 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol.
5, No. 1, August, 2001 pp. 40-49
Utilisation of Reproductive Health Services by Adolescent Boys in the Eastern Region of Ghana Addie Koster1, Julia Kemp2 and Aaron Offei31Masters of Community Health student (1998), Liverpool School
of Tropical Medicine, United Kingdom. Code Number: rh01005ABSTRACTIn Ghana few studies have investigated the reproductive health needs of adolescent boys. The aim of this study was to find out sources of reproductive health information for boys and the reasons for their low/non use of public health services. Qualitative methods were used, including focus group discussions, semi-structured and informal interviews. Findings suggest that adolescent boys receive little reproductive health information from schools, parents or health services and there are several barriers to accessing public services, such as age restrictions and hostile staff attitudes. Instead, boys learn about sexual issues from their peers and the media, and seek reproductive health care from private practitioners, such as pharmacists and herbalists. (Afr J Reprod Health 2001; 5[1]:40-49) KEY WORDS: Adolescent boys, reproductive health services, information, contraceptives, sexually transmitted infections, Ghana Introduction The population of adolescents (10-19 years old) in the developing world is estimated to be 914 million.1 In the early 1990s, concern about adolescents focused on their increased exposure to pre-marital sex, resulting in a higher incidence of teenage pregnancies, especially out-of-wedlock.1-7 At the International Conference on Population and Development in Cairo (ICPD 1994), governments were urged to focus more on the specific reproductive health needs of adolescents,2 emphasising the role of men in reproductive health.8 Boys’ involvement in reproductive health initiatives is important, both in the interest of young women’s reproductive health and to address their own reproductive health needs.9 Published studies from developing countries suggest that there are many barriers to adolescents’ involvement in reproductive health programs. Lack of information from formal sources is cited as one of the main problems. For example, adolescents in Nigeria, Kenya10,11 and Zimbabwe12 suggest that discussing sexual issues with parents is a taboo. Parents rarely seem to disseminate sex education to their children13 but prefer to rely on the educational system.14 Family life education (FLE) programs in schools are designed to cover reproductive health issues, but are either not implemented at all (in Nicaragua,15 Taiwan,16 Nigeria and Kenya10) or their scope and quality vary considerably. Furthermore, school programs often do not address the needs of out-of-school youths.12 Alternative sources of information are limited. Few reproductive health services are accessible to adolescents. Conventional maternal and child health/family planning (MCH/FP) services seem to target mainly older, married populations, predominantly women.1,5,13,17,18 Demographic health surveys in 11 sub-Saharan countries found that many of these services are inappropriate for young people because of the lack of experienced staff to counsel the youth, and adolescents’ inability to pay for services.19 Other evidence suggests that lack of knowledge of the location of family planning services,12,20 restrictions on access for the unmarried,21 and staff disapproval of young people using contraceptives also present barriers.15,22 Increasing evidence suggests that adolescents seek reproductive health information and care from a variety of non-formal sources. Peers seem to be an important source of information10,20,23 but may also apply undue pressure on adolescent boys.24 Recent studies from Ghana show that adolescents often frequent private services to obtain contraceptives, such as pharmacies and chemists (known locally as 'chemical sellers').25-27 In general, adolescent health literature does not elucidate the differences in awareness of reproductive health and health services between adolescent boys and girls, because many studies do not report findings according to sex. Furthermore, with the exception of a few targeted studies on adolescent boys,2,9,28 specific studies about their needs are rare. In developing countries young men often appear to be neglected in pregnancy prevention and FLE programs, despite their considerable influence in initiating sexual intercourse.29,30 In Ghana, with an estimated total population of 18.1 million,31 one in five people is an adolescent.32 Several studies found the serious lack of reproductive health knowledge amongst youth to be the main reason for their low/non-use of (formal) contraceptives, which has contributed to the observed increase in teenage pregnancies in recent years.3,10,20,24-26,33-36 Following the ICPD, the Ghanaian National Population Council designed an adolescent reproductive health policy, recommending a specific approach to adolescents in reproductive health programs.37 Against a background of rising rates of teenage pregnancies, the Ministry of Health (MOH) in the Eastern Region of Ghana has been eager to increase the involvement of adolescent boys in reproductive health programs. Therefore, a collaborative study was planned between the MOH and the Liverpool School of Tropical Medicine (LSTM), United Kingdom. The aims of this study were:
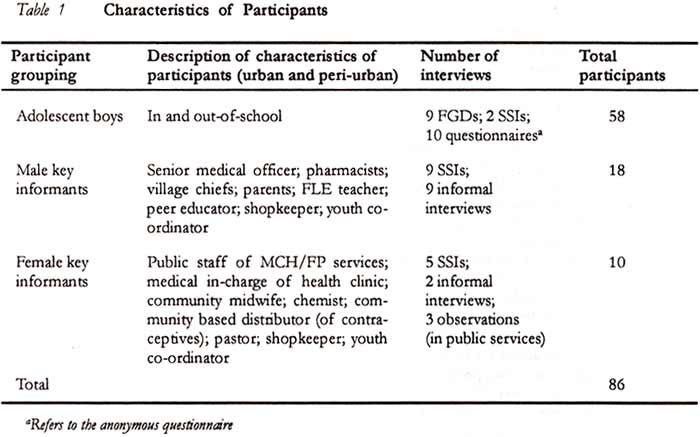
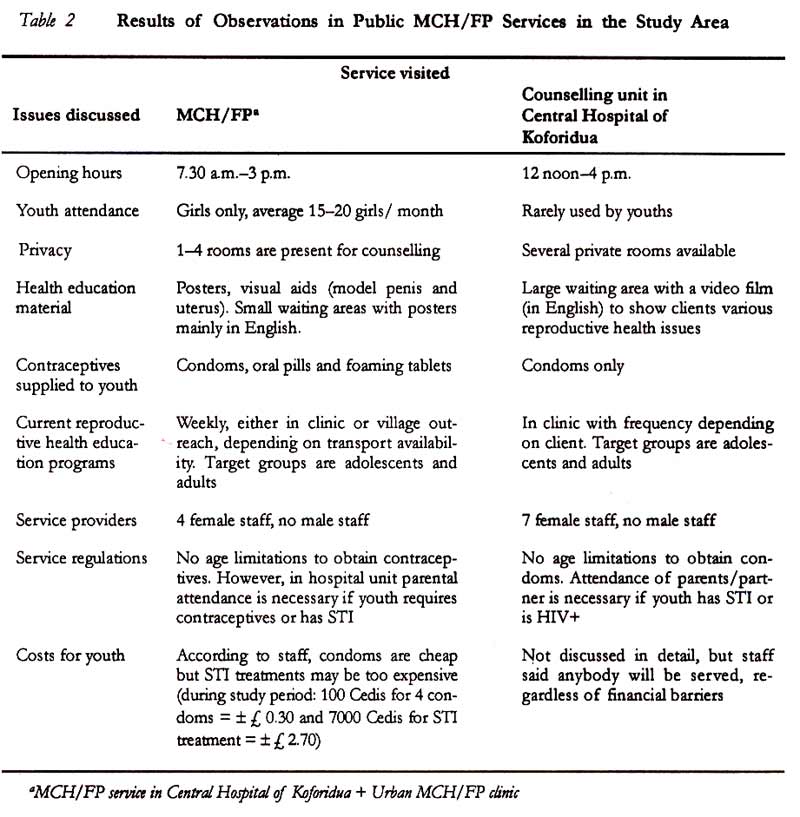
Methods This study was conducted between July and November 1998, and it included eight weeks of fieldwork. The study took place in and around urban Koforidua, the capital of the New Juaben District in the Eastern Region of Ghana. Two peri-urban communities were included in the study. The principal author, a master’s degree student of the LSTM, and two health professionals seconded by the MOH (one male and one female) collected data. The main study participants were male adolescents between 15 and 19 years old, both in and out-of-school, with different levels of education. Key informants with special knowledge about the youth were also interviewed. These included public and private providers of reproductive health services, FLE teachers, opinion/religious leaders and parents of adolescent boys. Adolescents were contacted through two local youth co-ordinators and the medical in-charge of health clinics. Key informants were jointly recruited by the medical in-charge and the two MOH research team members. Individual, verbal informed consent was sought from the study participants, with emphasis on their freedom to withdraw at any time. The study was primarily qualitative, including focus group discussions (FGDs) with adolescents, semi-structured interviews (SSI) with adolescents and key informants and participant observation. In addition, school attendees completed an anonymous self-administered questionnaire, and structured observations were made in public MCH/FP services. All interviews were recorded (with permission), transcribed and, when necessary, translated by the study team. Data analysis was carried out through an inductive process of identifying themes38 based on the interview topic guides for focus group discussions and checklists for semi-structured interviews. Participant checking (asking comments on notes made during interviews) and cross-checking (verification of findings with the study team members) took place regularly. This enhanced the trustworthiness of data through correction of misinterpretations.39 Altogether, nine focus group discussions, 16 semi-structured interviews and 11 informal interviews were conducted (Table 1). Findings Sources of Information on Reproductive Health for Adolescent Boys There are few formal sources of information for adolescent boys on reproductive health issues, and the need for more information for the youth was widely recognised. Family life education (FLE) programs are not yet fully integrated into the national school and many of the in-school boys said FLE was irregular or non-existent. Teachers were concerned about the lack of access to FLE for the out-of-school boys. Boys commonly felt that FLE could potentially assist them in resisting peer pressure to engage in sex. Although one female key informant felt that boys’ access to information should be restricted because "...if not, they will use sex as drinking water..." The majority of key informants shared the following view: "Because we know they do it, it is better to talk to them and to advise them at the same time to abstain. They have to know the availability of condoms and how to get them; to assume that they don’t do it is dangerous." The majority of boys (in and out-of-school) felt that both public and private health care staff do not provide sufficient information to the youth about contraceptive use and prevention of sexually transmitted infections (STIs). This was expressed even though local MOH staff conducted regular outreach visits to schools and community centres in the area. Most of the out-of-school boys said they did not have any gatherings for formal teaching, unlike in-school youths. A shared view across the key informant group was that boys generally lacked information on the location and programs of public health services as well as specific information on condom use. This view was supported during FGDs when many boys asked how to prevent a condom from 'bursting' and whether they should put on several condoms instead of one. Many boys (in and out-of-school) said their parents were afraid to talk to them about sexuality in case it encourages promiscuity. Fear of parental disapproval prevented some boys from becoming involved in youth-focused initiatives such as peer distribution of contraceptives. Additionally, boys generally felt that parents provided more information to girls, as one FGD, urban, out-of-school boy said: "... because the girls have to know their rights". Key informants (including parents) agreed that most parents do not talk about sex with their children because of their own lack of knowledge and, therefore, they feel shy. One male key informant felt that most parents "neglect" their sons, because parents do not know boys' particular reproductive health needs. Some female key informants said boys mostly learn "from the street". Key informants commonly expressed a wish to be given more information about reproductive health, so that they could teach the youth more accurately. Sources of reproductive information for boys were largely informal. Most boys said they rely on their peers for information. Urban boys also added that their teachers and the media provided information. Out-of-school boys (urban and peri-urban) said they occasionally receive reproductive health information from village chiefs. Many respondents suggested areas in which reproductive health information could be augmented. Several community members (male and female) pointed to the historical importance of puberty rites in informing the youth about sexual health. In the words of one of them: "The most important was the moral aspect where they taught us when you should become a man. Unlike today, now we have to look between religion and culture, Presently, we have a headache about what to teach the youth, probably the two have to come together." Boys asked to receive more information about puberty changes, STIs/AIDS and how to cope with the different pressures they find themselves under. The majority of boys, especially those who were out-of-school, asked for regular FGDs to discuss their queries and said it was the first opportunity they had to talk openly about reproductive health issues. Reasons for Use/Non-Use of Current Reproductive Health Sciences In the study area, formal reproductive health services are provided through MCH/FP clinics, either hospital-based or as separate units. There are 209 MCH/FP institutions in the 15 districts of the Eastern Region providing integrated services, including contraceptive supplies and counselling. Clients include both adolescents and adults.40 Three centres were visited as part of this study An overview of the services offered in these centres is given in Table 2. (Note: the MCH/FP service in the Central Hospital of Koforidua and another urban MCH/FP clinic are grouped together because they are set up similarly and liaise regularly with each other.) Observations in the three centres revealed that although adolescents may be target clients, there are several obstacles to their utilising the services. For adolescents in general, opening hours correspond with school times; most educational materials are in English; charges are incurred for services; attitudes towards young clients may be negative and the attendance of parents is requested if the adolescent client has an STI. In terms of barriers for adolescent boys in particular, staff in the facilities said there is no opportunity to consult a male health care worker. Staff felt that they lacked resources for outreach activities, in particular appropriate educational materials and transport. Most adolescents and key informants spoke of barriers to boys’ access to formal reproductive health services. The problem mentioned mostly amongst all different groups of boys was their shyness to ask female staff for condoms. Peri-urban out-of-school boys talked of "being afraid" to tell providers about their reproductive health problems. In the words of one boy (FGD, urban, in-school): "The boys, they feel often shy to go to the doctor, because when you go there they tell you you should go and bring your partner. So, sometimes you feel shy to mention that so you go to the herbalist and do what he prescribes." Key informants (male and female) confirmed the perception of boys' shyness, and some private providers (urban, male) added that as a result, boys often use their own 'language', for example, calling condoms 'socks' or a 'bullet.' Staff attitudes were also mentioned as barrier. Many boys (mostly in-school, since many out-of-school boys said they rarely go to public services) expressed that public health staff often told them that they were too young to buy condoms and were often sent away. They felt that nurses in particular were unfriendly, and sometimes insulted them. As one boy summarised (FGD, urban, out-of-school): "Sometimes when you go, they look at your features and they feel that you an not of age. They ask a lot of questions, like; 'who sent you?' 'You are too small.' This is what they say and they send you away." Boys across all groups felt that pharmacists or chemists are friendlier, ask no questions, but if requested will provide information. Key informants had varying views. A few public and private providers (male) felt that public staff sometimes shout at adolescents and are not receptive to their needs, whereas other public health staff (female) felt that "boys generally don’t care to come to the services." Lack of privacy and confidentiality in public health services was felt by the majority of boys (urban and peri-urban in-school) to hinder their access. Boys said they feared that staff would inform their parents about the purpose of their visit to the service. One boy summed up the common feeling (FGD, in-school): "Like me, if I go to the service and I am looking for a condom, they inform my mother [all participants agree with 'hmm']. But I came there for these reasons and then my mother will do something to me, so I feel shy, I am afraid to go, and rather contact my friends." Amongst key informants, opinions differed. While public providers in general had confidence in the privacy of their service, a minority of other key informants (in particular males) felt that boys sometimes face problems because their relatives work in the service. In all interviews with boys, the absence of male staff was felt to be a significant barrier, and their views are summarised in the following statement made by one boy (FGD, out-of-school): "We prefer males for counselling because we are all men and we all have the same thing."Amongst all key informants, there was a consensus about boys' reluctance to approach female staff for reproductive health issues. However, a small minority of public providers (females) felt that male staff would not make a difference for boys' attendance. Boys (in and out-of-school) also reported that public services were expensive and frequently not open. The majority of key informants (male and female) also felt that hospital cost (such as for investigations) could be a problem for adolescents. Despite the various negative points about public services, a minority of boys of all groups said that public health services provide effective treatments and have qualified staff. Most participants said, in addition to public services, contraceptives and STI treatments can be obtained through alternative providers in the area such as pharmacists, herbalists, 'quack doctors' (although not formally trained, they are diagnosing and dealing with medicine), traditional birth attendants and 'walking carriers' (women who sell medicines). Most boys (in and out-of-school) said that they frequent pharmacies and chemists to obtain condoms but go to the hospital for STI problems. However, further probing during one FGD (peri-urban, out-of-school) revealed that they often go first to see the herbalist, for reasons of confidentiality and cost. While boys in general were not always aware of the availability of public health service programs, they had good knowledge of the location and supplies of alternative providers. Youth-Focused Initiatives in the Eastern Region There are several NGO initiatives in the Eastern Region of Ghana that specifically target youths. The Philip Foundation and the Centre for National Culture (CNC) both use drama to raise awareness of reproductive health issues. Local NGOs have also developed their own FLE programs for adolescents (in and out-of-school). The Philip Foundation initiates FLE clubs in schools, and at the time of the study there were 33 FLE clubs in the area for the 14-33 years age group. The Planned Parenthood Organisation of Ghana (PPAG) run their own FLE clubs in 30 schools (figures per September 1998) and MCH/FP services at four locations in the Eastern Region. In their programs, youth volunteers are selected by community members to be distributors of contraceptives to peers. In the 1990s, the PPAG started 'Young Men’s Clubs' and 'Daddy’s Clubs' specifically for adolescent boys and men, providing them information on several reproductive health issues. Although the organisations described are mostly located within Kofondua centre, there was limited awareness among the study participants about their adolescent-focused programs. Most boys (mainly urban and in-school) were aware of the PPAG services, but not always of the programs of non-governmental organisations (NGOs). A few boys also mentioned NGOs as a source of contraceptives. Across all groups, boys clearly supported the involvement of youth in reproductive health programs. In the words of one boy (SSI, in-school): "The boys, we want people like our types to teach us, not very old because we may waste some time of intimacy because the person may be too old for us and the boy may feel shy to contact him or seek advice on that issue. So, we have to have young people so that they can be trained and teach the young people in the communities all about it." Study LimitationsThis study represents an initial investigation, and was restricted by the time available. As a result, fewer out-of-school youths were included in the study because of difficulties experienced in recruiting them. This has 'advantaged' the answers of the in-school youths. The marital status of adolescent participants was not included as a factor in the selection criteria. This limits the study findings, since marital status may influence reproductive health needs. For example, married adolescents may have highlighted different problems in coping with the responsibilities of parenthood and their access to information and support. It was found that alternative, non-formal care providers are an important source of reproductive health information and care for adolescents. It was not possible to investigate these non-formal services within the time available. It is recommended that complementary follow-up investigations should include a quality audit of services provided by alternative practitioners and a comparison of the reasons for girls' use/non-use of reproductive health services. Discussion It is clear from the findings that adolescent boys in the study area lack information on reproductive health issues. Many other studies, including those from Ghana, have drawn attention to the need to improve adolescents' knowledge of contraceptive use, prevention of pregnancies and STIs.3,10,20,24-26 However, in addition to technical knowledge, boys need to understand the norms and values in sexual relationships. The observed interest of the youth in reproductive health issues suggests that an expanded and holistic program of health promotion may be successful. In a review of sub-Saharan countries (including Ghana), it was reported that parents are often reluctant to allow the provision of reproductive health information to youths through schools.14 In the study area, although key informants admitted that talking about sexual issues with the youth is a sensitive subject, they clearly expressed a need to improve their own knowledge in order to pass on necessary information to them. Initiatives where parents learn these skills have proven to be successful in the Philippines and Tanzania.13 'Daddy’s Clubs' run by the PPAG in the study area provide an example, which could be expanded, to improve gatekeepers' education and involvement in adolescent reproductive health. FLE has recently been included in Ghana’s national school curriculum, but in the study area the teaching is irregular and may not achieve the desired impact. Furthermore, out-of-school youths have difficulties accessing both FLE and MOH school-based educational programs. However, there are a number of local NGO-led initiatives (by the PPAG and Ghanaian National Youth Council) that provide FLE programs for the youth in places where they gather. PPAG also trains youth to be peer educators and community-based distributors of contraceptives. These activities are consistent with successful examples of peer education in other countries.11,30,43 All NGOs in the study area mentioned their lack of resources to carry out the scale of activities that they consider necessary. Rather than duplicate activities, this area provides an opportunity to explore the role of partnership between the MOH, MOE and local NGOs to offer a comprehensive program for both in and out-of-school youths. Such co-ordination may provide greater accessibility for the youths and allow effective use of available resources. Another major problem for boys in the study area is their lack of access to reproductive health services. The reasons are diverse, from boys' reluctance to approach predominantly female staff; organisational issues, such as the lack of privacy and inconvenient opening hours. Reorganising existing public MCH/FP services may be difficult for the MOH, but certain measures could be taken to make these services more 'boy-friendly For example, eliminating the requirement that young people must bring their parents, providing a condom dispenser in a discrete location, and changing opening hours. Other measures to consider include employing male staff and having 'male-only' hours. Such initiatives have proved to be successful in improving men’s participation in reproductive health in Zimbabwe42 and Colombia.8 Public health staff may also draw upon the non-didactic, youth-friendly approach of the local NGOs in developing adolescent-focused services. The majority of study participants suggested setting up separate health centres for adolescent boys and girls. There are several examples of such centres from various countries.43-45 However, a study conducted in Mexico found that peer outreach workers were cost-effective and reached more unmarried young men, while youth centres reached more unmarried young women. 13 Another limitation of youth centres is that they are often urban-based and do not serve peri-urban or rural adolescents. It is important that youth centres offer innovative outreach activities such as village drama and puppet plays.41 In addressing the reproductive health needs of adolescent boys/youths it is important not to ignore the major health providers to the youths. In the study area, most young men seek reproductive health care from alternative sources such as pharmacies, herbalists and private community health workers. The health sector in Ghana, therefore, has a responsibility to improve the quality of care of these alternative providers. For example, a more consistent policy of training pharmacists and other private practitioners could be put in place by the MOH, supported by regular monitoring. In this way, common goals in reproductive health service provision for adolescent boys can be developed while providing more outlets to underserved youth populations. This is consistent with recommendations of other studies in Ghana.3,33,40 In this region of Ghana there is a background of interest in reproductive health of adolescent boys. This is evident from the MOH in commissioning this study, other local ministries,46 and from the study participants themselves.47 In the context of Ghana’s health sector reforms, it may now be possible to develop a district health strategy for the youth, which involves partnerships with the MOH, MOE, local NGOs, churches and private practitioners. Young men could be involved in district youth teams and participate in the design, implementation and evaluation of reproductive health programs. Promoting the increased involvement of young men in reproductive health, therefore, seems to be an achievable goal in the Eastern Region of Ghana. Acknowledgements This study was conducted for a dissertation in partial fulfilment of the degree of Masters of Community Health. The write up for publication was supported by a grant from the Katherine Elliot Award Fund. The authors thank Paul Gamer, International Health Division, Liverpool School of Tropical Medicine and Rumona Dickson, Research and Development Support Unit, University of Liverpool, for their helpful comments on an earlier draft of this paper. We acknowledge the generous support of the Regional Health Administration, Eastern Region, and we are particularly grateful to the adolescent boys and the community for their enthusiastic support and willing participation. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01005t2.jpg] [rh01005t1.jpg] |
| |||||||||

{kind=link}
{kind=link}