 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 1, August, 2002 pp. 20-31 (Re)Defining Reproductive Health With and For the Community: An Example of Participatory Research from Mali Sarah Castle1, Sidy Traore2 and Lalla Cisse2 1Centre for Population Studies, London School of Hygiene and Tropical Medicine, 49–51 Bedford Square, London WC1E 3DP. E-mail: sarah.castle@lshtm.ac.uk 2Save the Children UK, BP 2145, Bamako, Mali. E-mail: s.traore@scfuk.org.ml Code Number: rh02006 ABSTRACT Qualitative research was carried out in central Mali to inform the development of curricula for an intervention to improve young people's reproductive health. Both the young people and `societal gatekeepers' (including religious leaders and traditional healers) perceived reproductive health to comprise the social dynamics in which reproductive health decision-making is embedded and not just the biological aspects of sexual relations and fertility. Their definitions of reproductive health reflected social taboos about pre-marital sex, infidelity and illegitimate children, and comprised holistic notions of bodily and spiritual cleanliness. It is argued that the `Cairo' definition sees many of the social factors identified by respondents as comprising the context or background of reproductive health. The findings presented here indicate that local populations may see them as integral to the concept itself. It is discussed how the 'Cairo' definition of reproductive health needs to be made culturally specific in order to facilitate programme design and implementation. (Afr J Reprod Health 2002; 6[1]: 20–31) RÉSUMÉ La (Re)définition de la Santé Reproductive avec et pour la Communauté: Un exemple de la Recherche Participative du Mali. Une recherche qualitative a été menée dans le Centre du Mali afin d'influencer le développement du programme scolaire destiné à l'intervention qui permettra d'améliorer la santé reproductive des jeunes gens. Les jeunes gens et les gardiens de la société (y compris les leaders religieux et les guérisseurs traditionnels) ont aperçu la santé reproductive comme étant composée de la dynamique sociale à l'intérieur de laquelle est gravée la prise de décision sur la santé reproductive et non pas seulement les aspects biologiques des rapports sexuels et de la stérilité. Leurs définitions de la santé reproductive reflétaient les tabous sociaux concernant le sexe avant le mariage, l'infidélité et les enfants naturels; elles comprenaient aussi les notions holistiques de la propriété corporelle et spirituelle. Nous avançons l'argument que la définition de `Cairo' voit beaucoup de facteurs sociaux qui ont été identifiés par les répondants comme constituant le contexte ou les éléments de la santé reproductive. Les résultats que nous présentons ici montrent que les populations locales peuvent les percevoir comme étant intégral au concept lui-même. Nous avons discuté la manière dont la définition de `Cairo' de la santé reproductive doit être rendue culturellement spécifique afin de faciliter la conception et la mise en oeuvre du programme. (Rev Afr Santé Reprod 2002; 6[1]: 20–31) KEY WORDS : Young people, participatory research, reproductive health, Mali BACKGROUND The 1994 International Conference on Population and Development (ICPD) in Cairo called for a comprehensive client-centred view of reproductive health in order to access and include some of society's most vulnerable groups including young people.1-2 More than 180 states took part in negotiations to finalise a Programme of Action in the area of population and development for the following 20 years. The Programme of Action endorses a new strategy focused on meeting the needs of individual women and men rather than on achieving demographic targets. The Programme is orientated by the following definition of reproductive health, which resulted from the input of governmental and non-governmental representatives, policy makers and advocates.
This definition (often referred to as the `Cairo' definition) frequently acts as an operational basis for interventions implemented to address issues that emerged from the conference. The Programme was heralded as reflecting local priorities and seeking to address them using culturally appropriate solutions emerging from communities themselves. Indeed, a summary of the initiative five years further on states that ICPD served to place people firmly at the centre of development efforts as advocates for their own sexual and reproductive health, rather than as passive recipients of external inputs.4 This new approach may have appeared daunting to those running programmes where the main focus had been on services (for example, family planning provision or STI treatment) rather than on the social context or precursors leading to the clients' visits. Thus, the difficulty lay not only with unfamiliarity of the language and approach encompassed in the ICPD Programme but in knowing exactly how to execute it by those used to a medical rather than social focus to reproductive health. In addition, research results presented here indicate that the definition put forward by the Cairo conference may not accurately reflect what emerges from local communities. Rather, it is likely that it comprises the perspective of activists and actors whose `world-view' may, in some cases, not be those of the populations that they seek to represent. Ironically, and contrary to the spirit of ICPD, local communities can therefore sometimes find themselves in the role of passive recipients of programmes orientated around definitions coined outside their social world and realm of understanding. The findings presented here that the Cairo definition needs to be adapted for use in specific cultural contexts. Without such adaptation, community participation in, and ownership of, reproductive health interventions (shown to be the key to their successful implementation) are likely to be limited. In a review of activities in the years following the Cairo declaration, the goals of the original conference remained commendable, but problems were identified with their implementation.5-6 These were largely seen to be related to a lack of political will, legislative backing, support for NGOs, adequate infrastructures and to a lack of co-ordination between sectors.7-9 However, no critique was undertaken of the acceptability of the definition as a factor which may hamper attainment of the goals and aims of the Cairo conference. Despite the various short-comings described in this paper, the definition comprises a substantial step forward in viewing reproductive health as a holistic concept encompassing physical, mental and social well-being. Since the declaration was made, this broader view has enabled issues such as domestic violence and sexuality to be put on the reproductive health agenda.10-11 These address the psychological dimensions borne out of the way in which gender relations are played out at the individual level as well as the physical attributes of reproductive health. In this vein, ICPD made it clear that reproductive health is not simply a concept but a spectrum of conditions, events and processes through life, ranging from healthy sexual development, comfort and closeness and the joys of childbearing, to abuse, disease, disability and death.12 As will be reflected in this paper, these aspects are central to the conceptualisation of reproductive health by many people in the communities where programmes that emerged out of the Cairo conference (and its subsequent follow-ups) are implemented. Their testimonies recount how reproductive health comprises an active approach to ensuring optimal well being for men and women and as such has to be considered as a process rather than simply a terminology. Evidence suggests that in the fields of reproductive and sexual health, community understanding and engagement are key to eliciting continuing participation and commitment among local people.13-14 For example, the most successful HIV prevention programmes and other interventions to improve reproductive health outcomes build partnerships and trust between people and develop and incorporate communities' skills and knowledge.15 It is argued below that it is very difficult to build such partnerships and incorporate such skills if the definition of key concepts differ between providers and users of the intervention. This research work was carried out as part of a preparatory work for the development of curricula for an intervention that aims to improve young people's reproductive health in central Mali. In particular, the programme seeks to lower their risk of becoming infected with HIV. Qualitative methods were used to ascertain local people's priorities and concerns generally and in terms of their reproductive health, with a view to better tailoring the intervention to their needs and increasing their ownership of the project. In particular, young people and community stakeholders were asked for their own definitions of reproductive health so that the intervention could be orientated around local perceptions and insights. It was hypothesised that this would increase their ability to relate to the programme and their motivation to participate. The research describes how local definitions of reproductive health take account of the societal and familial forces that drive decision-making in this domain. It also shows how necessary it is to recognise that the elements people perceive to comprise reproductive health are often a reflection of social rules and societal dynamics (including gender and marital relations) together with views about the role and status of women. These issues are not viewed as comprising the social context or background of reproductive health outcomes and decision-making and not as enabling or facilitating factors as the Cairo agenda propounds. Rather, they are viewed as intrinsic elements of reproductive health per se and are at the centre rather than periphery of the definition. Qualitative and Programmatic Approaches to Eliciting, Using and Evaluating Local Knowledge In the last decade there has been an increase in the recognition that qualitative research, and in particular anthropology, has a crucial role to play in the design, implementation and evaluation of public health interventions. The emergence of rapid rural appraisal techniques16-17 or rapid assessment procedures18-19 paved the way for the quick and dirty collection of anthropological and ethnographic data as a means to eliciting the cultural foundations on which programmes would be built. However, in many cases the collection of qualitative data had little influence on programme design, as in some situations the framework of the project was often either already established before the research was carried out or went ahead despite is findings.20 A fundamental obstacle to the use of qualitative research as a basis for programme development is that the key characteristics of knowledge and behaviour sought by qualitative researchers and by those who implement programmes tend to be different. Public health “specialists” involved in programmes in a clinical or managerial capacity tend to look for measurable empirical criteria or outcomes that can be used as indicators of successful behaviour change. By contrast, anthropologists seek to understand emic or local folk models of illness causation and classification and to focus on the processes and context of decision-making. Nowhere has the tension between the two perspectives been more evident than in the formulation and application of definitions of primary health care concepts in relation to programme implementation. Clinicians or managers may refer to local `beliefs' with an innate sense of scepticism or as suspicion or classify them as `cultural factors' or `local wisdom'.21-22 By contrast, empirical evidence of the population's knowledge of key `facts' are acknowledged to be the `right' or `proven' truth because they are measurable and comparable. For example, knowledge of the use of oral rehydration solution and of the cause of malaria or methods of HIV prevention are often considered objective indicators of programme impact and as such are frequently demanded by funding agencies or global programme offices. For example, in Africa, a target may include a 40% rise in reported condom use with the present or last sexual partner in the year after implementing HIV/AIDS education or an increase in the proportion of the population with correct knowledge of HIV transmission.23 However, in the anthropological lexicon, beliefs and knowledge are not contrasting terms.24 Belief systems contingent on traditional “world views” are less easy to empirically measure and are less comparable, but may be more important in determining programme success. Such systems may be reiterated, changed or modified according to evidence elicited from social exchanges and social relations. These processes create evolving and reflective systems of local knowledge which impact on the target population's perception and use of the programme. The most effective way of understanding these social processes and the beliefs they form and influence is through qualitative research, which is thus crucial to programme design.25-27 The notion that the recognition and management of an illness takes place within a constellation of kin and community relations is as true for reproductive health as are other elements of primary health care.28 However, rarely are these social dynamics placed at the heart of conventional or generic definitions of reproductive health or even referred to as core elements of international debate and advocacy on the subject. The fact that reproductive health cannot be disassociated from the familial and community relations in which it is situated has been noted elsewhere in West Africa. In Senegal, a policy project review of post-Cairo reproductive health activities in Senegal noted that one government respondent as saying that the family is the basic social unit in Senegal, and reproductive health is only acceptable when expressed in terms of the family.1 Our evidence suggests that the same is likely to be true in neighbouring Mali. Programmes and interventions need to recognise that issues that are not directly health related, such as marital and family relations, gender and age based hierarchies and the role and status of women, crucially impinge on decision-making concerning every aspect of sexual and reproductive health. Despite talking of “social well-being”, this element of the Cairo definition seems marginal to the other aspects that focus on fertility regulation and outcomes. Issues such as gender relations and the need for social policies to help meet the ICPD goals (such as improving women's status through education and access to economic resources) are addressed in the broader Programme of Action. However, they are conceptualised as facilitating factors rather than as key components of reproductive health.4 Placing social relations at the heart (rather than at the periphery) of the definition seems to be crucial to local interpretations of reproductive health among the communities described in this study, and probably more widely in both the developed and developing countries. The definitions of reproductive health presented in this paper show how local knowledge can be used as a basis for programme design whilst at the same time `objective' aims and indicators can be pursued without conflict. In fact, using qualitative research to structure the intervention around local rather than outside definitions of reproductive health is likely to facilitate the overall attainment of aims that project funding organisations and international agencies want to achieve such as, for example, maximising family planning coverage or increasing knowledge of HIV. Potential participants are more likely to be motivated to participate in a project that they themselves have helped to orientate. In addition, the paper describes how the qualitative research findings were presented back to the participants to gain their views on ways the results might inform future intervention. Thus, qualitative research was useful as a means to opening up a dialogue between programme managers and recipients as well as in terms of gathering local knowledge and applying it to programme design. This participatory dynamic approach contrasts sharply with others from around the world where generic definitions are felt to be appropriate for programme orientation. For example, when defining a reproductive health package for India, the Population Council uses the following definition, which pays little attention to the cultural or social aspects of health and well being and rather emphasises the biological aspects of sex and reproduction:
Similarly, Pathfinder orientates programmes for young people around the following definition:
To date, those who use the Cairo definition (or one similar to it) as a basis for their activities tend to emphasise the medical aspects of reproductive health rather than taking a holistic view encompassing the social context in which health-seeking or risk-taking behaviour occurs. The lack of reference to the social or family context of reproductive health or to the broader notions surrounding it means that without modification definitions such as that formulated at Cairo are unlikely to serve as optimal operational tools in the field. Improving Young People's Sexual Health in Mali The Demographic and Health Survey for Mali (1995–96) showed that knowledge about sexual health issues was relatively good among young people but that the application of this knowledge was poor.31 For example, although 89.6% of young men aged 15–19 years had heard of HIV/AIDS, only 22% had used the condom during their last sexual encounter. Three years later, a survey of adolescent sexual behaviour in Mali carried out by the London School of Hygiene and Tropical Medicine (LSHTM) and the Centre d'Etudes et de Recherche sur la Population pour le Développement (CERPOD) found a similar gap between knowledge and behaviour. For example, although nearly all adolescents had heard of HIV, and over half had heard of other STIs, 15% of boys and 9% of girls had multiple partners at the time of the survey.32 The same survey developed a locally appropriate instrument to look at psychological characteristics that may help explain the gap between knowledge and behaviour.33 The analyses indicated that psychological factors may influence sexual behaviour and contraceptive use when controlling for educational and economic status. For example, girls with high self-esteem were more likely to have had sexual intercourse while those with an internal locus of control were more likely to have ever used a modern method of contraception.34 ISRA (Innovation en Santé de la Reproduction des Adolescents) is an initiative funded by the Department for International Development (DFID) and the Rockefeller Foundation to improve young people's sexual and reproductive health in central Mali. ISRA is being implemented by Save the Children (UK) in collaboration with the Regional Ministry of Health and the Regional Department of Social Affairs. It is notable that both Save the Children and the principal funders, DFID, use the Cairo definition of reproductive health to guide their policies and programmes. The 14 towns or large villages that will be included in the ISRA programme are in an extremely arid area characterised by widespread poverty. The majority of the people are of Peulh (Fulani), Bozo or Dogon origin interspersed with small pockets of Bambara populations such as the village of Bore, which was one of the four sites for the qualitative research. Modes of production vary by ethnicity with the Peulh practising agro-pastoralism, the Bozo relying primarily on fishing, whilst the Dogon and Bambara carry out millet cultivation. These two groups also rely heavily on remittances from migrants to Côte d'Ivoire. Young men may move seasonally to work as casual labourers while the girls go into domestic service in the cities. This not only exposes them to the modern media and urban ways of life but also to sexual health risks, as many turn to formal or informal sex work due to the irregular payment or non-payment of salaries.35 The Demographic and Health Survey indicated that 90% of women and 85% of men in the Mopti region had never been to school although this is likely to be slightly lower for the younger age groups. Median age at marriage for women was 16.0 and 25.8 for men.31 Fertility and mortality were high, indicating that the demographic transition was yet to begin. Motherhood occurred early, with the median age at first birth being 18.8 years. By age 19, 22% of women had experienced one or more live births. Socio-cultural values mean that childbearing is expected to take place within marriage resulting in the fact that pre-marital pregnancies often end in abortion.36 ISRA grew out of the research described above and recognises that increasing urbanisation, modernity and widespread rural-urban labour migration often send conflicting messages to young people while eroding the traditional sources of advice and support concerning sexual health matters from what can be termed `societal gatekeepers'. Specific beliefs and practices driving adolescents' sexual decision-making are often formed and reinforced by `gatekeepers' of information or customs within the community. Gatekeepers may include religious leaders and clerics (marabouts), caste members, traditional healers, traditional birth attendants, and praise singers (known as griots). These socially powerful individuals frequently control (or used to control) the gaining and transmission of sexual health knowledge by young people and impart norms relating to gender roles in their communities. For example, members of the blacksmith caste used to be responsible for giving information to young girls before their wedding day about how to give sexual satisfaction. Now, however, this duty has largely been abandoned. The intervention targets 15–19-year-olds and will specifically seek to:
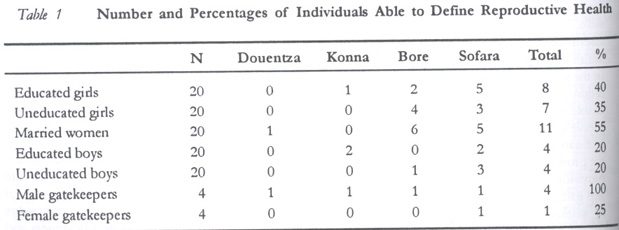
The indicators outlined in the project's logical framework are based on previous research findings and include (a) increasing the reported use of condoms from 11% to 20% among girls and (b) decreasing the percentage of unmarried adolescents with more than one concurrent sexual partner from 15% to 10% (boys) and from 9% to 5% (girls). However, at the same time the project seeks to encourage the community to engage as active advocates for young people's sexual health. This process of participation is seen as a goal in and of itself and not simply as a factor facilitating the goals described above. A baseline survey (including behavioural and biomedical markers) is currently being carried out by ISRA and the curricula for the two sets of peer education programmes are being developed. The intervention was formally implemented at the beginning of 2002. Qualitative Research to Inform the Curricula Development Qualitative research was carried out with young people and societal gatekeepers in four representative communities involved in the intervention. Three main sets of qualitative data were collected with a view to eliciting definitions of reproductive health, together with problems and priorities relating to reproductive health and other domains. Firstly, one hundred young respondents and eight gatekeepers were asked to give a definition of reproductive health and its component elements. Secondly, they were asked to free-list reproductive health and non-reproductive health problems affecting young people and to rank them in order of seriousness. Free listing involved asking people to list spontaneously the members of a domain (a culturally bound entity) such as diseases, plants, occupations or animals. Analyses of how often an item is cited and where it appears on the free list can tell us a lot about its importance.38 Thirdly, in-depth interviews were carried out with additional 48 gatekeepers and 20 focus group discussions were conducted with additional young people. These addressed the communication of reproductive health issues, inter-generational consistency and conflict regarding perceptions of young people's behaviour and values, and their suggestions as to the ways in which the two peer education programmes could work together. Interviews and discussions on all these subjects were carried out with married and unmarried women with little or no education, educated single women and men, and men with little or no schooling. The sample was picked purposively by following up contacts made through existing formal and informal community associations (such as youth groups) and commercial, religious or traditional structures. Contact with the respondents and social gatekeepers was facilitated by careful awareness-raising with the village chiefs and their counsellors. The large amount of information collected was analysed and used to compile a report that served as the background document to inform the curriculum development.39 Subsequently, the main results were presented back to selected young people and gatekeepers in a series of informal workshops to elicit their reactions to the main findings and suggestions for the curriculum design. In this way, the communities selected participated not only in furnishing the data but also in its analysis and application. Due to the enormity of the data collected, only the parts relating to the definition of reproductive health is presented here. Definitions of Reproductive Health The interviewees were asked if they knew what `reproductive health' was by asking them in Fulfulde what they understood by celal rimo (the health of one who gives birth) or celal beyngu (the health of reproducing, literarily meaning health associated with having progenitor or descendants). In Bambara, the concept was translated as keneya ko denroro lahalaya la, which again reflects the idea of health related to reproducing descendants. The vocabulary used in the definition was chosen after discussion with the interviewers and health workers who were used to talking about reproductive health in these two languages. Their replies were translated into French, noted by the interviewer and presented here in English. Table 1 shows the number of people interviewed in each setting who were able to give a definition of reproductive health and shows that on the whole most young people had never heard of the concept. However, the youth group with the highest percentage of respondents who had heard of the notion was the married women. This may be because they are likely to have given birth and had contact with antenatal or maternity services where they may have heard the term. Only 40% of educated women and 20% of educated men had heard of the idea reflecting the fact that the school curriculum in Mali does not generally address this topic. A slightly higher number of uneducated girls (7), compared with uneducated boys (4), had heard of the topic. Among the eight gatekeepers interviewed, all of the elderly men were able to give a definition, compared with just one elderly woman. This may be because a higher number of them had probably been to school, or because they may be more likely to listen to the radio where reproductive health is sometimes discussed. The definitions given by those who had some notion of what reproductive health meant were often much broader than those used by public health professionals or reproductive health `specialists'. Many respondents saw reproductive health as a means to adhere to specific social rules and avoid certain taboos (such pre-marital pregnancy and infidelity), whilst women in particular emphasised the role of marital relations, love and social support to ensure the holistic well being of mind and body.
The notion of hygiene and cleanliness as pre-requisites for good reproductive health were also strongly highlighted by many respondents.
One male and two female respondents emphasised the place of sexual relations within marriage and the importance of pre-marital abstinence and post-marital fidelity.
The women also brought up the idea of long-term care and raising children under the rubric of reproductive health. As noted by one of the respondents already cited, having children was seen as a means to happiness and overall well being. However, other respondents noted that childbearing also entails other important responsibilities such as getting them vaccinated. In this sense, reproductive health thus impinges on child health and illness prevention. Thus, according to the respondents, reproductive health cannot be seen as separate from other aspects of primary health care.
Interestingly the male respondents had a more `medical' view of reproductive health — one that is perhaps closer to that of the health professionals and those involved in coining the Cairo definition. They placed a particular emphasis on the prevention of STIs and HIV/AIDS.
However, some young people viewed issues such as condom use in the context of the social taboo against illegitimate children, which, as for the women, featured centrally in the definition of reproductive health.
Among the four older male gatekeepers interviewed, all had a holistic view of reproductive health, taking into account psychological and spiritual well being as well as physical condition.
Like the younger respondents they mentioned the importance of hygiene and nutrition in assuring the overall well being of mothers and children and also emphasised the role of birth spacing.
The one elderly female gatekeeper interviewed who was able to give a definition also had a holistic view of reproduction, drawing attention to elements relating to hygiene, childbirth, STIs and HIV/AIDS.
These definitions of reproductive health indicate that it is deeply embedded in notions of social and marital relations and reflects broader community dynamics and priorities. Among these priorities are requirements for women to be faithful and for children not to be born outside marriage. In addition, it encompasses not just pregnancy and birth but also the long-term upbringing of children together with the need for spiritual and bodily cleanliness. The fact that these culturally defined expectations were integrated spontaneously into the definition means that reproductive health cannot be separated from the social context in which it occurs. As described, these definitions and other aspects of the qualitative research were presented back to selected gatekeepers and young people via a series of workshops to try and ascertain how they view the research findings. The young people reiterated that reproductive health reflects social relations and in particular marital dynamics. Indeed, the principal example they gave of a reproductive health problem was one relating to gender-based conflict. They emphasised the need to address domestic violence and noted how this is often related to women wanting to seek to improve their reproductive health by using family planning in the face of their husbands' opposition. Their definition in the workshop, as in the field, was orientated around the idea that reproductive health results from inter-personal relations and cannot be separated from the social dynamics of a couple, household or community.40 Likewise, in a parallel workshop, the gatekeepers cited the social forces that lead to reproductive health problems as part and parcel of the same definition reiterating what had been brought up in the individual interviews in the field. When asked to define issues pertaining to reproductive health, they noted social rather than biological problems including sexual promiscuity, labour migration and the disrespect of parents by their offspring.41 Indeed, when both groups were asked how to improve reproductive health, their perceived solution was found in the social rather than the biological domain, with their consensus suggesting that improved parent-child communication is the answer. Thus, these issues of social control, gender relations and poverty (which are in turn related to labour migration) will become central to the reproductive health curriculum and be given as much weight as the information relating to clinical and biological factors and the provision of services. CONCLUSION The qualitative research presented here indicates that among the central Malian communities, reproductive health is perceived to reflect the social and community dynamics in which reproductive health decision-making is embedded and to comprise the biological aspects of sexual relations and fertility. Respondents frequently conceptualised reproductive health as representing, certainly for women, the importance of virginity upon marriage, fidelity to the husband, and a taboo around illegitimate children. Notions of social support and spiritual well being were also integrated into the local meanings of the term. In particular, the definitions given by respondents frequently emphasised the importance of overall cleanliness and hygiene as pre-cursors to general and reproductive health. Furthermore, the definitions went beyond pregnancy and birth and referred to the long-term raising of children as a means to personal happiness and divine benediction. Although the Cairo definition of reproductive health mentions “social well being”, it does not explicitly reflect the extent to which social relations influence the way in which these respondents conceptualise reproductive health. In the “real-life” definitions presented here, marriage, family and the community are central to the whole premise and do not simply comprise its context. Definitions that emphasise the medical aspects of reproductive health and consider the social dynamics in which they are situated as facilitating rather than integral factors are unlikely to constitute useful operational frameworks for programme implementation. As shown here, these social issues are the heart of local concerns and priorities rather than merely being background factors against which reproductive decision-making is said to occur. As described, the aim of this research was to inform the development of curricula for young people and societal gatekeepers for intervention to improve young people's sexual and reproductive health in central Mali. The curricula will thus be based on multiple definitions that recognise that the social dynamics of reproductive health decision-making are central to local perceptions of reproductive health. The themes addressed by the curricula will, therefore, not simply refer to the biomedical elements of reproductive health in isolation, but rather integrate them into the concerns described above, which are of importance to the potential participants. Thus, gender relations, labour migration, parental communication and social taboos and rules regarding pregnancy and marriage will be central to the peer-led discussions. Facilitators and peer educators among the young people and gatekeepers will be carefully trained to engage the community in a dialogue about its own internal logic and reproductive health discourse. The intervention thus acknowledges that local beliefs and local knowledge have an important role to play in orientating the programme and can be used to promote debates and discussion from within rather than imposing topics from the outside. Thus, the qualitative research has enabled the involvement of participants from the beginning in defining the operational rubric of the project on their own terms. In this way, it is hoped that the content of the curricula will be accepted and validated within the social structures that shape community and family relations, and that these relations will in turn be used to promote better reproductive health outcomes. Thus, as described above, reproductive health is an approach not just a concept. As recognised by the WHO, when we use the language of ICPD, we talk about health needs, but we also talk about rights, equity, dignity, empowerment, self-determination and responsibility in relationships. Reproductive health is an approach to analysing and then responding comprehensively to the needs of women and men in their sexual relationships and reproduction.12 If ICPD is to truly be about placing people at the centre of development efforts,4 then the programme implementers have to be able to listen to the way reproductive health is viewed in the community. They need to adopt a definition of reproductive health that is locally generated in order to make the programme accessible and acceptable, and to engage the community as partners in, not as recipients of, the intervention. ACKNOWLEDGEMENTS The authors are grateful to the study participants and their community leaders for their time and patience. We also thank Ms. Valerie Lépine of Africa Consultants International, Dakar, Senegal, for her help with the curricula development, and Dr Stan Yoder of Macro International for his helpful comments. The study and intervention are funded by the Department for International Development (Sexual Health Innovation Award) and the Rockefeller Foundation. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02006t1.jpg] |
| |||||||||

{kind=link}