 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 5, No.
1, August, 2001 pp.
66-74
Tracing Condom Fates: Design and Pilot Results of a Study Investigating the Use and Wastage of Public Sector Condoms Landon Myer1’2, Catherine Mathews1’3 and Francesca Little4 1Centre for Epidemiological Research
in South Africa, South African Medical Research Council 2Department
of Social Anthropology, University of Cape Town. 3Department
of Public Health, Universi!y of Cape Town. 4Department of Statistical
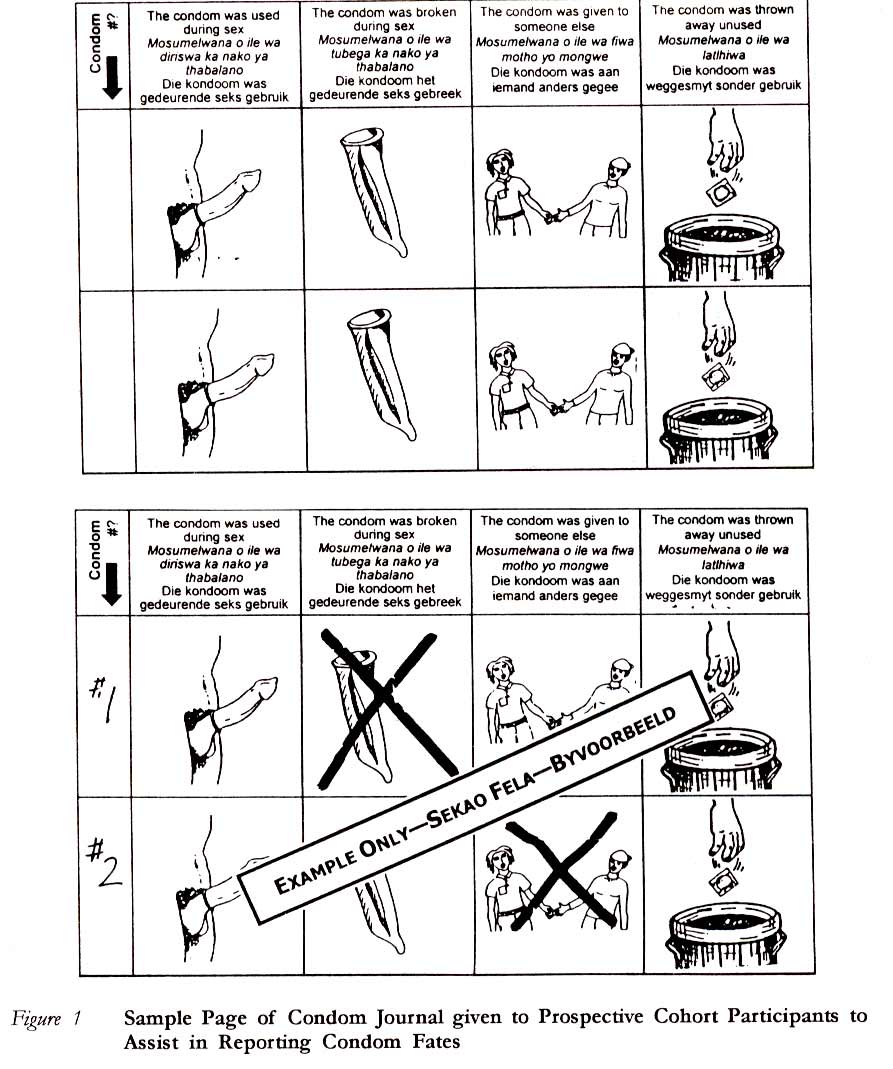
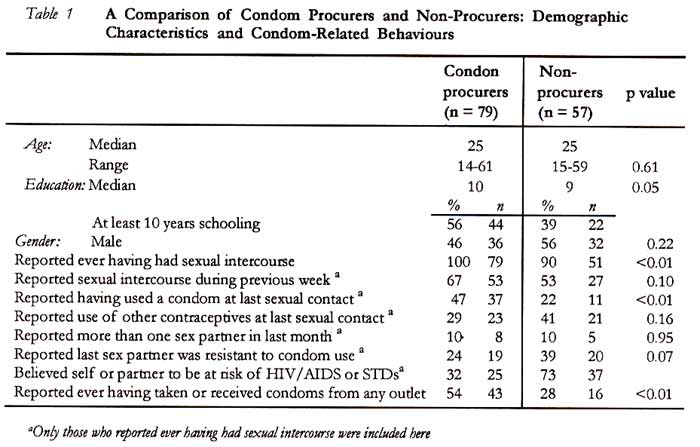
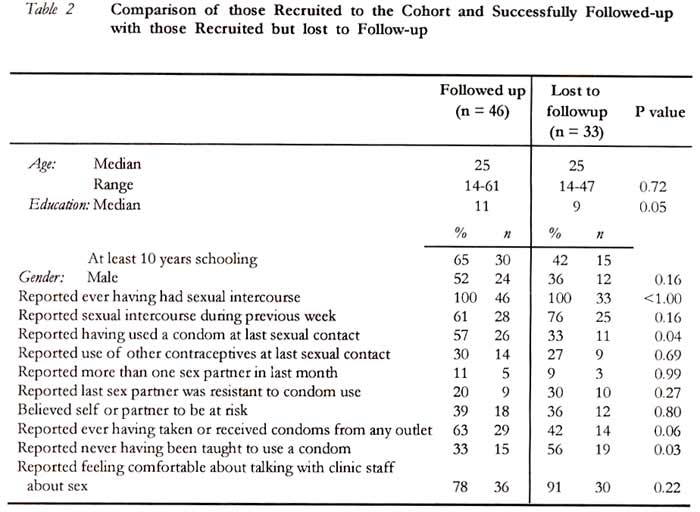
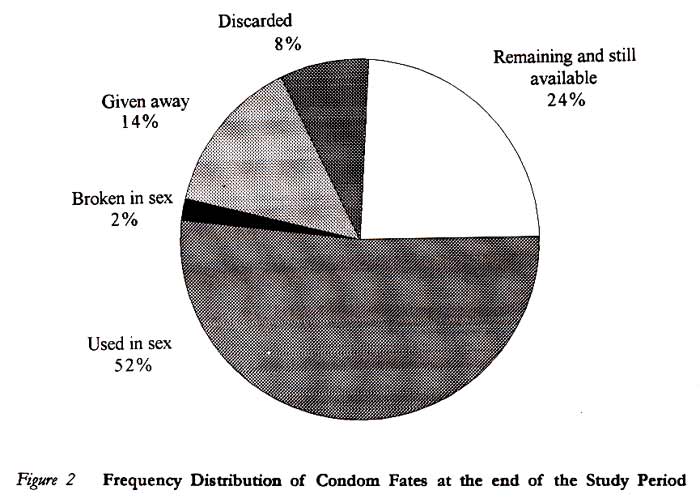
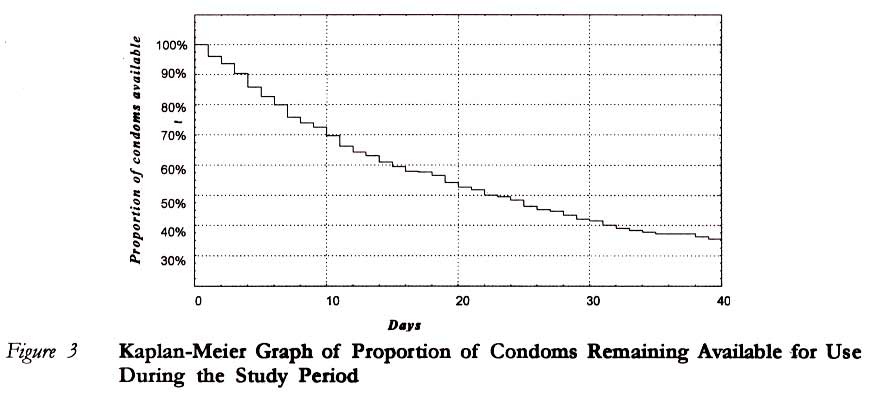
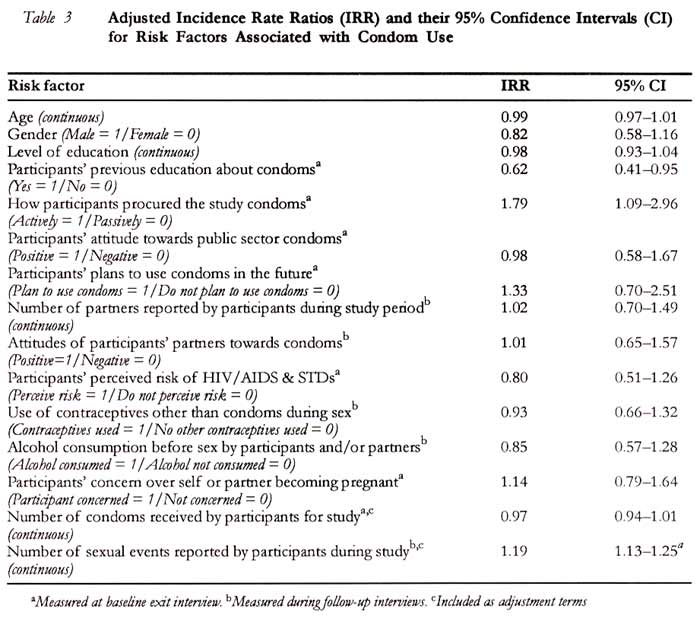
Sciences, University of Cape Town Code Number: rh01008ABSTRACTThere is little understanding of what proportion of condoms distributed to the public in South Africa is ever used in sex and what proportion is wasted. This study presents the methodology and pilot results for research into the fate of condoms as well as factors associated with condom use and wastage. Pilot research was conducted in the Boland/Overberg region of South Africa during June and July 1998. Individuals procuring condoms were recruited into a prospective cohort that participated in follow-up interviews over the following six weeks to report on the fate of the condoms they procured and their sexual behaviour. By the end of the six week study period, 52% of condoms procured from these clinics had been used in sex, 2% were broken in sex, 14% were given away before use, 8% were discarded before use, and 24% went unused. While these pilot results must be viewed tentatively, this pilot study presents an innovative methodology for research into the use and wastage of condoms. (Afr Reprod Health 2001; 5[1]:66 - 74) KEY WORDS: Condom use, sexual behaviour, research methods, South Africa Introduction Male condoms represent the most affordable barrier method available in most sub-Saharan African countries to prevent the spread of HIV/AIDS and other sexually transmitted diseases (STDs).1,2 The distribution of condoms free of charge to the public by government agencies in sub-Saharan Africa has been a central part of national strategies for HIV and STD prevention. In South Africa, the number of condoms distributed by the Department of Health to the public free of charge has increased dramatically in recent years: during 1997, some 172 million condoms were distributed to the general public, compared with only six million in 1994.~ Condoms purchased by the government are distributed through a wide range of outlets, from primary care clinics and government AIDS training, information and counselling centres (ATICCS) to non - governmental organisations (NGOs) and private businesses. Despite these figures and the well - established significance of condoms in combating the spread of HJV/AIDS, there is little understanding of what proportion of the condoms distributed to the public are ever used in sex. The results of cross-sectional studies from South Africa report prevalence of condom ever-use ranging from 220/o in a recent demographic and health survey (DHS)4 to 29% among black adolescents nation-wide,5 but such data provide little insight into the question. Meanwhile, common anecdotes suggest that condom wastage or disuse in various forms may be widespread. The most common approach to studying the proportion of condoms that are actually used in sex is to compare general distribution statistics with cross-sectional survey results of reported condom use. The resulting estimates of the proportion of condoms used in sex range between 10% and 500/0 for developing countries.6-9 Although this approach allows a rough approximation of the percentage of condoms that may be used in sex, it is unable to identify individual characteristics associated with condom use and wastage. Without understanding the profiles of individuals using or wasting condoms, or the contexts that lead to unused condoms, interventions to promote more efficient condom distribution are likely to prove inadequate. This paper presents a new methodology for investigating what happens to condoms once they leave distribution points. The pilot research reported here represents the first part of a national study underway in South Africa to inform more efficient and effective condom distribution strategies. Methods To directly measure condom use and wastage, a more rigorous interdisciplinary methodology was developed for this study. A descriptive cross-sectional study of people leaving condom distribution points with and without condoms was used to understand the local accessibility and availability of condoms. In addition, a prospective cohort study allowed researchers to trace condoms taken by participants for up to six weeks after they left distribution points. During follow-up interviews, cohort members completed fully structured interviews to describe their sexual behaviour and condom use over the study period. Cohort members also participated in unstructured in-depth interviews to explore the attitudes and contextual factors that shape condom procurement, use and/or wastage. These methods were piloted in four municipal clinics serving small rural towns within the Boland/Overberg health region in the Western Cape Province of South Africa. At each of the sites, all consenting individuals taking condoms from the research sites over a two-week period were recruited for an initial exit interview on recent sexual behaviour and condom-related knowledge, attitudes and practices (KAP). In addition, a sample of 58 people not taking condoms was selected and interviewed with a similar instrument (with adjustments in questions specific to condom procurement) as they left the clinic during the same two-week period in which the condom procurers were recruited. After these exit interviews, those individuals procuring condoms were recruited into the prospective cohort. Field researchers numbered each of the condoms procured by participants (using permanent ink on the condom packaging) to facilitate identification and recall. Participants were also given a condom journal for self-recording the fate of individual condoms (Figure 1 shows a sample condom journal). All participants were carefully instructed that their ability to participate in the study was not related to their reported sexual behaviour or their condom use, and that the condoms numbered for tracing in the prospective study should be treated normally Follow-up interviews were conducted at two and six weeks after the initial interview Here participants used calendars and their condom journals to count the number of days between the procurement of condoms (the same day as the initial exit interview) and their eventual ‘fate’. They also reported on their condom and contraceptive use as well as other aspects of their sexual behaviour during the study period. For their participation in each follow up interview participants received an incentive of 30rand (approximately US$5.00) to cover transport costs at the end of each interview. All interviews were conducted by trained field-workers working in participants’ home languages. Researchers explained the purpose and process of each research technique before participants gave their verbal consent. Anaysis Data were analysed using the statistical package Stata (College Station, Texas, USA). Univariate and bivariate analyses were used to describe the condom procuring cohort, the differences between the cohort and those who had not procured condoms, and differences between those successfully followed up for six weeks and those lost to follow-up. Chi-square tests were used to compare proportions, and Kruskall-Wallis tests were used to compare two medians. Kaplan-Meier survival analysis was used to describe the time to condom use. To avoid analytical problems due to the clustering of multiple condoms to one participant, Poisson regression was used to determine the influence of risk factors on the rate of condom use per person. The following risk factors were considered to be of potential importance and were all included in the multivariate model: age, gender, level of education, perceived risk of HIV/AIDS or STDs, use of other contraceptives, and the way in which the condoms were procured. Risk factors were adjusted for the number of condoms taken by each participant and the number of sexual events reported by each participant during the follow-up period. Results Condom Procurement Table 1 describes the 79 people that took condoms from the research sites during the two-week period of participant recruitment, and compares them with the sample 58 people that did not take condoms with respect to demographic characteristics as well as condom-related sexual behaviour. Those that took condoms were more likely to have had more than 10 years of formal schooling (p 0.02) and to report ever having had sexual intercourse (p 0.003). Of those who had ever had sexual intercourse, those taking condoms were more likely to report having had sexual intercourse during the previous week (p 001), and to have used a condom during their last sexual event (p 0.002). Cohort of Condom Procurers The 79 subjects recruited for the follow-up study had procured a total of 934 condoms at the beginning of the six weeks of follow-up. (In addition to these 79 subjects, 13 condom procurers had declined to participate in the research either because they would not be available for the follow-up interviews, or because they did not feel comfortable about the topic of investigation.) The median number of condoms taken was 10, with a maximum of 30. Most of the 79 procurers (63%) had asked health workers for their condoms, while 37% had received them from health workers without asking. (At this clinic, at no time were condoms freely available to the general public without request. Participants receiving condoms without asking were usually either family planning or STD patients.) Attriton Forty-six subjects and their .564 condoms were successfully followed up for six weeks, representing follow up rates of 58% of people and 60% of condoms. Table 2 describes and compares those followed up and those lost to follow-up, with respect to demographic characteristics and condom related behaviour. Those successfully followed up for the six weeks were more likely to have had 10 or more years of schooling (p= 0.04). They were more likely, at the initial exit interview, to have reported using a condom at last sexual intercourse than those lost to follow-up (p =0.04). In addition, more of those followed reported having been taught about condoms previously, compared with those lost to follow-up (p=0.05). Sexual Activity During the six-week study period, the 46 subjects reported having sexual intercourse 379 times, representing a median of nine times per person with a maximum of 28 events. Eleven per cent of participants reported no sexual contact whatsoever and two-thirds of participants reported having sex with only one partner during the study period. A large proportion (79%) of the sexual acts occurring during the study period was done with the use of condoms. It is important to note, however, that 30% of participants reported at least one unprotected sexual act during the six weeks Fate of Condoms By the end of the six-week study, each of the 564 condoms in the study met one of six ‘fates’, illustrated in Figure 2. The Kaplan-Meier survival analysis (Figure 3) illustrates that 30% of the condoms issued and available for use during sexual intercourse were used 10 days after the beginning of the study, and 50% after 22 days. The 92 lost or discarded condoms were excluded from this analysis, as they were not regarded as having been available for use. The consumption of condoms was rapid - almost two-thirds of the condoms were used within one month. Determinants of Condom Use The incidence rate ratios generated by a Poisson regression can be interpreted as the relative likelihood of condom usage during the study period in the different categories of the risk factors (see Table 3). The range of the confidence intervals on either side of 1, the point of equivalence, indicates the direction and strength of the relative likelihood of condom usage. The table shows that those actively procuring condoms (either by requesting them or taking them without asking) were more likely to use the condoms than those who received their condoms passively from health care personnel were. In addition, individuals who had received formal health education about condom use were less likely to use their condoms than those who had no such education were. Discussion Given that this data comes from a pilot study, and that these results are based only on the 46 individuals who were successfully followed up, the results are tentative. It is possible that some of the associations detected are spurious, or that we did not have the power to detect the factors that are associated with condom usage. Risk factor analysis will be further explored once the results from the national study become available. Although this analysis is still exploratory, it has generated some interesting results. The condoms are used quite rapidly, and the overall rate of actual condom use is high while wastage is somewhat lower than we had anticipated. In the light of this, it is important to note that the individuals taking condoms from these sites are not typical of the general population. Rather, these condom procurers represent a select group, who are more sexually active, more likely to report having used a condom at last sexual intercourse before the study and more aware of condoms than those lost to follow-up as well as their non-condom procuring counterparts. Each of the four clinics gives out, at most, 500 - 1000 condoms in a month, a low figure by national standards. This statistic says as much about the local approaches to condom distribution as it does about community attitudes. In in-depth interviews, all of the health care providers at the clinics in question noted that they ‘knew’ the people taking condoms and knew that they would use them; in these instances, condom use was wholeheartedly promoted. At the same time, the providers said that they also ‘knew’ who would waste condoms - from adolescents in search of inflatable toys to overly optimistic older men - and such individuals were actively discouraged from taking condoms. When a new face requested condoms they were asked explicitly what they would do with them and with whom. One good example of this was from an interview with a fourteen-year old boy, who asked for condoms and was promptly told that he must first produce a girlfriend with whom to use them. These kinds of condom distribution practices are nothing new in South Africa,10 but in the case of the pilot sites they could have had significant consequences on the observed rates of condom use. Providers who exercise conservative practices with respect to condom distribution coincidentally help to screen possible condom wasters. These practices may, in turn, lead to condom distribution limited largely to regular condom users, and thus the observed high condom use rate among this cohort. ConclusionsLessons from Pilot Study Several lessons from this pilot study will be addressed by refinements in the research methodology before the research is expanded to other condom distribution sites across South Africa. By raising topics such as condom use and HIV/AI[DS and STDs the study has the potential to change the behaviour, or at least the reported behaviour, of participants. As a result, it is possible that participants in follow-up interviews may have had the tendency to overestimate their reported condom use or that the study may have actually changed behaviours and increased condom use. This effect is common to almost all studies of condom use and sexual behaviour. In this study, this effect can be measured by crosschecking data on condom fates with data from sexual behaviour, and possibly using the condom journals to verify interview data.” In addition, the response rate of participants recruited for the cohort study was lower than we expected and this loss of condom procurers to follow-up represents a source of potential bias. These results show that those followed up were more likely to be men, were better educated, and were more likely to have used condoms previously, than those lost to follow-up. Tracing cohort members can be unusually difficult in this setting, as most participants do not have telephones at home, and many live in informal settlements without a simple home address. Nonetheless, it may be possible to improve the follow-up rate by reducing the time between follow-up interviews and by extending the availability of field researchers to meet participants. Relevance to Policy Making In the case of the pilot clinics, it seems clear that making providers aware of the issues of condom accessibility at clinics as well as their important role in facilitating the efficient use of condoms is crucial. On a national level, given the diversity and complexity of local condom distribution in South Africa, there is obviously no single panacea for improving rates of condom consumption. Rather, this research is important in understanding the kinds of behaviours and interactions that can lead either to condom use or wastage. This in turn is vital in developing models for more efficient and effective condom distribution, models that can be used to design local solutions. Finally, this type of research can provide more accurate estimates of the effectiveness of condom promotion policies in the prevention of NIIV. Acknowledgements This study was funded by the South African Department of Health’s HIV/AIDS and STD Research Funding Committee, with support from the Medical Research Council (MRC). Ethical approval was granted by the Research Ethics Committee of the Health Sciences Faculty at the University of Cape Town. The authors would like to thank Alana de Kock, Mango Matha, Eldred Fourie and Nokuzola Matiso for their outstanding field research. In addition, the assistance of Carl Lombard in designing and analysing the study, and the comments of Merrick Zwarenstein on the report, were greatly appreciated. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01008t1.jpg] [rh01008f2.jpg] [rh01008f1.jpg] [rh01008t2.jpg] [rh01008f3.jpg] [rh01008t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}