 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 5, No. 1, August, 2001 pp. 100-105 LABORATORY REPORTS Sonographic Assessment of Fallopian Tube Patency in the Investigation of Female Infertility in Ilorin, Nigeria Oguntoyinbo AE1, Amok AOD1 and Komolafe OF1 1Department of Radiodiagnosis, Faculty of Health Sciences, University of Ilorin, P.M.B. 1515, Ilorin, Kwara State. Correspondence: Dr. A.E. Oguntoyinbo, Department of Radiodiagnosis, Faculty of Health Sciences, University of Ilorin, P.M.B. 1515, Ilorin, Kwara State. E-mail: fhsilorin@ampa.net.ng Code Number: rh01012 ABSTRACT This study was conducted to bring into focus the value of pelvic sonograms in assessing tubal patency in order to overcome the radiation hazard associated with hysterosalpingogram (HSG), reduce cost of examination and encourage it as first-line office-based procedure for management of female infertility. Fifty consecutive female patients primarily designated for HSG underwent pre- and post-HSG pelvic sonograms and the results were documented. Agreement between HSG and SHSG was established in 89 of 100 (89%) fallopian tubes. The sensitivity of sonohysterosalpingography (SHSG) in diagnosing tubal patency was 85.5% and the specificity 96.8%. Analysis of the raw data gave positive predictive value of 98.3% and negative predictive value of 75%. It is accepted that there is no statistically significant difference (p = 0.237) between the results of the two methods (HSG and SHSG). SHSG is found to be a reliable, relatively inexpensive diagnostic and therapeutic (guided hydrotubation) procedure in the management of female infertility (Afr J Reprod Health 2001; 5[1]:100-105) KEY WORDS: Sonography, fallopian tube, investigation, management, infertility IntroductionIn this study, we have attempted to demonstrate or highlight the value of pelvic ultrasonography in the management of female infertility, which is a very common clinical and very emotional problem, particularly in Africa. Prior to this study, there have been standard methods of determining tubal patency. These include hysterosalpingography, tubal insufflations, and laparoscopy and dye test, the commonest being HSG. Hysterosalpingography is a fluoroscopic procedure that outlines the uterine cavity and fallopian tubes. It is used most often in the investigation of infertility.1 In evaluating the efficacy of pelvic ultrasonography in the detection of tubal patency, HSG was used as the gold standard for the diagnosis. Hysterosalpingography is however associated with some disadvantages, which include patient discomfort, radiation exposure to patient and personnel, high cost, and scarcity of resources in a developing country. This study was thus carried out with the following objectives in mind:
Materials and Method Fifty consecutive patients with either primary or secondary infertility were examined at the Department of Radiology, University of Ilorin Teaching Hospital, Ilorin, between February and August 1997. These patients were primarily seen for HSG evaluation of utero-tubal status. However, we painstakingly explained the rationale for the study and obtained their verbal consent. In carrying out this study, two methods of assessing tubal patency were employed:
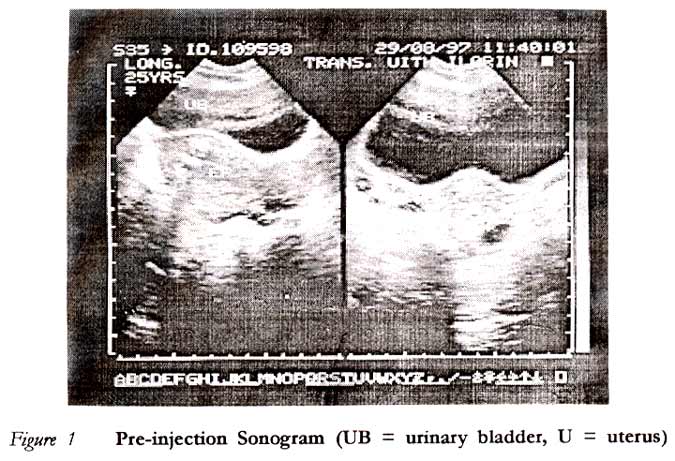
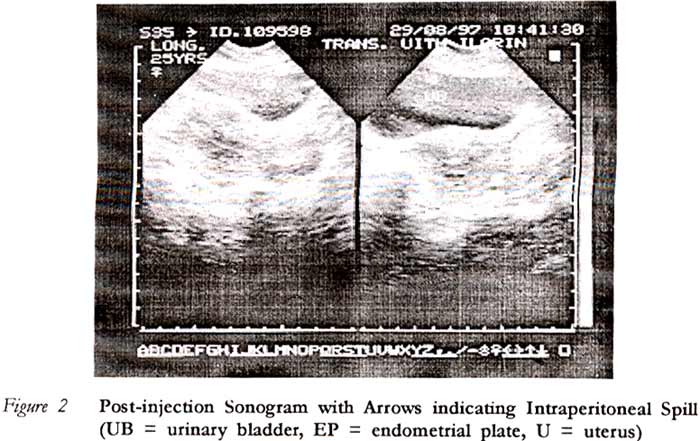
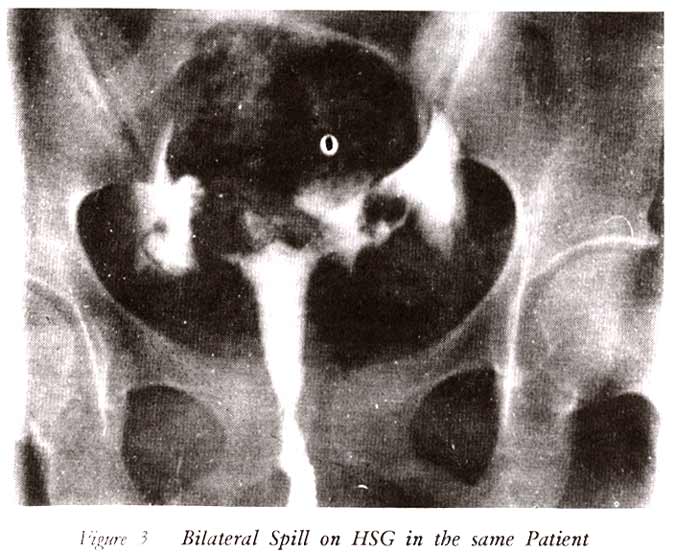
This second method utilised the injected iodine-containing contrast medium, thus eliminating the need for introducing sterile isotonic saline into the reproductive tract and a separate appointment as in the first procedure. However, since one of the aims of this study was to reduce cost, the first method was advocated or favoured in practice. Nevertheless, it was decided for the purpose of this study to use the second method because it eliminated the need for two separate examinations at different sessions; the first being direct sonohysterosalpingogram and the second, X-ray hysterosalpingogram. All pelvic sonograms were done with Siemens Sonoline Sx machine, a scanner with a 5-MHz mechanical sector transducer, while the HSG examinations were done using GEC medical unit with an Apollo Dynamax HD 50D tube head. The contrast medium used was urograffin 76% (Scherring Federal Republic of Germany). After ensuring proper booking of patients, and following the ten-day rule, each patient had a pelvic scan (pre-HSG scan) with a full bladder. After completely emptying the bladder, HSG was then carried out by an independent radiologist. Each patient had intravenous administration of 20mg hyoscine butylbromide as pre-medication. The outcome of the HSG was unknown to the investigators until after the final pelvic scan (post HSG scan), immediately following the second radiographic exposure, prior to the delayed exposure. However, in practice we have observed that by the time the post-HSG scanning was done, the bladder was sufficiently refilled, probably from the initial fluid administration to the patient to obtain a full bladder prior to the initial scanning. Based on these three sequential steps (pre-HSG scan, HSG examination and post-HSG scan) and the findings, the following sonographic features were regarded as evidence of tubal patency: Presence of free fluid in: a. either of the adnexae, indicating patency of the ipsilateral fallopian tube; b. both adnexae and around the pelvic parts of bowel loops; c. pouch of Douglas alone; and d. in all of the above sites. All HSG examinations were interpreted by direct visualisation of hard copy images, checking for unilateral or bilateral peritoneal spillage of contrast medium. Results and Data Analysis The fallopian tubes were evaluated separately and the results were compared with the findings at HSG. Two of 50 patients (4%) had fluid collection on pre-HSG scanning. In one patient it was periadnexal and was attributed to an old pelvic inflammatory disease. The other showed a small amount of free fluid in the pouch of Douglas that was considered physiological, presumably from a ruptured follicular cyst, as she was examined on the 16th day of the menstrual cycle. In these two patients, additional fluid different from the collection or an increase in the amount of the pre-existing fluid was considered as evidence of tubal patency In all, 100 fallopian tubes were examined, as none of the patients had a history of previous salpingectomy. Patency of the fallopian tube was established by SHSG in 60 of 100 (60%) tubes examined while HSG showed 69 of 100 (69%) tubes as patent. When the results of SHSG were compared with those of HSG, there was a 90% agreement on the right and 88% on the left (mean concordance 89%). The overall sensitivity of SHSG in diagnosing tubal patency was 85.5% and the specificity 96.8%. The positive predictive value for tubal patency by SHSG was 98.3% and the negative predictive value 75%. Comparison made between the two methods showed no significant difference (p = 0.237) in the outcome of these examinations. Discussion The past several years have witnessed advances in the medical and surgical management of infertility. One of the major causes of infertility is blockage of either end of the fallopian tubes. The commonest cause of female infertility in Africa is bilateral tubal occlusion following previous episodes of sexually transmitted diseases or pregnancy complications2 In the investigation and treatment of infertility, it is important to establish that the tubes are patent especially after two years of unprotected intercourse.3 This is necessary because any treatment, such as induction of ovulation and artificial insemination, given without making sure that the tubes are patent may be a futile effort. There has been a rising demand for accurate and non-invasive diagnostic procedures, and this has fostered significant innovations in the technique and equipment used for evaluating infertility. Several methods to assess fallopian tube patency have been described by different authors. These Include HSG, hysterosalpingoscintigraphy, hysteroscopy, laparoscopy and dye test, and tubal insufflations.4 Presently, hysterosalpingography and laparoscopic dye examinations are the most commonly used methods. Ultrasonography is a simple but versatile tool for the investigation of the infertile woman. Its potential has not been fully explored. Like HSG, SHSG is a dynamic imaging procedure that can be monitored on an image display screen during sterile isotonic saline introduction through the cervical canal, but with an added advantage of non-exposure to ionising radiation. Sterile isotonic saline causes less pain than the hyper-osmolar ionic contrast medium.5 There is also a less likely chance of reaction to the medium, in cases of intravasation. There have been reported cases of death from pulmonary embolism following venous intravasation with large amounts of oil based contrast media.5 Tubal and peritubal granuloma formation are thought to be much more common with these oil-based media, although they are no longer in current use. Though not yet popular, sonohysterosalpingogram is a recognised and acceptable
method of assessing tubal patency.1 This method also
has an advantage over HSG in that intravasation of fluid medium does
not interfere
with the
determination of tubal patency as it does with HSG. An additional advantage
of SHSG over HSG is the cost of the examination. While SHSG costs between The accuracy of this procedure can further be improved by using echovist as in Hy-Co-Sy or transvaginal colour-coded duplex sonography (TVCCDS).7 Other workers have further improved the accuracy and sensitivity of this new method of tubal assessment by employing the Sion test. The Sion procedure involves instillation of the pouch of Douglas with approximately 300ml of sterile normal saline to elucidate not only the patency of the fallopian tube but visualise the motility, the fimbriae, and peritubal adhesions if present.8 Furthermore, to facilitate patient’s co-operation during the examination, and to minimise errors due to tubal spasm some form of mild sedation with analgesia or antispasmodic may be administered shortly before the procedure is carried out. In conclusion, SHSG is a comparatively reliable, simple and relatively inexpensive diagnostic and therapeutic procedure in the management of female infertility. It is also relatively free of complications. With expected improvement in this techniques and future advances in sonographic tissue characterisation, it is believed that SHSG will be a first line, office-based diagnostic procedure in the evaluation of tubal patency Thus, it compliments other infertility investigations currently available. The general enthusiasm of patients and investigators for this approach offers a promising future for sonohysterosalpingography Acknowledgement Our gratitude goes to Mr. E. F Adebiyi for the statistical analysis. We also appreciate the assistance of Mr. Dennis Edet in the validation and verification of the raw data. We are grateful to members of the Radiology Department, University of Ilorin, for their contribution, most especially Miss Imoh Akpabio. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01012f1.jpg] [rh01012f3.jpg] [rh01012f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}