV/AIDS in five Colombian cities* Niñez afectada con VIH/SIDA: Información sobre VIH/SIDA en cinco ciudades colombianas Ana María Trejos, Psychol1, Rafael de Jesús Tuesca, PhD2, Mario Mosquera, PhD3
1Coordinator of University
Welfare, Universidad del Norte Hospital, Direction of University
Welfare. Universidad del Norte, Barranquilla. e-mail: atrejos@uninorte.edu.co * Agreement 0168-04-06 Instituto Colombiano de Bienestar Familiar-Save the Children-UNICEF, Department of Research and Projects (DIP), Universidad del Norte, Barranquilla. Received for publication November 23, 2009 Code Number: rc11006s SUMMARY Objectives: To describe information about HIV/AIDS in a youth population under 18
years of age affected with HIV/AIDS and caregivers in five Colombian
cities: Cali, Buenaventura, Barranquilla, Santa Marta, and Cartagena. Keywords: HIV seropositive; Acquired immunodeficiency syndrome; Information about HIV/AIDS; Patient education as subject; Childhood population. RESUMEN Objetivos: Describir información sobre VIH/SIDA en población
infantil afectada y menor de 18 años y cuidadores en cinco
ciudades colombianas: Cali, Buenaventura, Barranquilla, Santa Marta y
Cartagena. Palabras clave: Seropositividad para VIH; Síndrome de Inmunodeficiencia Adquirida; Información sobre VIH/SIDA; Educación del paciente como asunto; Población infantil. The acquired immunodeficiency syndrome (AIDS) has claimed the lives of over 25-million people throughout the world, making it one of the most destructive epidemics in the annals of history1. AIDS has become a worldwide emergency issue and one of the most serious challenges for human life and dignity2,3. Urgently diminishing and containing the propagation of this world epidemic requires universal access to joint prevention, treatment, and support. If the world moves this way to simultaneously and dynamically broaden HIV prevention, treatment, and attention, we could reach authentic integral criteria to approach AIDS, which curtails the epidemic and inverts its course4,5. Although the most recent international epidemiological data indicate that the world percentage of people living with HIV was established in 2000 and the estimated rate of mortality through AIDS diminished due to pharmacological advancements and access to anti-retroviral therapy, these tendencies are still unequal in different world regions. It is estimated that in 2007, there were 33-million [30.3-36.1-million] people living with HIV. Worldwide, the number of children under 15 years of age who live with HIV increased to 1.6-million (1.4–2.1 million) in 2001 to 2.0-million (1.9-million–2.3-million), while youth between 15 and 24 years of age represent 45% of the estimated new HIV infections6. The development of the HIV/AIDS Programmed Management Model7 defines programs and actions for integral attention, access, and anti-retroviral medication supply to reduce the complications of the disease, as well as offers protection and permanent educational support to improve awareness, knowledge, and autonomous management of the disease for people living with HIV/AIDS. Knowledge and information on HIV/AIDS are considered priority factors to reduce vulnerability in high-risk populations, like children, adolescents, and their families, as well as for the population already affected by the disease. In this sense, the purpose of this article is to describe information on HIV/AIDS in children and adolescents under 18 years of age with HIV/AIDS and their caregivers from public and private healthcare institutions in five Colombian cities: Cali, Buenaventura, Barranquilla, Santa Marta, and Cartagena. Aside from describing the information about what the HIV/AIDS disease is, along with its transmission and treatment mechanisms in the affected population, this research identified difficulties related with the process of disclosing the diagnosis of seropositivity for HIV/AIDS to Colombian minors by their caregivers and by the team offering them health services. METHODS A quantitative and qualitative descriptive study was undertaken, targeting children and adolescents under 18 years of age who knew they were affected by HIV/AIDS and whose caregivers consented their participation in the study, and caregivers of children and adolescents who were not aware of their being affected by HIV/AIDS, from public and private healthcare institutions in five Colombian cities: Cali, Buenaventura, Barranquilla, Santa Marta, and Cartagena. According to international definitions on the concept of childhood affected by HIV/AIDS, participating minors must comply with the following affectation categories as criteria of population inclusion, non-excluding amongst themselves:
A non-probabilistic sampling by quotas was done, whose size per city was determined by the criteria of experts in the participating cities and given the under registration and the disparity of the figures in the childhood and adolescent population affected by HIV/AIDS in our nation, a quota of up to one-hundred (100) surveys was determined, along with three (3) focal groups per city. According to population inclusion criteria and to conditions relevant to these types of studies mainly related to the political will of the institutions lending health services to youth populations affected by HIV/AIDS and, with the participation consent of the subjects in the study, 286 personal surveys were conducted; 11 of which were done on children and adolescents affected with HIV/AIDS who were aware of their HIV seropositive diagnosis and whose caregivers consented to their participation in the study, and 275 surveys to caregivers of children and adolescents affected with HIV/AIDS who were not aware of their HIV seropositive diagnosis. In the same manner, 15 focal groups were carried out with three different populations:
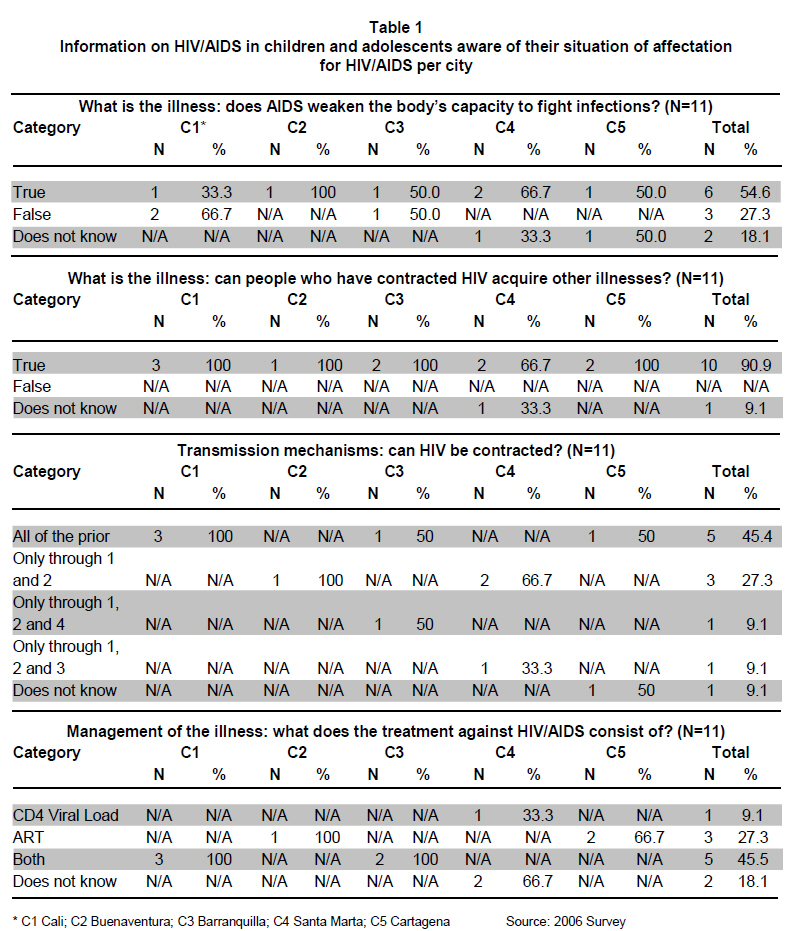
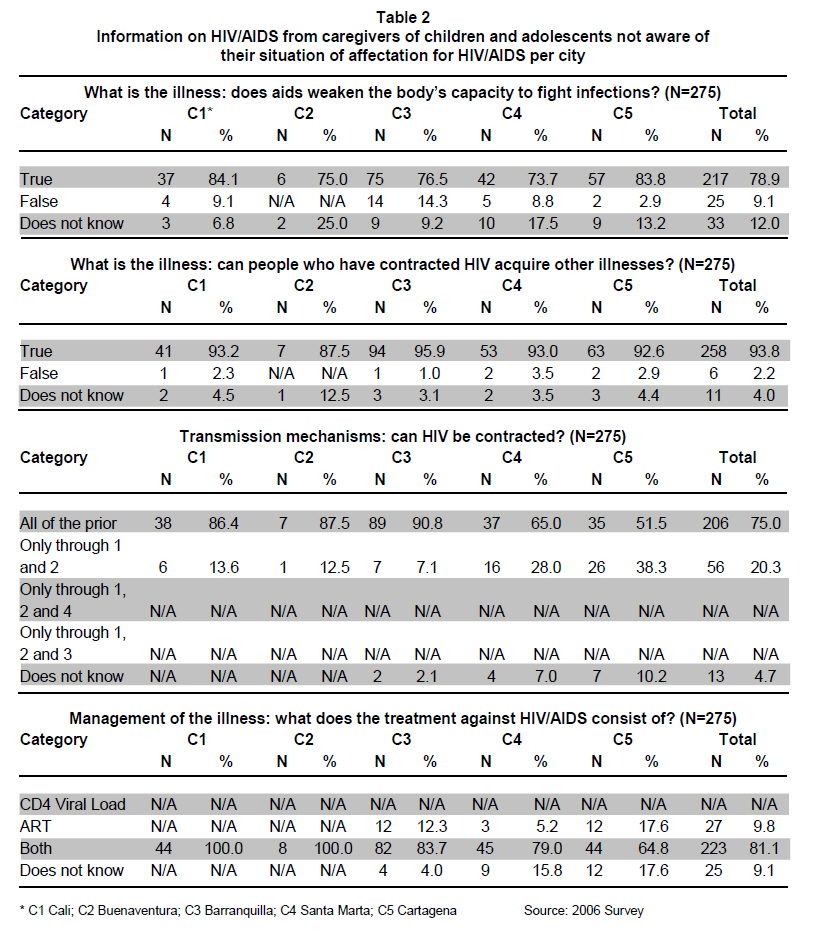
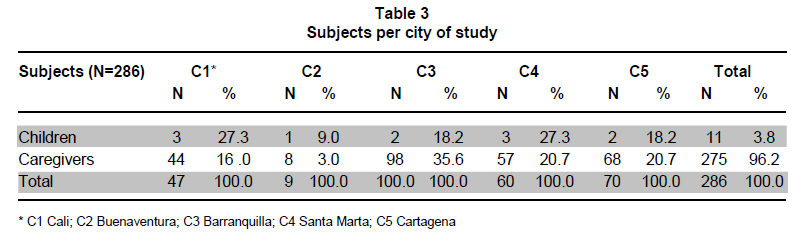
The source of primary information was through a personal survey of the subjects in the study. The protocol, the informed consent form for caregivers of affected minors, and the agreement to participate form for the child to participate in the study were made available to the directives of the public and private healthcare institutions selected for institutional backing and to guarantee access to the population subject of the study. The survey was structured to address sociodemographic and socioeconomic variables, and information on HIV/AIDS in children and adolescents and their caregivers. Prior to the elaboration of the instrument, interviews were done with the interdisciplinary teams at the healthcare institutions participating in the study to determine the informative contents on HIV/AIDS received by the affected childhood population and their families. After establishing the common contents of the interventions in the five cities under study, an instrument was elaborated regarding what the HIV/AIDS disease is, and its transmission mechanisms and clinical management. For adjusting the survey, a pilot test was run on a group of subjects who attended a foundation. The subjects participating in this phase did not reside in the cities of the Caribbean region selected for this study; this process permitted adjusting the scales and time of application of the instrument. A descriptive analysis was conducted of the data and the SPSS version 15 software in Spanish was used to process the information. Herein, we will present the information relating the dependent variable per participant subject and per city of study. Ethics. Seeking to guarantee the ethical aspects of the research8,9, the research protocol, the informed consent form, the agreement form for the child to participate in the study, and the instruments were submitted to evaluation by the ethics committees of the financing institutions and the institution executing the study; nevertheless, it must be cleared that the concepts of the financing institutions prevailed over the Research Ethics Committee in the area of healthcare at Universidad del Norte as the institution executing the study. By employing the ethical norms of the institutions financing the study, we kept in mind the legal capacity to grant consent thus, we obtained the informed consent form from caregivers of children and adolescents under 18 years of age affected by HIV/AIDS; preserving the right to privacy and intimacy, the confidentiality of the information gathered during the research process, and maintaining the anonymity of the information obtained at the moment of making public any information relevant to healthcare derived from the research, mainly reserving the names or identities of the subjects concerned; the agreement to participate form was only requested from children who were aware of their situation of affectation for HIV/AIDS. The process of obtaining the informed consent for the current study gathered three basic characteristics: sufficient information, understanding, and voluntariness. The information received by the study participants included the objectives and the methodology of the study; possible benefits and risks, as well as potential advantages, inconveniences, or damages of their participation in the study and how to compensate for these or repair them. They were also informed of their participation in the study being voluntary, of the possibility of abandoning without furnishing explanations and without affecting the quality of the healthcare assistance lent by the institution. Participants were informed of the restrictions to accessing the data by third parties, procedures to safeguard confidentiality, and how the results would be published. In this sense, it was remarked that risks would not be monetarily compensated but by doing everything possible to minimize them and that what would be compensated would not be the risks but the inconveniences and the time lost. Because of the low earnings of the participants, transportation costs were covered for those subjects who attended the personal survey and the focal groups at times not coinciding with their regular medical appointments; for the city of Santa Marta, in addition to transportation coverage, the foundation offered food incentives for those who participated in the research process. Lastly, researchers assigned to data collection manifested their identity, possible conflicts of interest, address, telephone number, and other contact information, and their willingness to respond to any matter that could arise during the course of the research. RESULTS Most 90.9% (N=10/11) of the children who knew of their situation of affectation for HIV/AIDS hold that upon acquiring the HIV virus, they can contract other illnesses; nevertheless, half 45.4% (N=5/11) are not aware that AIDS weakens the body’s capacity to fight infections (Table 1). The following opinions obtained from the focal groups illustrate the aforementioned: «…Well, I think HIV is a virus that enters the body, that it is difficult to come out, but if one takes the medication, taking it at the right time, and doesn’t stop taking it every day one will have much quality of life, and that now the individual who dies of HIV is because that individual wants to die, because now there anti-retroviral medications that one can take to be able to live more …». (Interview of a 13-year-old Seropositive Adolescent, Barranquilla, 2006) «…I think it is a very bad illness because I don’t know how it saddens people so much when they have that illness, but little if the person reacts, there is improvement little by little and if the medicine is taken at the right time the virus will be dormant, and it’s as if you didn’t have it…» (Interview of a 14-year-old Seropositive Adolescent, Barranquilla, 2006) In relation to mechanisms of HIV/AIDS transmission, 45.4% (N=5/11) children aware of their situation of affectation for HIV/AIDS recognize that the illness is transmitted through four mechanisms: sexual relationships without protection, blood transfusions, use of infected syringes, and from mother to child. 27.3% (N=3/11) of the children identify two mechanisms: sexual relationships without protection and blood transfusions; another smaller group 9.1% (N=1/11) also considers these two mentioned mechanisms, as well as the use of infected syringes; while another minor group 9.1% (N=1/11) considers the same two mechanisms, as well as the vertical transmission. Only one child reported not knowing the transmission mechanisms for HIV/AIDS. According to the aforementioned it may be noted that children (N=11) who were aware of their situation of affectation for HIV/AIDS mainly identify sexual relations without protection and blood transfusions as the principal transmission mechanisms for HIV/AIDS (Table 1). With respect to the information the children have on HIV/AIDS treatment, 45.5% (N=5/11) hold that anti-retroviral medication and viral load /CD4 T-lymphocyte count tests are required; 27.3% (N=3/11) of the children consider that treatment consists only of administering anti-retroviral medication, and 9.1% (N=1/11) feel that only viral load/CD4 T-lymphocyte count tests are needed; 2 children (18.1%) reported not having information with respect to HIV/AIDS treatment (Table 1). Most caregivers 96.2% (N=275) of children who were aware of their situation of affectation for HIV/AIDS had adequate information with respect to the nature of the illness, its transmission mechanisms, and treatment (Table 2). The results indicate that 78.9% (N=217) of the caregivers know that AIDS weakens the body’s capacity to fight infections, as opposed to 21.1% (N=58) who were not aware of this level of affectation of the illness. 93.8% (N=258) of the caregivers stated that individuals who had contracted the virus can acquire other illnesses. Related to the virus transmission mechanisms awareness by the caregivers, an important percentage, 75% (N=206), recognizes four forms of HIV transmission, opposed to 20.3% (N=56) who recognize only the mechanisms: sexual relations without protection and blood transfusions. Some 4.7% (N=13) of the caregivers do not know the HIV/AIDS transmission mechanisms (Table 2). 81.1% (N=223) of the caregivers stated that HIV treatment consisted of performing viral load / CD4 T-lymphocyte count tests and prescribing anti-retroviral therapy (ART). The following testimonial reveals this: «…At the Casa Gami Foundation, they had some workshops for 4 Saturdays with Doctor Lina, the Psychologist, the Nutritionist, and they advise you on how to take the medications, the schedules, all that. At least for me, those workshops were very useful …» (Focal Group of Legal Guardians in Cali, 2006). For the study group (Table 3) without awareness of their situation of affectation for HIV/AIDS, the current study identified the reasons why caregivers and healthcare professionals delay disclosing the diagnosis to the HIV/AIDS seropositive children. The caregivers manifested not opting to reveal the serologic status for HIV, seeking to protect the children against psychological damage or emotional stress that could be caused by knowing of the illness and for fear that once these children knew of their condition, they would inadvertently reveal such to other people, which would probably expose them to stigma, rejection, and/or discrimination. Professional lending healthcare services to the affected population reported not feeling trained on the issue of the proper procedure and age to deliver this information. The following testimonials illustrate the difficulties inherent to the process of disclosing the diagnosis of HIV/AIDS in children: «…the children know they are ill, I manage for them an illness quite different to what they have and, thus, I tell them they have to take the medication for the illness they have, they may know they are sick and that they have X illness, but they don’t really know what they have …» (Healthcare Providing Institution Psychologist, Focal Group of Workers in Cartagena, 2006). «…the child I am treating still does not know, although he asks many questions. But due to fear I have not told him anything, I don’t know how he will react. I told the physician and she suggested I speak to him little by little; I have AIDS and the boy asks me: «what do you have?», and I tell him playfully: «dear, it is something like AIDS». He also asks about the constant medical appointments he has to attend …» (Focal Group of Legal Guardians in Cartagena, 2006). »…I need help because it is difficult for me to tell her. Because the girl asks me daily: «Why do I have to take so much medicine?», and I answer her that if she doesn’t, she won’t get well. At 12 years of age, she has to be told the truth …» (Focal Group of Legal Guardians in Cartagena, 2006). DISCUSSION The results previously exposed indicate the difficulties experienced by healthcare professionals, parents and/or caregivers of HIV/AIDS seropositive children and adolescents with respect to the process of revealing the diagnosis. In the international context, the Guidelines of the American Pediatric Academy on disclosure of the HIV illness have received special attention. These guidelines hold that all adolescents must know their diagnosis and that disclosure must be considered for school-age children, bearing in mind their age, level of cognitive development, psychosocial maturity, complexity of the family dynamics, and the clinical context10. With development, it is considered adequate that elderly children and adolescents be aware of their diagnosis, given that with education and emotional support they can eventually have more control over the process of their illness; this being more imperative for adolescents to keep from, unknowingly, exposing others during sexual activity11. Two main factors emerged in the current study associated to barriers for disclosure of the diagnosis to children and adolescents who are seropositive for HIV/AIDS: the preoccupation of the parents or caregivers on the possible impact or emotional damage the disclosure could cause to the child. In other words, fears from the parents or the caregivers about the possible negative psychological consequences of the disclosure like: angst, depression, anxiety, and isolation. These data are consistent with the studies12-19. Also, there is fear that the involuntary disclosure by the child to others may lead to possible situations of stigma, discrimination, or ostracism of the child and family. In other words, parents or caregivers consider that the child is not capable of keeping the diagnosis secret. These data are consistent with the findings reported12,13,16,17,19-21. Pediatric patients with HIV and AIDS now live longer with improved quality of life, which makes disclosure an essential process, which is why the guidelines by the American Pediatric Academy on disclosing the HIV illness indicate that all adolescents should know of their serologic status and that disclosure should be considered for school-age children10. The results reveal that children and adolescents who are aware of their HIV/AIDS seropositive diagnosis need to enhance the information with respect to the HIV chronic disease. The children and young adolescents in the study revealed having inconsistent or incongruent information with respect to the principal action of the HIV virus. Half the children recognized as false that AIDS weakens the body’s capacity to fight infections, although most of them stated that by being infected by the HIV virus, they could acquire other illnesses. Equally, when asked about the treatment for the illness, half the children do not know that the anti-retroviral therapy is accompanied by tests to evaluate the viral load and the CD4 T- lymphocytes. As for the information the children have about HIV/AIDS transmission mechanisms, half of these only partially identify them. Also, parents and/or caregivers of children affected by HIV/AIDS recognize and have more precise information with respect to the illness, maintaining some percentages of parents and/or caregivers who are still unaware of some basic aspects of the illness. These results suggest the importance of enhancing training processes within healthcare institutions lending services to families affected by HIV/AIDS, as well as the importance of designing and implementing a clinical model for disclosure of the diagnosis, developmentally adequate to overcome the barriers or fears of parents and/or caregivers and healthcare professionals. Conflict of interest. None of the authors has conflicts of interest related to this study. ACKNOWLEDGMENTS The funding agencies have no involvement in the collection, data interpretation, or the decision to submit the manuscript for publication, so there is no conflict of interest with the project. An especially for the good disposition of the people who made this study possible: the children and adolescents affected by HIV/AIDS, legal guardians/caregivers from the five city regions: Cali, Buenaventura, Barranquilla, Santa Marta, and Cartagena. We also thank all the institutions serving individuals affected with HIV/AIDS and who accepted to collaborate with the development of the objectives of the study. Without their participation, field activities and research would not have been possible. REFERENCES
Copyright 2011 - Colombia Médica The following images related to this document are available:Photo images[rc11006t2.jpg] [rc11006t3.jpg] [rc11006t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}