 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
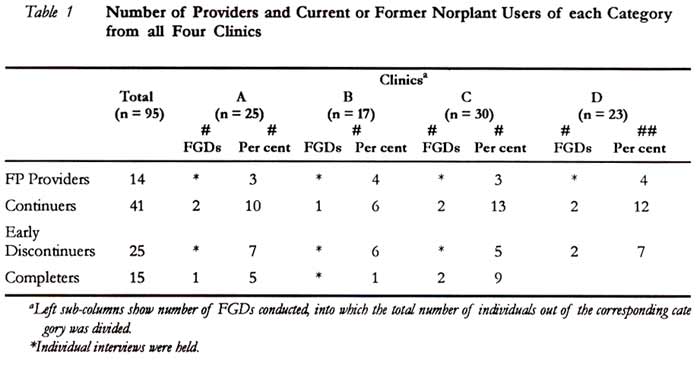
African Journal of Reproductive Health, Vol. 5, No. 1, August, 2001 pp. 90-99 Access to Norplant Removal: An Issue of Informed Choice Elizabeth Tolley1 and Christine Nare2 1Family Health International, Research Triangle Park, NC, USA. 2Comité d’Etudes sur les Femmes, la Famille et l’Environnement en Afrique (CEFFEVA), Dakar, Fann, Senegal. Correspondence: Elizabeth Tolley, FHI P.O. Box 13950, Research Triangle Park, NC 27709. Fox: 919/544-7261 Email: btolley@fhi.org Code Number: rh01011ABSTRACTThis paper presents data from a qualitative study to examine women’s experiences in using and discontinuing use of Norplant at four family planning clinics in Dakar, Senegal. Focus group discussions and individual interviews were conducted between June and August 1996, with 81 current and past Norplant users and 14 providers. The study found that a woman’s desire to limit future childbearing and her husband’s support for method use increased her acceptance of side effects and use of the method. Counselling that women perceived to be thorough and that included discussion of other options also had a positive effect on acceptance and use. Finally, the study identified ways in which providers attempted to control decision-making about treatment and discontinuation in all four clinics. Such attempts had a negative impact on women’s experiences using the method. Findings from the study suggest the need for a more client-centered approach to Norplant service delivery, one that emphasises consideration of individual circumstances during counselling and that ensures client control over decisions about continued use of the method. (Afr J Reprod Health 2001; 5[1]:90-99) KEY WORDS: Norplant informed choice; removal, qualitative research Introduction The concept of informed choice in contraceptive decision-making maintains that individuals or couples have effective access to a range of contraceptive options, adequate information about these options, and the ability to actively participate in decisions about their use.1,2 For potential Norplant users, this suggests they be well informed about insertion and removal procedures, about method-related menstrual and other side effects, and about other available contraceptive methods. It also suggests that women who elect to use Norplant retain ultimate control over how long to use it and when to have it removed. Nevertheless, acceptability studies in Bangladesh, Indonesia, Thailand, Egypt and the Dominican Republic identified limitations to women’s informed choice of Norplant. Among the problems identified, some women faced significant barriers to early removal of their implants3,4,5 With that in mind, a study was conducted in Dakar, Senegal, in 1996, to evaluate access to early removal of Norplant. Senegal was the first African country to introduce Norplant, conducting a preintroductory trial in one clinic in 1986. By 1992 the method was available through five clinics in Dakar and by the time of this study, approximately 3,000 women had used the method. Although two earlier acceptability studies suggested that women were not always informed about when they could have their implants removed, no African studies has examined women’s experiences obtaining removal.14,15 The study reported herein determined the following a. How women cope with side effects b. Why women request early removal of their implants c. How service providers respond to these requests for removal The WHO and others have called for a new approach to family planning programs, one that puts people before technology. As Simmons and Fajans point out, increasing the number of contraceptive options available does not necessarily expand individuals’ reproductive choice. In order to do so, the new method must correspond with potential and actual contraceptive users’ needs as they themselves perceive them, and it must be provided in a way that preserves or enhances quality of care for all methods, not just the one being introduced.6,7 In a more client-centered program, providers’ technical knowledge and expertise is tempered by individual clients’ awareness of their own life situation, their personal preferences for specific contraceptive attributes and their concerns about real or imagined side effects. In this context, the client’s role in contraceptive decision-making is paramount.5 The WHO call for a new strategy was in part based on experiences with Norplant introduction.6,7 When Norplant came into the market, it promised to greatly expand women’s reproductive choices by providing a non-vaginal contraceptive method that was safe, effective, and could be used long-term. Norplant’s high continuation rates have been considered as one indication of the method’s acceptability to women around the world. First year continuation rates are around 80% in a number of countries. 9,11-13 However, in many studies the five-year continuation rates are lower, somewhere between forty and seventy per cent.9,10,12 Norplant acceptability studies identified two factors: women’s desire to become pregnant; and their intolerance of side effects, especially menstrual disturbances, as the most important reasons for discontinuation before five years of use.10-13 While reasons for discontinuation are known, few studies have examined women’s experiences obtaining early removal of their implants. Nevertheless, these few suggested that some Norplant users faced significant barriers to early removal. A study of access to removal services in Bangladesh found that some providers discouraged clients from early discontinuation out of concern for the method’s relatively high cost. They encouraged clients to follow treatment or wait for side effects to subside, performing removal only after these two approaches failed.3 A four-country study on Norplant acceptability using focus group methodology also indicated that some users perceived problems with access to removal. To overcome these difficulties, women resorted to giving false reasons for requesting early removal.4 A qualitative study in the US looked at the perceptions of Norplant users who discontinued the method early. Women in this study suggested that they accepted Norplant under false pretenses. Some felt pressured to accept the method and did not feel they had been fully counseled about side effects. Others were initially denied removal when they requested it. Women who experienced these problems said it engendered a lack of trust in the medical community that they did not have previously.5 Methodology Qualitative data were collected between July and September 1996 at four clinics in Dakar. Three of the four clinics are in the public sector, while the fourth, an International Planned Parenthood Federation (IPPF) affiliate, is a non-governmental organisation (NGO). One of the public-sector clinics, a teaching hospital, had been providing Norplant through a preintroductory trial since 1985. The NGO had limited services available in 1991. The method was not offered in the other two public clinics until 1992. Three different types of Norplant users participated in focus group discussions (FGDs) or individual interviews. "Continuers" (women who were using Norplant) took part in FGDs at all four clinics. FGDs or individual interviews were conducted with "completers" (women who used the method for at least four and a half years before stopping) in clinics where Norplant had been available for this long. Women who had their implants removed at or before three and a half years of use, referred to as "early discontinuers"a, were interviewed individually in all but one clinic. Discussions with all groups focused on women’s experiences with side effects, including any requests for early removal of their implants and their experiences requesting removal. Early discontinuers were asked about their reasons for removal, and the process of obtaining it. In addition, Norplant providers were interviewed individually to identify any provider-based barriers to removal before five years of use. To avoid selection bias, researchers made lists of all women who fit the study’s description of continuer, early discontinuer and completer from each of the four clinic’s registers since 1990. At each clinic, forty women were randomly selected from each of the continuer, early discontinuer and completer lists. A community worker attempted to visit each of these women in their homes, inviting them to participate in a focus group discussion. Those who agreed to participate received a second visit to communicate the time and place of the discussion. To ensure a neutral setting, a room was rented in a well-know social centre located on a main public transport line and near a large market area. Because so few early discontinuers who agreed to participate actually showed up for the first scheduled FGDs, researchers decided to interview the remaining women individually in their homes. Providers were interviewed at the clinic. Providers were purposefully selected so that at least one provider interviewed at each clinic had been formally trained in Norplant provision and all interviewed were able to insert and remove the implants without supervision. All in-depth interviews and FGDs were recorded on cassette, translated into French and transcribed and typed into separate word processing files. Transcripts were coded and a software package was used to categorise data into approximately 25 broad topical areas ranging from "women’s histories of contraceptive use" to "obstacles to early removal". Researchers analysed each topical area for ideas, concepts or experiences that were common across clinics and client and provider groups, and those that differed from one group to another, or within groups. FindingsA total of 81 current or former Norplant users and 14 providers participated in the study. Table 1 shows the number of women and providers who participated from each category and clinic. The left column under each clinic shows the number of FGDs conducted, into which the total number of individuals was divided. When there is no number in the left column, individual interviews were held. Individua1 Awareness and the Choice of Norplant Women’s motivations for using Norplant About one-third of women in this study clearly stated that they did not wish to have any more children. Several of these women had important medical reasons to limit births. More often, women wanted to avoid pregnancy because they simply had too many children, too few resources and were too tired to cope. At least a dozen women with too many children, or children too closely spaced, attributed the problem to unwanted pregnancy and contraceptive failure. Most had gotten pregnant while using the pill. They were particularly attracted to Norplant’s long period of effectiveness and its ease of use and determined to put up with side effects. One 31-year-old woman that already had four children used the method for five years, despite intervals of amenorrhea, heavy bleeding and excessive weight gain. "...even if someone suggested that I come into an alley, and (get) cut a little with a knife in order not to have children, I would have preferred that to (hearing) Madam, push’ !" Most women, however, wanted at least one more child. They were using Norplant to "rest a little" before getting pregnant again. These women tended to be younger, with three children or fewer. About half a dozen women were not married. Whether single or divorced, almost all said they had intended at the time of acceptance to use the method for at least five years. As they began to experience side effects, however, a number of these women changed their minds about how long they would continue Norplant. The words of one woman convey her wavering "It’s true that I was hoping to remove (Norplant) beause of my health. And also, and especially, I wanted a daughter. I on/y have sons. Then my (blood) pressure was too low something that had never happened to me before. I was afraid and I had to give it up. But my wish is to have a girl." Partner’s role in contraceptive use Men clearly had a powerful influence on women’s Norplant experience. Most women actively engaged their partner in the decision to use Norplant. When wives consulted husbands, and couples agreed on their family planning goals, Norplant users appeared better able to tolerate side effects. For example, a 39-year-old woman who had already used the method for approximately three years said: "My husband himself suggested that I take Norplant to space births, because for him, with these close/y-set baptisms, we couldn’t accomplish anything.... When I talked to him about Norplant, he felt that this could do it- especially since it lasted for five years. When I have a long period, I avoid my husband during this time. Either I go to bed very early or I stay outside chatting until I am sure that he is sleeping. But everything is going well. There isn’t a problem." On the other hand, about one third of women reported that their husbands did not approve of Norplant use. The objections were numerous. Some men valued large families, or simply considered contraceptive use to be against religion. Others appeared to construe their wife’s act as a threat to their authority. A few women said their husbands worried that side effects might endanger their wives’ health. Some women actively disregarded their husband’s attitudes. Others obtained the method without informing him. But the immediate signs of the insertion procedure, and longer term changes in menstrual patterns or other side, effects, make it difficult to hide Norplant use. Such women often faced strong opposition to their continued use of Norplant. In the words of one current user: "He doesn’t want me to plan (my pregnancies), because for him, if I do, it’s because I’m going to prostitute myself. He is very jealous.... When I had the insertion, my husband didn’t know. So, when he learned about it, he created a lot of problems. He saw the bandage and asked me what I had done. I told him that I had gotten Norplant. I didn’t hide it from him.... He created a lot of problems for them (at the clinic), telling them that (s)he didn’t have the right to do my insertion without his agreement. The midwife told him that I was the one who had told them that he had agreed; and that was the truth - that’s what I told them. I told them that I needed it (Norplant)." Technical information about method choices Most providers insisted that they gave women a full range of contraceptive choices and the information needed to use the methods well. However, women’s perspectives on counselling varied substantially from clinic to clinic. Based on client accounts, only two of the four study clinics appeared to counsel women thoroughly about method options and only one did so consistently. In that clinic, some participants from all FGDs and six out of seven early discontinuers stated that they were shown all the contraceptive methods available at the clinic. Most added that the provider told them about advantages and disadvantages of the methods. In addition, almost all clients said providers explained the different side effects associated with Norplant. One client explained her counselling session this way: "They explained the side effects to me that are linked to Norplant. They told me that I could have headaches all the time or I could go a long time without my period or I could have it three times in one month. Then, they told me not to worry if one of these things happened, since it's linked to Norplant and people react differently to Norplant. Really, they were clear with me. And I accepted all of it...I told myself ,.. I am choosing Norplant as an informed woman and I agree to deal with all the side effects. On the other hand, if they hadn’t told me about these side effects and then I suffered from them, I would immediately see them to talk about what was happening to me." When sufficiently counseled, clients who experienced bleeding side effects did not appear very concerned. They recognised that their irregular cycles were due to Norplant. Some did not bother to return to the clinic. Others were provided additional counselling, or treated occasionally with pills to which they responded well. In contrast, counselling appeared inadequate for numerous clients in the other clinics. Clients who were in fact told about "some", "several", or"other" ; contraceptive methods before obtaining Norplant rarely mentioned being told about their advantages, side effects or contraindications. In addition, counselling on Norplant side effects was minimal. Most women who said they were counseled about side effects were told only about possible bleeding disturbances. Fewer were told about headaches, dizziness, weight gain or other side effects from Norplant use. Consequently, when these problems did occur users were concerned or even frightened. And, while some clients said they were counseled about the benefits and disadvantages of the method, they concluded that the information given had been misleading. For instance, a 39-year-old Norplant user explained: "Before the insertion, the midwife warned me about the little problems that I might encounter with Norplant. She said that I could have amenorrhea for a certain amount of time, then one fine day have my period in a normal cycle. But I realise that the bleeding problems, the menstrual disruptions that I would be forced to live with had been minimised." Four out of six early discontinuers from one of the three clinics said they were not counseled about Norplant’s side effects at all. One of the women was surprised that she had not seen her menses for some time. She only learned that it was a side effect of the method when she returned to the hospital. A second woman suffered from bleeding and abdominal pain. She gave the following account "I didn’t talk with anyone. They say that normally when a woman arrives at the family planning service, someone must talk with her and tell her how Norplant works. But me, on!y my friend gave me information... every time that I went to the centre to talk with them, I was always told; ‘You were told about all of that before insertion’. But in truth, their problem is that they don’t tell you clearly what there is about Norplant." Several clients said they were only counseled about Norplant’s side effects on the table just before or after the implants had been inserted. A 35-year-old woman who used the method for only six or seven months pointed out "I no longer had a choice. I accepted." Role in contraceptive decisions Women must rely on providers both to initiate and discontinue Norplant use. Because of this, providers can wield tremendous control over such decisions if they choose to do so. In this study, providers sometimes attempted to influence women’s decisions about Norplant use by withholding information or delaying removal. Information about ear/y removal of Norplant Information about early removal of Norplant varied widely among clinics, as well as among individual providers. And, the information that providers said they gave differed from what clients said they were told. The way clients interpreted these sometimes confusing messages about access to removal affected their willingness to tolerate side effects and ultimately affected their satisfaction with the method. All providers recognised in theory a client’s right to remove her implants whenever she wanted. However, less than one third of providers said they told clients that early removal was possible "at any time". Just less than one quarter of them told women they could only remove their implants after five years. Slightly more suggested early removal might be possible, but only for reasons that they (the providers) considered acceptable. Most often, valid reasons for early Norplant removal included severe or persistent side effects such as migraines, heavy bleeding that did not respond to treatment, increased blood pressure, and weight gain. A few providers said a woman’s desire to get pregnant again, or a husband’s request was also sufficient for obtaining early removal. Clients were even less likely to say they were told that removal was possible on request. Only three of 25 early discontinuers and women in two of 12 FGDs said they were given this information. During initial visits, many Norplant acceptors said they were told that removal was only possible after five years of use. A woman who obtained her implants just months before this study was conducted said "They tell you something that is certain - it (Norplant) is not removed before five years. (Providers say) there are people who come before five years and agitate us to remove them. They cause us enormous problems." Some women were not told anything about removal during initial visits. They learned about removal possibilities later by asking clinic personnel during follow-up visits or overhearing neighbours, friends or other clients talk about their experiences. The information that women gather from these different sources is often conflicting. They are left to sift through the various accounts and determine what, if any, action they can take. Women’s experiences obtaining early removal of Norplant Regardless of what they were told (or not) during early counselling sessions, some women attempted to have their implants removed before five years of use. But while some obtained early removal with relative ease, others obtained it with much difficulty, or not at all. Table 2 summarises early discontinuers’ experiences of removal. Easy removal About half of the early discontinuers said they had little problem obtaining removal of their implants. Six of the ten stopped using Norplant because of side effects.b However, in five cases it was the provider, and not the user, who suggested that the implants be removed. Removal was suggested not because of spotting or prolonged bleeding, but because of other side effects such as high blood pressure or excessive weight gain. Providers believed that these problems increased the risk to the client’s health or decreased the method’s effectiveness. The only woman who sought and easily obtained removal herself because of bleeding was in the medical corps and a colleague of those from whom she requested Norplant services. The other four early discontinuers in this group stopped using Norplant to get pregnant. All but one of these women had used the method for three years before stopping, and had been assured prior to insertion that they would be able to do so. In general, women who were able to get their implants removed when they wanted were satisfied with the method, despite the side effects they may have experienced. For example, one woman in this group exclaimed: "As for me, I don’t have the right to say anything bad about Norplant. I didn’t have any problem with it. When I wanted to use it, they inserted it with no problem, when I wanted removal I didn’t run into any difficulties."Removal with difficulty Nevertheless, as shown in Table 2, an equal number of early discontinuers reported difficulty in obtaining removal. Most of these women initiated the removal request themselves because of bleeding disturbances. Providers, however, appeared less willing to grant immediate removal under these circumstances. Some providers explained that it was their duty to treat side effects, particularly bleeding, before allowing removal. Such a policy had physical, emotional and financial repercussions on women’s lives. Despite providers’ assertions that treatment is voluntary, women commonly complained that they were forced to return to the clinic many times for counselling and treatment before they were granted removal. A phrase used by women from three out of four clinics was "coming and going". Fed up with the process, one woman stated: "I went to see the midwife several times because of bleeding problems in order that she do the removal. But each time she told me to leave it like that, that the bleeding was going to stop. It is especially this last time when I insisted that she give me a tubal ligation that she discussed (things) serious/y with me." For more than a dozen women in this study, the actual treatment of their side effects was as difficult to support as the side effects themselves. Some complained that the pills they were prescribed did not help stabilise their periods. At least five women complained of suffering pill-induced side effects in addition to their original problems. Three of these women had used oral contraceptives prior to accepting Norplant, and changed methods to avoid these side effects. A current Norplant user pointed out the contradiction: "It’s the prolonged bleeding that discourages me the most. Once the period begins it’s ‘non-stop’. As long as I don’t take pills the bleeding doesn’t stop, so much so that I have the impression that I’m ‘on pills’. I used to have some problems with the pills; that’s why I wanted to change. If I am going to have to start taking the pill again despite the fact that I am on Norplant, frankly it’s no longer very interesting. Four times I had bleeding that lasted at least 15 days each time, and each time I had to take the pill to stop the bleeding. During these times I am not (sexually) available to my husband. In addition, the pills that I was taking gave me nausea, dizziness; I had the feeling that I was pregnant. It really bothered me!" In a few cases, Norplant users found the cost of treatment prohibitive. Having used the method for just over one year, one woman estimated that she had spent as much as 30,000 CFA (or $60) on prescriptions and laboratory tests before removing the implants. The above study participants eventually succeeded in having their implants removed. However, one or more continuers from all four clinics said they had been denied removal at least once during their use of Norplant. Likewise, some women in all completer focus groups and in three individual interviews said they had been denied removal in the past. Even some women who used the method for five years but did not wish to renew it had to request for removal several times before being granted it. One woman who had used the method for five years said: "They made me run! They were always giving me appointments and when I would come, they would send me away until another date, because they asked me if I really wanted to have it removed and I answered that I had decided to remove it. The last time she knew I really wasn’t joking. I had really decided and then she told me ‘Since you’ve really decided, stay, we’ll remove it for you.’ When they did the removal at the last minute, they asked me if I wanted to do a removal and reinsertion. I answered that I would wait and see." Discussion Acceptability studies often suggest that side effects are the critical factors in determining continuity or discontinuation of methods. This study demonstrates, however, that other more fundamental factors influence how women interpret these physical manifestations. Women’s attitudes towards side effects were strongly affected by the kinds of information they were provided with, the role they played in decisions about use, and ultimately how well the method suited their individual reproductive needs and life circumstances. Little can be done in the short term to change the attitudes of partners and other family members towards family planning. However, we can improve the chances of individuals or couples for obtaining the best method for their personal situations by ensuring that family planning services are provided in a context of informed choice. The results of this study indicate that contraceptive clients and providers alike will benefit. The following discussion suggests areas in which the context of informed choice is critical. Women appreciate providers’ efforts to fully counsel them about all family planning methods, and especially about the full range of side effects associated with Norplant use. Those who had been counseled about the full range of Norplant’s side effects appeared better able to tolerate these side effects, and to seek treatment for them. In contrast, women who were not well counseled about side effects were often surprised and even frightened by their occurrence. They concluded that providers had tried to minimise side effects in order to convince them to use the method, producing a lack of trust in clinic personnel. It is particularly important for women who plan to use the method without their partner’s knowledge, or in defiance of his wishes, to consider the kind of bleeding side effects that are likely with Norplant, and how they will manage these side effects in the light of family opposition. The counselor should also review a woman’s reproductive intentions with her before accepting Norplant. Women who would like to get pregnant again within one year or two could then be encouraged to use a method that can be more easily discontinued. It is possible that some women may choose not to use the method after such counselling However, those who do select Norplant after such counselling should be more satisfied and more likely to continue. Providers send mixed messages about access to early removal of the implants. While most midwives recognised a woman’s right to have the implants removed whenever she desired and for any reason, few had provided this information to clients. Yet, as pointed out in this and other studies, women gain information about Norplant from a wide variety of sources.7,9 As women compare what providers tell them about early removal with the experiences of other Norplant users, the disparities become apparent. Such disparities are likely to heighten women’s concerns about the method, without substantially reducing and perhaps increasing requests for removal. Many women who requested removal because of side effects experienced considerable difficulties stopping Norplant use early. Providers’ unstated policy to exhaust available treatments for bleeding before allowing removal is undoubtedly well meaning. They would like to help women continue the method if a solution was available. Some women readily accepted such medical treatment. They were content to follow the treatment even when it meant doing so on a regular basis, because it allowed them to continue using Norplant. Others, however, were not at all content to try any medication to end the bleeding. Their objections were varied. Some experienced treatment-induced side effects. Some women disliked the financial burdens or disruption to their schedules that such treatment involved. Others simply objected to such treatments being forced upon them when they had decided to stop the method. While providers need to present all the options available to clients in managing Norplant side effects, the choice to treat or remove should remain with the method user. Such a policy would benefit not only the client, but also clinic providers. Repeated clinic visits pose financial and other burdens on Norplant clients who have already decided they would like to stop using the method, and further heighten their dissatisfaction. Additionally, the more women queue up in busy family planning clinics to complain about and receive treatment for unexpected side effects, the less time clinic staff have available to provide thorough counselling to new method acceptors. The words of one long-term Norplant client provide a fitting conclusion for this study: "Talk better with people inform them well. The midwives who give it (Norplant) should organize a day to better explain, not to hide, the advantages and disadantages that there are, because every medication has advantages and disadvantages. Now, everyone must take responsibility for using it or not. I think that if it (Norplant) was provided like that, many people would have the courage to use it." Acknowledgements This is a shortened and updated version of a report entitled "Women’s Experiences with Norplant Removal in Four Clinics in Dakar". The report was presented at a sub-regional conference on Norplant held in Lomé, Togo, in April 1998. Family Health International (FHI) provided support for this study with funds from USAID, although the views expressed in this article do not necessarily reflect those of FHI or USAID. The authors would like to thank Ms. Lucie Noellie Tapsoba, Daba Nguer, Rosalie Ndeye Lô, Jacqueline Cabral, and Halimatou Ba for their diligent work in conducting interviews and transcribing tapes. Finally, I would like to thank Dr Barbara Janowitz for her technical guidance in developing the study and thoughtful review of the final report from which this paper was written. NOTESa. The term "early discontinuation" has been used in this paper to mean discontinuation before three and a half years of use. The phrase is problematic in the sense that there is, and should be, no minimum length of use associated with this method, and, therefore, there should be no negative connotations with discontinuation before five years. Nevertheless, the author feels that in many settings providers and clients alike believe Norplant should be used at least two or more years before removal. The use of "early discontinuation" has been retained in this paper because it conveys the feeling of disapproval that women must face, who act to discontinue Norplant before a generally acceptable period of use. b. All but six women in this study experienced at least one side effect they attributed to Norplant use. Menstrual disturbances, and especially prolonged or frequent bleeding and amenorrhea were reported most frequently. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01011t1.jpg] [rh01011t2.jpg] |
| |||||||||

{kind=link}
{kind=link}