 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 5, No. 1, August, 2001 pp. 50-55 Prevalence of Gardnerella vaginalis in Pregnant Nigerian Women JIB Adinma1, NR Okwoli2, Agbai3 and N Unaeze4 1Department of Obstetrics and Gynaecology, College of Health
Sciences, Nnamdi Azikiwe University, Nnewi Campus. 2Department
of Medical Microbiology, College of Health Science, Nnamdi Azikiwe University. 3 Department
of Community Medicine, College of Health Sciences, Nnamdi Azikiwe University. 4Department
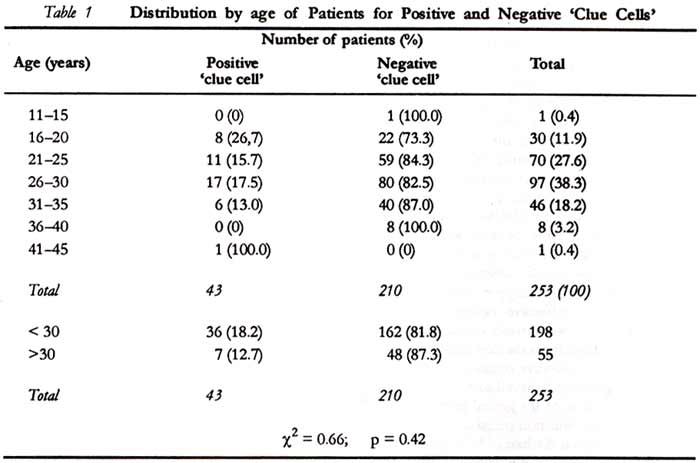
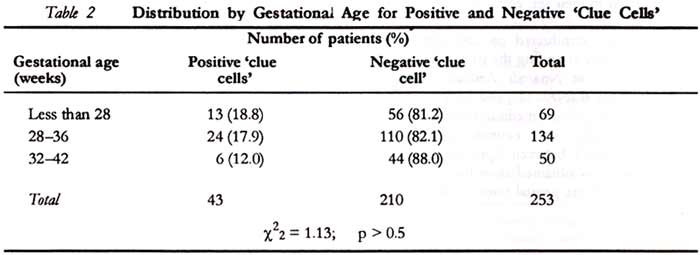
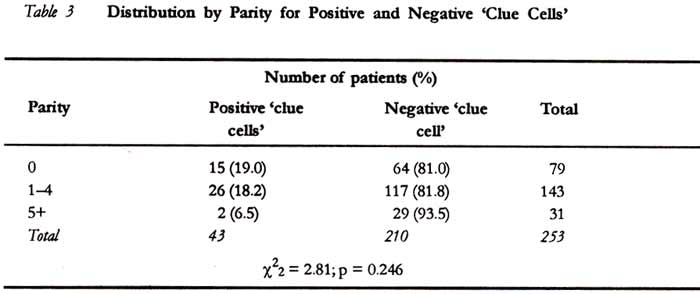
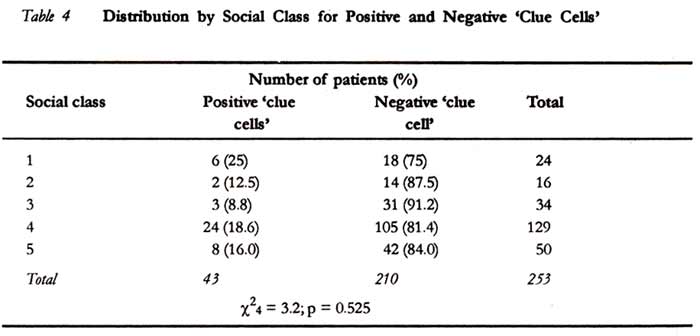
of Microbiology, University of Nigeria, Nsukka. Code Number: rh01006ABSTRACTThe prevalence of Gardnerella vaginalis in the genital tract of 253 pregnant Nigerian women was 17.0 % (43). The highest prevalence occurred among women aged 16-20 years (26%) while the lowest occurred among those aged 31-35 years (13%). Women aged 30 years and below had an overall prevalence of 18.2% while those above 30 years had a prevalence rate of 12.7%. This difference was not significant (c2 = 0.66; p = 0.42). There was a decline in the prevalence rate of G. vaginalis with increasing gestational age being 18.2% for pre-term gestational age (i.e., below 37 weeks) and 12.0% for term gestational age (37-42 weeks), although the difference was also not significant (c22 = 1.13; p > 0.5). Similarly, a non-significant decline in the prevalence of Gardnerella vaginalis occurred with increasing parity from 19% in the primigravida to 6.5% in the grandmultipara (c22 =2.81; p = 0.246). No definite trend occurred in the prevalence of G. vaginalis for social class (c24 =3.2 p = 0.525). The pattern of prevalence of Gardnerella vaginalis in the genital tract in pregnancy suggests an indirect relationship with pregnancy sexuality, which needs to be corroborated with further larger studies. (Afr. J Reprod Health 2001; 5[l]:50 - 55) KEY WORDS: Gardnerella vaginalis, prevalence, Nigeria, pregnant women Introduction Pregnancy is a special physiological state associated with gross alteration in the hormonal status of the woman, and this considerably affects both her emotional and physical state. Hence, a noticeable change in lifestyle particularly in sexual behaviour occurs.1,2 Pregnancy hormones encourage the growth and deposition of glycogen in the vagina, and this together with the effect of Doderlein’s bacilli (Lactobacillus acidophilus) alter the pH status of the vagina and influence considerably the microbial flora of the genital tract of the pregnant woman.3 G. vaginalis either alone or in combination with other organisms, notably Mobilunucus specie, Mycoplasma hominis and some obligate anaerobes has been recognised as the causative agent for bacterial vaginosis - a non-specific vaginitis believed to be sexually transmitted and may present clinically as a homogenous gray offensive vaginal discharge.4,5 Bacterial vaginosis is invariably characterised by a shift in vaginal flora from the dominant lactobaccilus species to its causative organisms, notably G. vaginalis. G. vaginalis is believed to be the predominant bacterial isolate of the genital tract of women - both pregnant and non-pregnant - especially when there is vaginal discharge.3,6,7 In pregnancy it has been incriminated in the pathogenesis of premature rupture of membrane (PROM), chorioamnitis and pre-term labour. 8,9 This study examines the prevalence of G. vaginalis in 253 Nigerian pregnant women with or without vaginal discharge, especially in relation to their age, gestational age, parity and social class. Subjects and MethodThe study was conducted on 253 consecutive pregnant women attending the principal author’s antenatal clinic at Nnamdi Azikiwe University Teaching Hospital (NAUTH) and Summit Specialist Hospital (a private medical centre), both at Nnewi in Anambra State, eastern Nigeria, over a nine-month period, between April and December 1993. A swab was obtained from the posterior or lateral fornix of the genital tract of each subject; the specimen was gram-stained and examined for 'clue cells' using a microscope. The age, parity and gestational ages of the women were documented. The social classes of the women were determined from Olusanya’s10 classification, making use of the educational status of the woman and her husband’s occupation. The collected data were analysed for positive and negative 'clue cells' for the variables using comparative percentages and chi-square (c2 )test. ResultsThere were 43 'clue cells' - positive cases, out of 253 subjects, giving a prevalence rate of 17.0%. Table 1 shows the distribution of the women by the presence or absence of 'clue cells for age. The highest prevalence of Gardnerella vaginalis occurred among women aged 16 - 20 years (26%) while the lowest occurred among those aged 31 - 35 (11%). Women aged 11 - 15 years and 41 - 45 years (one each) were too few to be included in the comparison. Gardnerella vaginalis generally occurred in 18.2% of women aged <30 years, compared with 12.7% in women >30 years. The difference was not statistically significant; c2 = 0.66, p = 0.42. The distribution of gestational age, as shown in Table 2, indicates a decline in the prevalence rate of Gardnerella vaginalis, with increasing gestational age being 18.2% (37) for pre-term gestational age, i.e., 37 weeks and 12.0% (6) for term gestational age (i.e., 37 - 42 weeks). The difference was not statistically significant; c2 = 1.13, p > 0.5. Similarly, a non-significant decline in the prevalence of Gardnerella vaginalis occurred with increasing parity from 19% in primigravida to 6.5% in grandmultipara, c22 = 2.81; p = 0.246 (Table 3). Table 4 shows no definite trend in the prevalence of Gardnerella vaginalis for the social class of the women studied; c24 = 3.2, p = 0.525. Discussion The prevalence of Gardnerella vaginalis in pregnancy from this study, 17%, is quite low when compared with a prevalence rate of 40.8% observed among non-pregnant women from the same study area; 11 although the later group of women had vaginal discharge, unlike the present study that was conducted among women with or without vaginal discharge. Previous reports have, however, indicated high isolation rate of Gardnerella vaginalis even in asymptomatic women.12,13 Totten14 isolated Gardnerella vaginalis in 69% of women without any sign or symptom of infection. This implies, therefore, that this organism may be part of the normal vaginal flora of some women15, remaining relatively quiescent but playing opportunistic role following alteration in the complex balance of vaginal organisms. There is, however, a general consensus that higher isolation rate of Gardnerella vaginalis occurs in symptomatic compared with asymptomatic women. The role of pregnancy in the relatively low prevalence of Gardnerella vaginalis in pregnant women is not clear. Perhaps, pregnancy, by lowering vaginal pH, prohibits the growth of Gardnerella vaginalis known to thrive in alkaline medium.11,12 Observations from our previous report on pregnancy sexuality2 suggest an indirect relationship between the frequency of sexual intercourse and the prevalence of genital tract Gardnerella vaginalis. The corollary to this is the reported high prevalence of Gardnerella vaginalis infection associated with sexual promiscuity.17 This study has shown that the prevalence of Gardnerella vaginalis was lower at term gestational age (12.0%) compared with pre-term (18.2%), in consonance with the usual pattern of sexual frequency during pregnancy.1 Reduction in sexual activity at term is believed to be due to decline in sexual desire borne out of a fear of injury to the fetus, inducing labour or difficulty in finding a suitable position for coitus late in pregnancy.1,18 This study also showed that a higher prevalence of Gardnerella vaginalis occurred at younger maternal age and earlier parity. Women of 30 years and below had a higher prevalence of Gardnerella vaginalis (18.2%), compared with women above 30 years (12.5%). Women of lower parity (0.4) had a higher prevalence rate of Gardnerella vaginalis (18.5%), compared with the grandmultiparous women (para = 5 and above), 6.5%. Although these differences did not reach significant proportions, a definite trend, however seems to emerge. It is tempting to suggest that the younger, pregnant mothers who are also likely to be of lower parity are more likely to have higher frequency of sexual intercourse than the older pregnant women, particularly the grandmultipara, and by implication, therefore, a higher incidence of Gardnerella vaginalis infection. However, our earlier study on sexual activity during pregnancy did not ascribe any definite pattern of sexual frequency in relation to maternal age and parity.2 The prevalence of Gardnerella vaginalis showed no trend in respect of the social class of the women studied. This also agrees with the finding on the pattern of sexual activity during pregnancy, which similarly showed no trend in respect of social class.2 Findings from this study unequivocally ascribe a relationship, albeit indirect, between pregnancy sexuality and the prevalence of Gardnerella vaginalis in pregnancy. This relationship needs to be corroborated by a more in-depth study involving a larger number of pregnant women. The study is furthermore expected to corroborate observed trend from the present study, in the prevalence of Gardnerella vaginalis with maternal age, gestational age, and parity, which may perhaps reach expected significant proportions. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01006t4.jpg] [rh01006t1.jpg] [rh01006t3.jpg] [rh01006t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}