 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
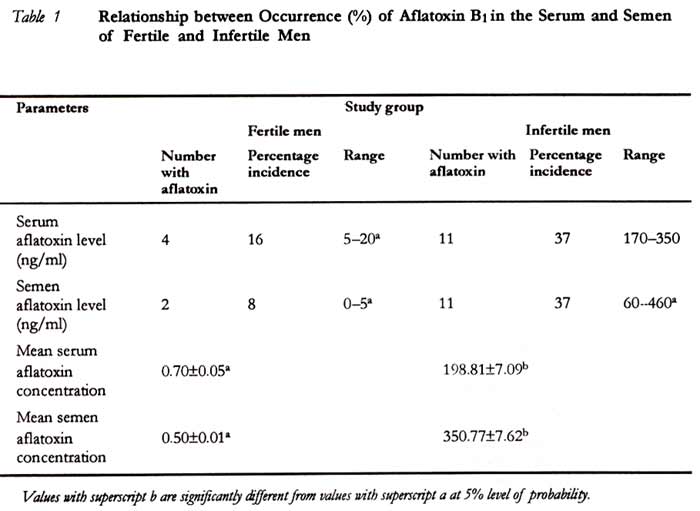
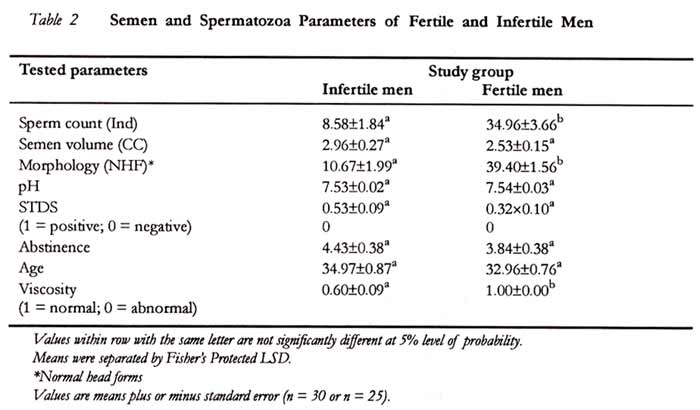
African Journal of Reproductive Health, Vol. 5, No. 1, August, 2001 pp. 106-110 LABORATORY REPORT A Study on the Impact of Aflatoxin on Human Reproduction Nduka Uriah1, Isaiah N Ibeh1 and Flora Oluwafemi1 Code Number: rh01013ABSTRACTInfertility among couples in Nigeria is causing increasing concern. Investigations have shown a relationship between abnormalities in spermatozoa/semen parameters and the incidence of male factor mediated fertility problems in couples. However, the factors responsible for the sudden increase in semen/spermatozoa abnormalities are not fully understood. In this study, blood and semen samples were collected from fifty-five adult Nigerians comprising 30 infertile and 25 fertile control individuals, and screened for the presence of aflatoxin using solvent extraction and quantitation by high performance liquid chromatography. Semen parameters such as volume, viscosity, pH, fructose, spermatozoa count, morphology, and motility were determined. Blood and semen aflatoxin levels in infertile men ranged from 700 to 1392ng/ml and 60 to l48ng/ml respectively and these values were significantly higher than the concentrations of the toxin in fertile men (p <0.05). Deviation from normal in semen parameters showed a definite pattern in infertile men. About 37% of the infertile men had aflatoxin in their blood and semen suggesting that aflatoxins may be a contributory factor to the incidence of infertility in Nigerians since the toxin has been shown to produce deleterious effect on the reproductive system. (Afr J Reprod Health 2001; 5[1]:106-110) KEY WORDS: Aflatoxins, impact, human reproduction, Nigeria Introduction Community-based studies have shown that about 30 per cent of couples in some parts of western Nigeria experience difficulties in conception after two or more years of unprotected sexual relationship around the ovulatory period.1 When extrapolated to the national population of about 100 million people in Nigeria, about 30 million people may be experiencing infertility conditions, although this value may decrease when children and post menopausal couples are excluded from the population, the final figure may still be significantly higher than the estimated 8 per cent of couples experiencing infertility problems globally. This translates to suffering social stigma, a raised frequency of polygamy and divorce, and, in severe cases, suicide.2,3 Regarding gender differences, literature suggests that disorders in males and females account for an equal proportion of infertility. Studies elsewhere4 showed that 8 (about 47 per cent) out of 17 males whose female partners were experiencing difficulties in conception had severe semen abnormalities that could have been responsible for the infertility in the couples. Concerns have been expressed about rising cases of male spermatozoa abnormalities.5,6 Causes of infertility are many, such as sexually transmitted diseases through parasitic diseases, toxic agents to physiological and genetic defects7,8,2 One of the least understood among these factors seem to be the impact of toxic agents, including mycotoxins, on the reproductive performance of human beings. Studies elsewhere have shown the presence of aflatoxins in common food items in Nigeria,9,10 suggesting that exposure of members of this community through diet to aflatoxins may be high. The present study was, therefore, initiated to determine whether aflatoxins are present in the body fluids (blood and semen) of infertile males in this community and to ascertain whether there is a relationship between the presence of aflatoxin and deviation from normal in human male semen/spermatozoa parameters. Materials and Methods Infertile male patients attending the University of Benin Teaching Hospital (n = 30) and a fertile group (n = 25) were used in a case control study. Prior to semen samples collection, the men were advised to abstain from sexual intercourse for about 3-5 days. A study protocol was also administered to all the participants. The parameters that were examined in the two groups of persons included sperm count, motility, morphology, semen volume pH and viscosity, according to the method of Rowe et al.2 All semen samples were cultured in recovery media to isolate any bacteria and fungi present, with a view to excluding microbial infection in addition; a search for any anatomical defects in the gonads of infertile males was done. Aflatoxin Extraction from Human Serum and Semen Blood specimens were obtained from infertile and fertile men intravenously. The blood was allowed to clot at room temperature for 2 hours and serum was separated by centrifugation at 3,000g for 5 minutes. Semen samples were collected either by masturbation or by coitus interruptions after a period of 3-5 days’ abstinence. Aflatoxins were centrifuged at 3,000g for 5 minutes and extracted using hexane-chloroform extraction method of Lamplugh.11 The dried extracts were redissolved in 1ml methanol: water (50:50), and 20% of the resultant solution was fed into high performance liquid chromatography (HPLC) for quantitation of toxin at flow rate of 1.5/min and detection at 365min at 1.0atm (Vydac microbore C18 RPC Column). The identity of extracted toxins was confirmed according to the method of Van Egmond and Stubblefield.12 Statistical AnalysisData were analysed by two-way analysis of variance (ANOVA) and means were separated using Fisher’s protected LSD. T-test was used to determine the significance of the differences in values. P values less than 0.05 were considered to be significant. ResultsAflatoxin B1 content of serum and semen samples obtained from infertile men is shown in Table 1. Twenty-two out of the 60 samples of serum and semen of the infertile men had aflatoxin B1 ranging from 60ng/ml to 148ng/ml. In cases where aflatoxin B1 was present in both semen and serum of fertile men group, the aflatoxin B1 was always higher in the serum than in the semen. More respondents of the infertile men group had higher concentrations of aflatoxin B1 in their semen than in their serum, with aflatoxin values of serum and semen at 170 and 350ng/ml respectively There was a significant statistical difference in aflatoxin B1 content of blood and semen from the fertile and infertile groups at 95% level of confidence (p <0.05). Semen parameters in Table 2 show severe deviation from normal in sperm count, morphology and motility in the infertile group when compared with the WHO standard. In contrast, the semen parameters of the fertile group did not differ from the WHO standard for sperm count and morphology (20 million cells/ml and 30% normal head forms respectively). Some of the respondents in the infertile group had no live spermatozoa (azoospermia), while others had spermatozoa that were immobile and with abnormal headshape. Mean sperm count, morphology and motility of infertile men were statistically different from the fertile group (p < 0.05). There were no statistically significant differences with respect to semen volume, pH, age, days of abstinence and amount of fructose between the two groups of males investigated. Discussion One of the important aspects of infertility management is to identify the cause(s) and suggest possible solutions.13 From the present case control study of infertile men in the University of Benin Teaching Hospital, aflatoxin B1 was present in 37% of the infertile respondents. In a normal situation, ingested aflatoxin is metabolised at the liver to intermediate and end products, which are more water soluble and easily excretable via urine. When this liver function becomes inefficient or impaired, accumulation of aflatoxins in the system occurs. This perhaps explains why aflatoxins were found and at higher concentrations in infertile men when compared with the control group (Table 1). Aflatoxin is a potent mutagen.14 Mutation has been found to prevent fertilisation in house mouse15 by way of severe malformation in epididymal spermatozoa. The presence of aflatoxin in the infertile respondents, therefore, might have played a contributory role in the impaired semen parameters observed in this study. In some of the respondents, there were no live spermatozoa (azoospermia), and aflatoxin B1 levels were as high as 692, 698, 750 and 1450ng/ml. The capacity of the human sperm to fertilise female ova principally depends on sperm motility and membrane integrity.16 In-vitro studies confirmed the coupling of aflatoxin to DNA, forming aflatoxin-DNA adducts.17,18 Damage to the genetic material at both the gene and chromosome levels may lead to obvious abnormalities in sperm in man.19 The toxicity of dietary aflatoxin in mammals has been extensively studied20,21 and several factors have been adduced to contribute to aflatoxin tissue toxicity. One of such factors is the ability of aflatoxin to undergo translocation. This was clearly seen in the results as aflatoxin B1 was found in the blood and then in semen. The toxin has passed through several organs and tissues, thus exposing the ingested toxin to several parts of the body. The translocation of aflatoxin B1 from blood to semen through the blood testis barrier was very effective. This can be seen in the ratio of concentration of aflatoxin B1 in the semen to its concentration in blood (Table 1). This storage of aflatoxin in semen might set up an oxidative stress in the testicular region following the depletion of preformed antioxidants. The storage of aflatoxin B1 in the semen eliminates its excretion through urine or sweat or saliva or faeces, thus enhancing its toxicity in the testes. The impact of aflatoxin in the testes seems to be time and concentration dependent since some of the fertile men had aflatoxin in their blood (Table 1). Results obtained from this study in the protocol administered to respondents showed that all participants ate basic staple foods such as garri, yam, beans, rice, maize, bread, groundnut, etc. Ninety per cent of aflatoxin in humans is due to dietary intake of toxin.22 Studies by Ibeh et al in Benin City confirmed the presence of aflatoxin in staple foods such as garri, beans, yam flour, cassava flour, melon, onion, rice, plantain, red pepper and eggs.10 It is, therefore, likely that the source of aflatoxin in the body fluids of individuals investigated was food contaminated by mycotoxin. Longer exposure to dietary intake of aflatoxins at high concentrations in the infertile than in the fertile control group, in addition to faulty liver clearance, may be the cause of the higher semen and serum levels of aflatoxins. The higher concentration of aflatoxins in semen than in serum suggests that semen is a sequestration point for ingested aflatoxins. Although this study indicates that aflatoxins may have a negative effect on fertility, more studies are needed to ascertain the generalisability and impact of this relationship. Acknowledgement We are grateful to the University of Benin URPC for her support through the Research Grant REG/E & R. 175/Vol. URPC/1996/97.7. REFERENCES
Copyright 2001 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh01013t2.jpg] [rh01013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}