 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 5, No. 1, August, 2001 pp. 31-39 Ranking Reproductive Health Problems to Define Service Priorities Theo Vos1 1Department of Human Services, Melbourne,
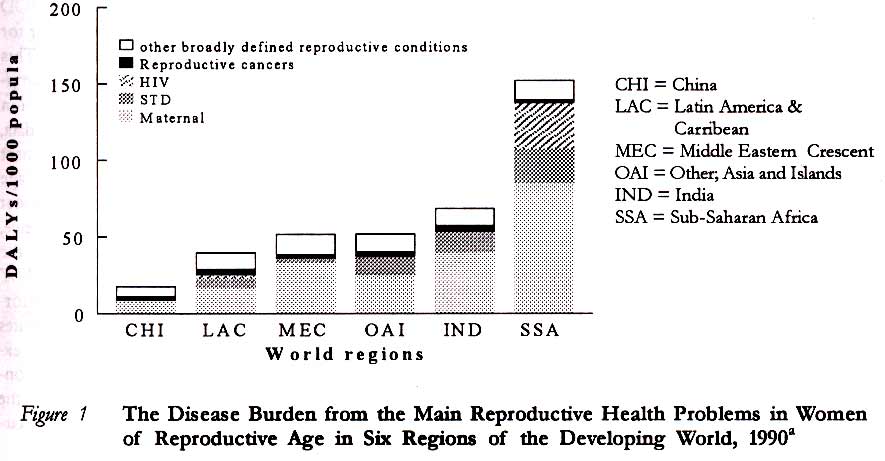
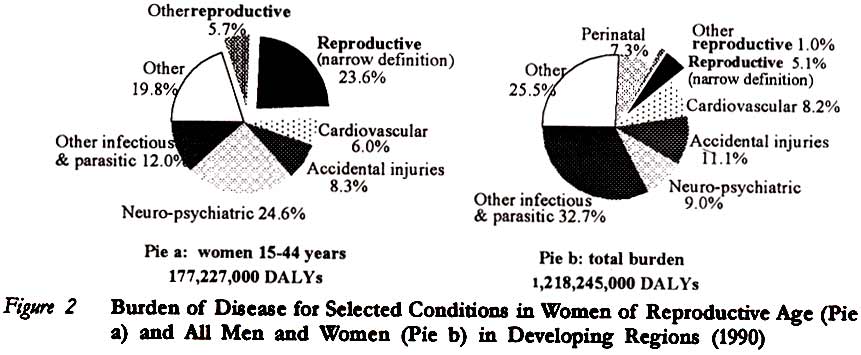
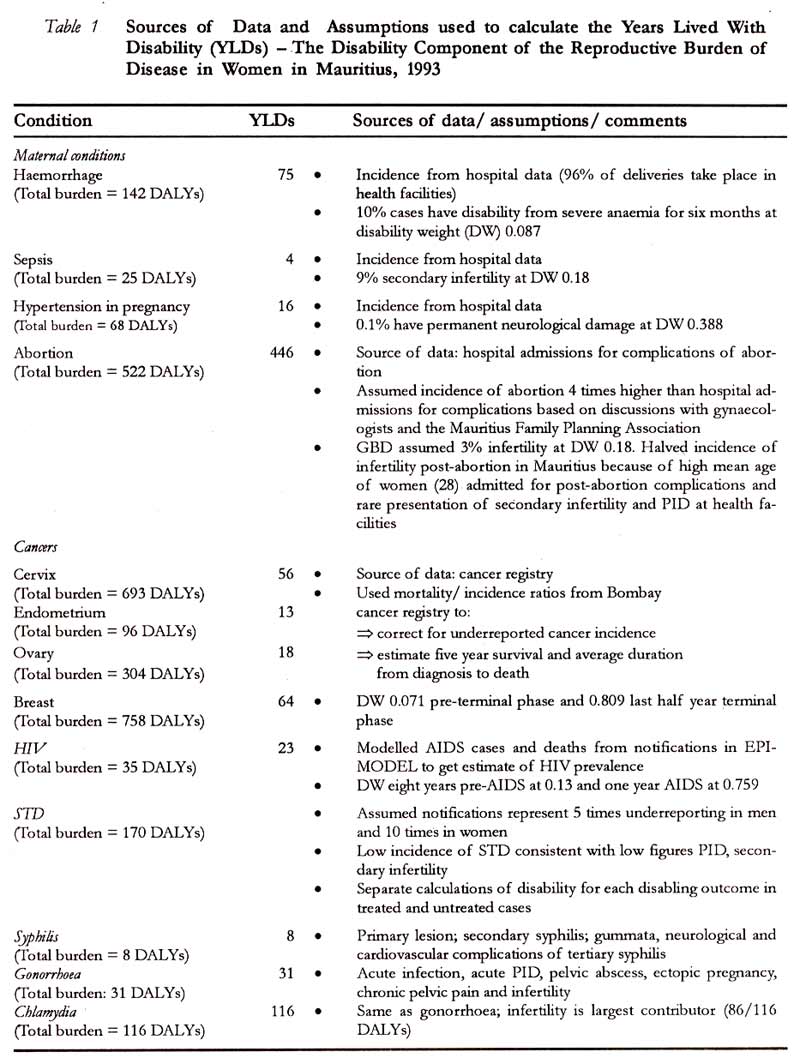
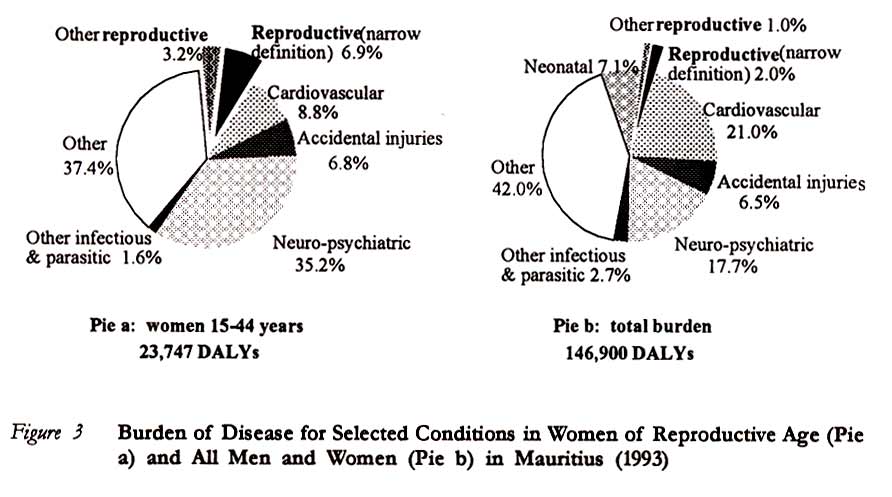
Australia Code Number: rh01004 ABSTRACT The 1993 World Development Report proposed a new paradigm to priority setting in health services. Two important steps in this approach are burden of disease estimates and cost effectiveness analyses that use disability adjusted life years (DALY) as the measure of health outcome. This paper explores how this methodology can be applied to estimate the size of the burden of disease caused by conditions currently considered the domain of reproductive health. Examples from the Global Burden of Disease Study and the Mauritius Burden of Disease Study are used to illustrate the strengths and weaknesses of this approach. While most of the criticism has centred on the assumptions of discounting and age weighting in the application of this methodology to priority setting, it is of far greater importance to examine the uncertainty of epidemiological and costing estimates. The conclusion is that however fraught with uncertainty, this approach to priority setting in health is an improvement over traditional influences on the decision-making process based on ranking of mortality alone, shaky assumptions of ‘preventable’ deaths or the most vocal advocacy groups. (Afr J Reprod Health 2001; 5[1]:31-39) KEY WORDS: Reproductive health, Global Burden of Disease, Mauritius, DALY Introduction The 1993 World Development Report (WDR), Investing in Health, examined the relationship between health, health policy and economic development.1 It identified misallocation of resources in public budgets, inequity, inefficiency and an explosion of costs as the four main problems in health systems. To redress these problems in developing countries, the report advocated that governments redirect health expenditure to a package of the most cost-effective, curative and preventive health interventions that do more to help the poor. Priority setting by selecting health interventions that give the best value for money requires quantification of the burden caused by all diseases and evaluation of the cost-effectiveness of health interventions that prevent the occurrence or reduce the severity of diseases. To this effect the WDR introduced the Disability Adjusted Life Year (DALY) as a single, comparable measure of health outcome to quantify premature mortality and disability from all diseases, at all ages, and for both sexes. The report estimated the global burden of disease in DALYs in 1990 and cost-effectiveness ratios for a selected number of health interventions in 'cost per DALY saved'. The ranking lists by disease burden and cost-effectiveness of interventions from the WDR have been widely quoted without much public scrutiny of the underlying epidemiological assumptions. This paper will explore the advantages, and limitations of this approach to set priorities within the domain of reproductive health and in relation to other health problems, illustrated by the Global Burden of Disease (GBD) estimates and examples from the 1993 Mauritius National Burden of Disease Study.2-3 Redefining Reproductive Health The 1994 Cairo International Conference on Population and Development proposed a broadened perspective for reproductive health programs. As yet, there is no clear consensus on which health problems and health services fall within the mandate of reproductive health. Family planning, sexually transmitted diseases (STDs), HIV/AIDs, reproductive tract infections, cancers and other gynaecological morbidities, infertility, maternal health, abortion and female genetial mutilation are generally included.4 Further suggested areas of relevance include sexual health, violence against women, anaemia, male infertility, and male reproductive cancers. As the discussion about the new mandate for reproductive health evolves, it is useful to quantify the relative importance of these reproductive health problems. The global burden of disease estimates provide the opportunity to make such comparisons. Burden of Disease Measurement in DALYs The DALY is a discounted and age-weighted, composite indicator of the future stream of life lost due to premature deaths and the future stream of healthy life forgone due to disabilities caused by disease. As a universal indicator of adverse health outcome, it allows comparisons of the disease burden by age, sex and geographical distribution. For global comparisons, DALYs lost due to mortality in all regions of the world are calculated using the same low-mortality model life table as a reference, where life-expectancy at birth is 82.5 years for women and 80 years for men. In national cost-effectiveness analyses it is more realistic to use the local life expectancy to quantify mortality. Disability weights based on opinions of disease experts using person trade off methods, determine the proportion of a year of healthy life deemed ‘lost’ in the presence of disabling disease. Disability weights take into account the functional loss of healthy life from disability in individuals. Through age weights, a higher value is attributed to years lived as young adults and the middle aged, arguing that at those ages people have a social responsibility to care for children and the elderly. DALYs are discounted at three per cent per annum on the assumption that this reflects the pure social rate of time preference.5 The Global Reproductive Disease Burden The GBD presents separate details of the disease burden from maternal conditions, including abortion, STDs, HIV and female reproductive cancers (of the breast, cervix, ovary and corpus uteri). Secondary infertility is considered as a disabling outcome of STDs, post-abortion and post-delivery sepsis. The burden from primary infertility and other gynaecological conditions is not estimated separately and at best, if at all, is hidden in a residual category of other genito-urinary diseases. It is not possible to separate violence against women from the general category of violence/homicide and the after-effects of rape from the overall category of post-traumatic stress disorder. Likewise, the estimates do not differentiate between sexually and non-sexually transmitted hepatitis B. Neither could one argue that all anaemia in women of reproductive age ought to be included in the reproductive health burden. Given the right epidemiological information, however, it would be possible to make such distinctions in the future. The following sections will use a narrow definition of reproductive health conditions (including maternal conditions, STDs, HIV and reproductive cancers) and a very broad definition (adding all anaemia, violence, post-traumatic stress disorder and 'other genitourinary disease' in women of reproductive age; and male reproductive cancers and morbidity). The narrowly defined group of reproductive health conditions accounts for 23.6% of the 1990 overall disease burden in women of reproductive age in developing countries, ranging from 8.0% in China to 39.7% in sub-Saharan Africa. All other conditions included in the broad definition of reproductive health only marginally add to these burden estimates in all world regions except China. Figure 1 shows the considerable geographical differences in the burden from reproductive health problems, expressed as DALY rates per 1000 women of reproductive age (based on data from the GBD). The narrowly defined reproductive conditions are responsible for 5.1% of the overall burden in men and women of all ages in developing countries. Inclusion of all broadly defined reproductive conditions raises this percentage to 6.1%. The fact that infectious and parasitic diseases (32.7%), accidental injuries (11.1%), neuro-psychiatric conditions (9.0%), cardiovascular diseases (8.2%), and perinatal conditions (7.3%) contribute a greater share to the total burden in developing countries puts the relative importance of reproductive health problems in perspective (Figure 2). The burden from perinatal conditions, which dwarfs even a 'generous' estimate of the reproductive health burden, deserves further attention. One could argue that a proportion of the perinatal burden is due to maternal conditions or lack of adequate obstetric care and, therefore, ought to be considered as a health outcome of reproductive health programs. Furthermore, there are two unresolved issues concerning the measurement of the burden from perinatal conditions. Firstly, at present, stillbirths are excluded from burden estimates while a neonatal death, inclusive of discounting and age weighting, accrues around 32 DALYs. It is an obvious anomaly that the difference can be so great between a fresh stillbirth and a newborn dying after one gasp. Secondly, the death of a woman of 30 years old during childbirth gives 29 discounted, age-weighted DALYs. One could argue that in many societies the death of a mother aged 30 years would be considered a much greater loss than an early neonatal death. While mortality accounts for most of the burden estimates for HIV and the reproductive cancers, disability dominates the burden from STDs and maternal conditions, in particular infertility after sepsis and obstructed labour; vesico-vaginal fistulae following obstructed labour; and to a lesser extent infertility after septic abortion, and anaemia following postpartum haemorrhage. The global burden of disease estimates for 1990 are based on the average occurrence of death and disability in eight large world regions. Inevitably, rather broad stroke generalisations had to be applied to fill in the large gaps of unavailable epidemiological, and in some regions demographic, information. Several updates of the 1990 GBD estimates have been made since the version 3 presented in the WDR to incorporate newly acquired epidermiological information and refinements of the disability weights used to value the loss of healthy life from disability.2,6 The Reproductive Disease Burden in Mauritius, 1993To illustrate the practical considerations involved in burden of disease assessments, this section presents details of the calculations of the burden from reproductive ill-health made for the 1993 Mauritius National Burden of Disease Study.3 The study used the same methods as were employed in the Global Burden of Disease Study. Mauritius is a small, densely populated, volcanic island with just over one million inhabitants in the southwest of the Indian Ocean. Rapid and sustained economic growth allowed Mauritius to move up from being a low income country at independence, 33 years ago, to its present status of an upper-middle income country.1 The Mauritian government provides a welfare state with access to free education, free public health care and invalids’ and old age pensions. In the last three decades, the country went through an accelerated demographic and epidemiological transition. The total fertility rate dropped from 3.6 in 1970 to 2.3 in 1993, and the infant mortality rate dropped from 60 to 20 per 1000 live births. MortalityThe effectively complete death registration in Mauritius facilitated the calculation of years of life lost due to premature mortality. Because over half of deaths occur outside health facilities, and autopsies are not performed for natural causes, there is more uncertainty about the accuracy of cause of death reporting. However, there are a number of indications that the registration of cause of death attribution is quite good. First, ill defined and senility codes are used in not more than 6% of deaths (less than 2% of deaths under 60 years of age and 11% in the elderly). Second, all deaths are certified by physicians. Third, an independent check of coding practices carried out as part of the Mauritius National Burden of Disease Study revealed that less than 8% of causes were wrongly coded, but only half of these cases had been assigned the code of a different disease category. Disability The estimation of the burden caused by disability was much more complicated and required information on the incidence, age of onset and average duration of each disabling outcome of disease. Routinely collected health service data were only useful for a few conditions in which health service utilisation is high and repeated episodes within a year are unlikely, e.g., complications of pregnancy and childbirth. Registers, e.g., for tuberculosis, cancer, HIV, and a variety of disabilities from a regional community-based rehabilitation project, and community-based surveys, e.g., for diabetes and ischaemic heart disease, provided the most accurate data on incidence. The available information on each condition was checked for internal consistency, making use of the DISMOD computer software, developed at the Center for Health and Population Studies, Harvard. This program is designed to assess whether assumptions about incidence, case fatality and remission are consistent with prevalence and mortality data, as well as estimates of the average age of onset and duration of the condition within each age category. Since data on the prevalence of most conditions was easier to obtain than incidence, the DISMOD program helped to estimate the most plausible incidence needed for the DALY calculation given a certain prevalence and mortality. Where no data were available, estimates had to be based on the judgement of disease experts in Mauritius or epidemiological studies conducted elsewhere. Table 1 gives details of the sources of data and the assumptions used to calculate the disability component of the reproductive burden of disease in Mauritius. The assumptions of duration, age at onset, probability of disabling sequelae and disability weights are based on those applied in the Global Burden of Disease Study. The burden of disease due to the 4 main reproductive health problems (maternal conditions, STD, HIV and reproductive cancers) in Mauritius makes up a relatively small proportion of the burden in women of reproductive age (6.9%), and still a smaller part of the total disease burden (2.0%). The burden from the other broadly defined reproductive conditions, most of which is attributable to anaemia, increases the reproductive burden by about 50% in both women of reproductive age and the whole population (Figure 3). The per capita rates of the reproductive burden of women of reproductive age in Mauritius are much lower than those of the six regions of the developing world depicted in Figure 1. In this respect, Mauritius even compares favourably with the estimates made for the region of established market economies (EME). The Mauritius burden rates for reproductive cancers and maternal conditions are similar to those in the EME region, but STDs and HIV are far less common in Mauritius. It is important to realise that the burden of disease in a country or region describes the gap between the current and 'ideal' health status, given all the health services and other endeavours to promote health that are in place. Prevention of maternal mortality and severe morbidity to a large extent depends on access to appropriate obstetric care. The low burden from maternal conditions in Mauritius reflects the success of its accessible health services in containing maternal mortality and morbidity. Therefore, the low ranking of maternal conditions in the burden of disease should not be interpreted as a license to divert resources from maternity services. The relatively high burden from perinatal conditions in Mauritius and a subsequent analysis of obstetric and neonatal services indicating inadequacies in the quality of care suggest that complacency about obstetric services is not warranted.8 There is scope for improvements in the technical efficiency of the current services to liberate resources that can then be directed towards obstetric and neonatal interventions to reduce the perinatal burden without compromising the successful containment of adverse maternal outcome. The presumed disability attributed to abortions, mainly due to infertility as a consequence of post-abortion sepsis, is one of the most uncertain estimates of the burden of disease in Mauritius. There was considerable uncertainty about the number of abortions. In a survey, the majority of women admitted for complications of abortion to public hospitals acknowledged that they had used a method to induce the abortion.9 In the absence of an accurate estimate of the incidence of abortion, we quadrupled the number of admissions in public hospitals for complications of abortion, arguing that not all induced abortions would lead to admission for complications and that a considerable number of abortions are performed in the private sector. It is clear that this was a rather bold guess. An additional argument to assume that abortions, despite their illegality, are frequently used as a method to regulate family size is that without these it is unlikely that Mauritius could have consistently sustained a total fertility rate below 2.5 for the last two decades with less than half of women using scientific methods of family planning. Further uncertainty entered the equation about the proportion of women who experience disability after an induced abortion. GBD calculations assumed that in developing countries 3% of women become infertile after an induced abortion. It was decided to attribute disability from infertility to only 1.5% of induced abortions in Mauritius, considering that pelvic inflammatory disease and secondary infertility are rarely diagnosed, and the fact that the average age of women admitted for complications of abortion is 28, an age at which most women in Mauritius have no further fertility wish and would therefore not consider themselves 'disabled'. Additional research would be needed to assess the validity of such assumptions. Priority Setting in Reproductive Health by Burden of Disease The above examples from the global and Mauritius burden of disease studies illustrate the attraction of quantifying adverse health outcome in DALYs. The use of a common metric allows comparisons between diseases with fatal and non-fatal outcome, at all ages and across geographical regions. The validity of burden of disease estimates greatly depends on the availability of demographic and epidemiological information. Unfortunately, the public discussion of the DALY methodology has concentrated on the assumptions of discounting and age-weighting which are of far lesser importance to the eventual results than the disability weights and the uncertainty of the epidemiological estimates fed into the calculations.10-12 Only recently, the disability weights used and methods used to derive these weights by person trade-off methods with 'experts' have been put in the public domain, allowing public scrutiny. A Dutch study determined disability weights using methods similar to those of the GBD and found good correspondence between the weights derived from both studies.13 Further work is needed to determine whether the GBD disability weights reflect societal preferences for health states across different cultures and between different groups in the society. However, improvements of epidemiological estimates generally will have a much greater bearing on accuracy of burden of disease estimates than the smaller changes brought about by using different assumptions of disability weights. The findings of sensitivity analyses of the Mauritius study are encouraging to those who advocate the use of DALYs in prioritisation. The order in which diseases are ranked according to their share of the burden is quite insensitive to relatively large fluctuations in the estimates of the incidence of disabling diseases.3 Ranking of conditions by their relative contribution to the burden of disease is not sufficient to set service priorities. There may be no effective interventions known for some conditions with a large share of the burden, while other conditions responsible for a smaller burden may already be effectively dealt with by the health services (as illustrated in the above example of maternal conditions in Mauritius) or may produce further health gains at low cost. Such additional information on the cost-effectiveness of health interventions should accompany burden of disease estimates.13 However, there are major gaps in the required epidemiological and economic knowledge about costs and effectiveness of health interventions to allow detailed lists of priorities to be made. Information about the efficacy of many health interventions is lacking and even less information is available about the effectiveness of such interventions when delivered through routine health services with the eventual health gain reduced through limited uptake and less than ideal delivery of the service. A further complication is that contextual factors influencing costs and effectiveness make generalisation of cost-effectiveness data difficult. The limitations of the available information about most effectiveness ratios to a few broad categories - 'very', 'quite a bit', 'somewhat' and 'not at all' cost-effective - rather than the detailed figures of cost per DALY saved presented in the WDR. Nevertheless, even such broad categories can provide useful comparisons because costs per DALY saved often vary by orders of magnitude. The WDR presents examples of 47 interventions ranging from US$1 to more than US$10,000 per DALY1 Evaluation of the cost-effectiveness ratio (in 'cost per DALY saved') of family planning programs in comparison to other health interventions runs into a number of sticky issues. Unlike other health interventions, family planning services aim to prevent not only adverse health outcomes, but also the births of people with the expectation of a healthy stream of life. Taking this argument to extremes, one could argue that family planning programs actually cause the loss of many DALYs. A further problem is that cost-effectiveness ratios ignore any benefits beyond the prevention of premature mortality or disability. Increased educational and vocational opportunities for women are examples of such additional benefits to individuals of family planning programs. Neither is this sort of economic analysis suited to take into account the potential economic or social benefits to society of containing population growth, which a family planning program may provide. The cost-effectiveness ratios given for family planning programs in the WDR are simply based on an estimate of the expected reduction in maternal and neonatal motality (converted into DALYs) as a consequence of a reduced number of pregnancies and births. In conclusion, there are many arguments to be cautious about the use of burden of disease and cost-effectiveness analyses to inform decision-making about health sector reform, in general, or health service priorities in reproductive health programs, in particular. On the other hand, however fraught with uncertainty this approach to priority setting in health is an improvement over traditional influences on the decision-making process, based on ranking of mortality alone, shaky assumptions of 'preventable' deaths or the most vocal advocacy groups. The details about the methodology presented in this paper should equip the reader with insight to judge the merits and weaknesses of the method. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01004f2.jpg] [rh01004f1.jpg] [rh01004f3.jpg] [rh01004t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}