 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
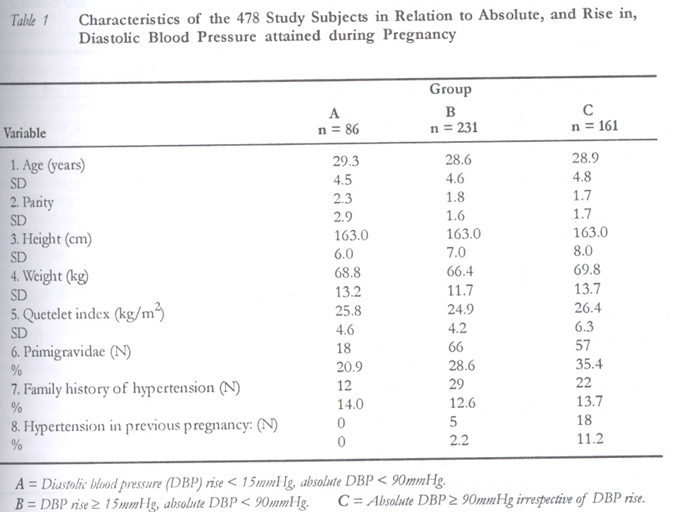
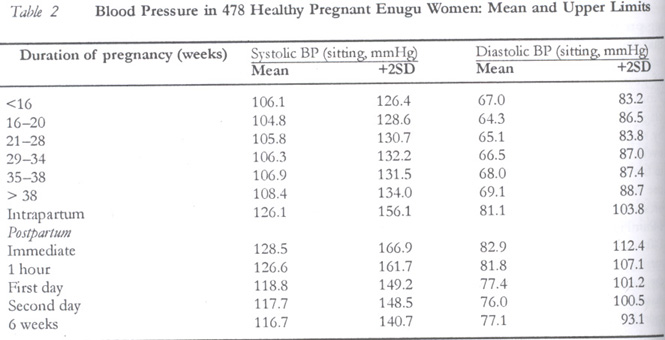
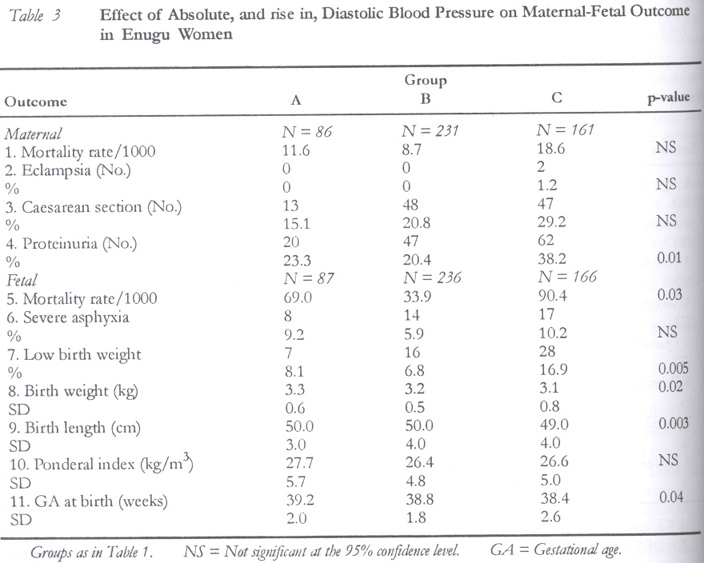
African Journal of Reproductive Health, Vol. 6, No. 1, April, 2002 pp. 32-40 Prognostic Value of Absolute versus Relative Rise of Blood Pressure in Pregnancy HE Onah1 1Dr H. E. Onah, Department of Obstetrics and Gynaecology, College of Medicine, University of Nigeria Teaching Hospital, Enugu, Nigeria. Tel: 042-256263, 090-503826 E-mail: hyacinon@infoweb.abs.net Code Number: rh02007 ABSTRACT This study evaluated the prognostic value of absolute versus relative rise in blood pressure during pregnancy at the Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Enugu, Nigeria from 17th December 1997 to 31st March 1999. The study sample consisted of 515 consecutive healthy antenatal subjects of the hospital who satisfied the inclusion criteria. The study involved a longitudinal measurement of variables such as blood pressure and anthropometric data of the subjects as well as the maternal mortality rate, caesarean section rate, incidence of eclampsia and proteinuria, perinatal mortality rate, incidence of severe asphyxia and low birth weight, mean birth weight, birth length, ponderal index and gestational age at delivery. Differences in these indices between different groups of the subjects were compared using the chi-square test for categorical variables and one way ANOVA for continuous variables. Grouping was based on the absolute systolic/diastolic blood pressure (SBP/DBP) and relative rise in SBP/DBP from mid-pregnancy until delivery at term. The absolute blood pressure of 140/90 mmHg was a better predictor of feto-maternal outcome than a relative rise in the systolic/diastolic blood pressure from mid pregnancy, which did not reach this absolute level. We conclude that in the Nigerian obstetric population, the practice of diagnosing pregnancy hypertension on the basis of a relative blood pressure rise of 30/15 mmHg alone without reference to the absolute blood pressure level needs to be reviewed. (Afr J Reprod Health 2002; 6[1]: 32–40) RÉSUMÉ La Valeur Pronostique de l'Absolu par Rapport à la Hausse de la Tension Artérielle Pendant la Grossesse. L'etude a évalué la valeur pronostique de l'absolu par rapport à la hausse relative de la tension artérielle pendant la grossesse, au Departement de l'obstétrique et de la gynécologie du Centre Hospitalier Universitaire à Enugu au Nigéria, du 17 décembre 1997 au 31 mars 1999. L'échantillon comprenait 515 sujets prénatals consécutifs en bonne santé, tirés de l'hôpital et qui ont satisfait le critère de l'inclusion. L'étude concernait les mesures longitudinales des variables tels la tension artérielle et les données anthropométriques des sujets aussi bien que le taux de mortalité périnatale, l'incidence de l'asphyxie sévère et le faible poids de naissance, poids de naissance moyen, la taille à la naissance, l'indice pondéral et l'asphyxie gestationnelle à l'accouchement. Les différences des indices qui existent entre les groupe différents groupes de sujets ont été comparées à l'aide de test chi-carré pour les catégories viables et ANOVA à sens unique pour les variables continus. Le groupement a été basé sur la tension artérielle systole/diastole absolue (PAS/PAD) et la hausse relative dans PAS/PAD depuis la mi-grossesse jusqu'à l'accouchement à terme. La tension artérielle absolue de 140/90 mmHg est un meilleur indice de l'issue féto-maternelle qu'une hausse relative dans la tension artérielle systole/diastole à partir de la mi-grossesse, qui n'a pas atteint ce niveau absolu. Nous concluons que dans la population obstétrique nigériane, la pratique de la diagnostic de l'hypertension artérielle pendant la grossesse en se fondant uniquement sur une hausse relative de la tension artérielle de 30/15 mmHg sans référence au niveau de la tension artérielle absolue devrait être réexaminée de nouveau. (Rev Afr Santé Reprod 2002; 6[1]: 32–40) KEY WORDS : Absolute, relative, rise, blood pressure, pregnancy, prognosis INTRODUCTION Hypertension during pregnancy has traditionally been defined on the basis of an absolute blood pressure of 140/90 mmHg1-3 or a relative rise in systolic/diastolic blood pressure of 30/15 mmHg.3 In a comparison of the absolute and relative rise in blood pressure during pregnancy in British women,4 it was shown that the former was prognostically better than the latter. In a latter study,5 it was found that the diastolic blood pressure could rise to as much as 15mmHg during pregnancy without the appearance of proteinuria as long as the diastolic pressure does not reach 90mmHg. In Nigeria, both definitions of hypertension in pregnancy are widely used with preference for 30/15mmHg relative rise, because of the assumed low blood pressures in the population. However, whether or not a relative increase in systolic or diastolic blood pressure without an absolute increase to at least 140/90mmHg constitutes hypertension has recently become controversial.3,6,7 To the best of the author's knowledge, no study has compared the prognostic value of the two definitions in Nigerians. This comparison was done in the present study. MATERIALS AND METHODS The study was longitudinal and it took place at the Department of Obstetrics and Gynaecology, University of Nigeria Teaching Hospital, Enugu, Nigeria, from 17th December 1997 to 31st March 1999. It was approed by the hospital's ethical committee. The study sample consisted of consecutive healthy antenatal subjects of the hospital satisfying the following criteria: no history or evidence of renal disease, diabetes mellitus, chronic hypertension or other chronic medical diseases and first antenatal clinic attendance before 16 weeks of gestation. The study involved the longitudinal measurement of many variables. Because of this, three resident doctors and five nurses took part in the study in addition to the investigator. To minimise inter-observer errors, the participants were trained during the first two weeks of the study. At first contact, the purpose of the study was explained to each eligible subject who, if willing to participate, then gave informed consent. A standard questionnaire was completed, followed by a physical examination during which the fundal height, weight, height, blood pressure and presence or absence of proteinuria were noted in a data collecting form which was subsequently attached to the antenatal folder. All blood pressures were measured using three standard sphygmomanometers. Two of them, each with a cuff dimension of 35cm x 13cm, were used for normal or lean arms while the third, with a cuff dimension of 42cm x 13cm, was used for obese arms. The three sphygmomanometers were standardised. The blood pressures were measured in accordance with the recommendations of the British Hypertension Society8 and the American Heart Association.9 After the subject had rested for 5 minutes, the procedure for blood pressure measurement was explained to her. Then while sitting comfortably with her left arm extended on a table, the cuff was wrapped around her exposed arm in such a way that the tubing leading from the cuff to the manometer aligned with the brachial artery. While palpating for the radial pulse with the fingers of one hand, the other hand was used to pump up the bladder until the radial pulse disappeared. With the earpieces of the stethoscope in the observer's ears, the diaphragm part was then placed lightly on the antecubital fossa of the subject's extended arm. The valve of the sphygmomanometer was then released gradually while the observer listened for the Korotkoff sounds. The first phase of the Korotkoff sounds was recorded as the systolic blood pressure while the fifth phase was taken as the diastolic endpoint, both measurements being recorded to the nearest 2mmHg. In all subjects, the blood pressure was measured twice per session and the mean obtained. During labour, the blood pressure was measured two-hourly between contractions. During puerperium, the blood pressure was measured on two occasions daily. During antepartum and six weeks postpartum visits, the measurements were undertaken in a side room adjacent to the doctors' consulting room. In the immediate puerperium, the blood pressures were recorded in the wards. Midstream urine samples were analysed for proteinuria using Albustix strips. Proteinuria was defined on the basis of at least two clean-catch midstream specimens of urine (more than 4 hours apart) with 300mg/l or more of protein on reagent strip. Urine analysis was performed during each antenatal visit, on admission into the labour ward, each time the subject voided during labour, once daily in the immediate puerperium, and finally at the 6 weeks postnatal visit. Gestational age was estimated from the first day of the last menstrual period. In subjects with uncertain dates or in whom the uterine size was incompatible with the dates given, the gestational age was estimated ultrasonically in the second trimester. The heights of all the subjects were measured to the nearest 0.5cm using a standard ruler. One weighing scale was used to measure the weights of all subjects to the nearest 0.5kg. After delivery, the birth weight, birth length, Apgar score, mode of delivery, and maternal and fetal outcome were recorded. The relevant variables were measured finally during the postnatal visit and entered into the data form, which was then detached from the subject's folder. Data Analysis Only subjects who made at least four clinic attendances, whose pregnancies reached term, and who delivered within the hospital were included in the data analysis. The Quetelet index (QI) was calculated from the formula: QI = weight (kg)/height (m)2. QI is a measure of weight adjusted for height and is an objective measure of body adiposity.10 The infant's ponderal index (PI) was calculated from the formula: PI = weight (kg)/length (m)3. It is a valid indicator of nutritional status at birth and is predictive of poor neonatal outcome.11 The blood pressure trends in the study population were first determined. A problem that was noted in previous studies12,13 is that the pregnant patients' visits usually varied not only in number but also in timing. As in those studies, both these variations were eliminated by sub-dividing the period of pregnancy as follows: 15 weeks and below, 16–20 weeks, 21–28 weeks, 29–34 weeks, 35–38 weeks, greater than 38 weeks, intrapartum, immediate postpartum, one hour postpartum, first day postpartum, second day postpartum, and six weeks postpartum. All readings of a variable falling within a given period were pooled and averaged. The averaged systolic and diastolic blood pressures, each with the +2SD, for the various periods were used to illustrate the blood pressure changes in pregnancy. The lowest blood pressures were recorded in the 16–20 weeks period. To determine whether the absolute or relative rise in blood pressure during pregnancy was prognostically better in the study population, the subjects were categorised as follows: Group A: Subjects with a relative diastolic blood pressure (DBP) rise from the averaged 16–20 weeks readings until delivery < 15mmHg and absolute DBP < 90mmHg. Group B: Subjects with a relative DBP rise > 15mm Hg and absolute DBP <90mmHg. Group C: Subjects with absolute DBP > 90mm Hg irrespective of the relative rise in blood pressure. Using chi-square test for categorical variables and One Way ANOVA for continuous variables, outcome variables were compared for the three groups at 95% confidence level with the statistical package SPSS for Windows. For continuous variables, significant differences between group means were further characterised by a post-hoc analysis using the Scheffe test. The variables compared were incidence of proteinuria, eclampsia, caesarean section, maternal and perinatal mortality, birth length, birth weight, ponderal index, gestational age at birth, incidence of asphyxia and low birth weight. Similar comparisons of the outcome variables were made when the patients were grouped on the basis of systolic blood pressure into: Group A: Absolute systolic blood pressure (SBP) < 140mmHg and relative systolic blood pressure (SBP) rise from the averaged 16–20 weeks readings until delivery < 30mm Hg. Group B: Absolute SBP < 140mmHg and relative SBP rise > 30mmHg. Group C: Absolute SBP > 140mmHg irrespective of the relative rise in SBP. RESULTS Of the 560 eligible subjects, 45 women declined to participate while 515 women were enrolled in the study. Four hundred and seventy eight out of the 515 enrolled women completed the study. The dropout rate of approximately 7% represented those who made less than four clinic attendances, did not deliver in our hospital, or delivered preterm. Table 1 shows the physical characteristics of the subjects grouped as stated above. Table 2 shows the blood pressure trends during pregnancy in the study population. It shows that maternal blood pressures fell during pregnancy, being lowest at between 16 and 20 weeks of gestation, and then rose as term approached. From the 16–20 weeks period until term, the average systolic and diastolic blood pressures rose by approximately 4mmHg and 5mmHg respectively. However, from the last clinic visit at term to the immediate postpartum period, the relative rise in the average systolic and diastolic blood pressures was more rapid (20mmHg and 14mmHg respectively). A blood pressure of 140mmHg corresponded approximately to the mean + 2.5SD of the systolic blood pressures of the subjects at 38 weeks gestation and above. A diastolic blood pressure of 90mmHg corresponded approximately to the mean + 2SD of the diastolic blood pressures of the subjects at 6 weeks postpartum. Table 3 shows the maternal and fetal outcome for the three groups of subjects. Since all subjects in groups A and B had absolute DBP < 90mmHg throughout pregnancy, it was expected that if only the relative rise in blood pressure was all that mattered, then those with a relative DBP rise of 15mmHg or more (Group B) would have worse maternal and fetal outcomes than those with smaller relative rise in DBP (Group A). The results of chi-square test for groups A and B only and of post-hoc analysis for significant differences between group means differed from this expectation. Groups A and B did not differ significantly in all the maternal and fetal outcome measures (p > 0.05). The one maternal death in group A and the two in group B were due to haemorrhage. The data suggest that irrespective of the relative rise in diastolic blood pressure above the mid-pregnancy values, maternal and fetal outcome is unlikely to be affected as long as the absolute DBP does not reach 90mmHg. Chi-square test for groups A and B only and post-hoc analysis (Scheffe test) showed that groups A and B did not differ significantly in all the maternal and fetal outcome measures (p > 0.05). Similar tests for groups B and C only showed that women in group C had a significantly higher incidence of proteinuria, higher perinatal mortality rate, higher proportion of low birth weight babies and lower mean birth length than those in Group B (p < 0.05 for each variable). Group C has significantly higher incidences of caesarean section and proteinuria but lower mean birth weight and gestational age at delivery than group A (p < 0.05 for each variable). The effect of the absolute DBP was further explored by comparing the maternal and fetal results for the group of women with relative DBP rise consistently < 15mmHg but whose absolute DBP throughout pregnancy was < 90mmHg (Group B) with the results for the group of women whose DBP was consistently > 90mmHg anytime from mid-pregnancy until delivery at term (Group C). By current definitions, both of these groups are considered hypertensive and should have statistically similar feto-maternal results. However, if the absolute DBP of 90mmHg was more important in predicting feto-maternal outcome than a relative rise in DBP of > 15mmHg not reaching this absolute level, one would expect the subjects in group C to have worse results than those in group B. Chi-square test for groups B and C only and post-hoc analysis for significant differences between group means confirmed this expectation. Women in group C had significantly higher incidence of proteinuria, higher perinatal mortality rate, higher proportion of low birth weight babies and lower mean birth length than those in Group B (p < 0.05 for each variable). Although there was no statistically significant difference between the two groups in the remaining seven variables assessed, two of these deserve further comments. The two maternal deaths in group B were due to haemorrhage while the three maternal deaths in group C were due to pre-eclampsia. Although no case of eclampsia was recorded in any of the women whose DBP remained below 90mmHg, two eclamptic cases were recorded in those with DBP < 90mmHg. The results of the systolic blood pressure groups were similar to those of the DBP groups, the maternal and fetal outcome being again worse in the women with absolute systolic blood pressure > 140mmHg. The details of the maternal deaths were as follows: Group A: The only maternal death in this group occurred in a 34-year-old gravida 7, para 6+0 woman. She developed spontaneous intrapartum uterine rupture and died within 30 minutes of the incident before blood and other arrangements could be completed for operating on her. Group B: Two deaths occurred in this group. The first was in a gravida 3, para 2+0, who had caesarean section for placenta praevia. Three hours postoperatively, she developed disseminated intravascular coagulation. Fresh blood, fresh frozen plasma and cryoprecipitate were not available in the hospital on the day of the incident. The patient died six hours later after receiving six units of banked blood. The second maternal death in group B was in a gravida 6, para 5+0 woman. She too had placenta praevia. At caesarean section, uncontrollable haemorrhage was encountered resulting in total hysterectomy. Five units of blood were all that could be procured and transfused before the patient died three hours postoperatively in the intensive care unit. Group C: Three maternal deaths occurred in this group. The first was a 33-year-old gravida 5, para 4+0 woman, who had induction of labour for severe pre-eclampsia. There was delay in the second stage of labour and failed vacuum extraction. Caesarean section was performed for this indication. She developed acute renal failure postoperatively. Dialysis could not be performed on her because the only available dialysis machine in the hospital then was out of order. She died on the 4th postoperative day. The second maternal death was in a 27-year-old gravida 2, para 1+0 nurse. She had caesarean section for severe pre-eclampsia. Following extubation, she developed laryngeal spasm from which she later died. The third maternal death was in a 29-year-old unbooked primigravid eclamptic, who was admitted after fitting five times at home. On admission, her Glasgow coma score was 4. She had an emergency caesarean section. Postoperatively, she remained unconscious and died 5 hours later. With regard to perinatal deaths, there were five stillbirths and one early neonatal death in group A, giving a perinatal mortality rate of 69 per 1000. The five stillbirths were due to asphyxia from intrapartum uterine rupture (1 baby), placental abruption (2 babies) and undetermined cause (2 babies). The one early neonatal death was due to birth asphyxia from difficult labour. In Group B, there were 6 stillbirths and 2 early neonatal deaths, giving a perinatal mortality rate of 34 per 1000. The causes of the stillbirths were intrauterine growth restriction (2 babies), congenital malformations (2 babies), asphyxia from ruptured uterus (1 baby), and undetermined cause (1 baby). The causes of the two early neonatal deaths in this group were neonatal sepsis (1 baby) and neonatal jaundice (one baby). In Group C, there were 10 stillbirths and 5 early neonatal deaths. The stillbirths were due to congenital malformation (2 babies), hypertensive disorders (6 babies) and febrile illness (? malaria) in pregnancy. The 5 early neonatal deaths were due to intrauterine growth restriction (4 babies) and neonatal jaundice (1 baby). No post-mortem examination was carried out on these babies, as their parents refused to give consent for the procedure. DISCUSSION The above data, which suggest that the absolute blood pressure of 140/90mmHg is a better predictor of feto-maternal outcome than is a relative rise in the systolic/diastolic blood pressure, are in agreement with a previous Caucasian study.4 Furthermore, data from Table 2 suggest that a mean rise from mid-pregnancy of 24mmHg and 19mmHg in the systolic and diastolic arterial pressures respectively may be physiological in the population studied as long as the absolute blood pressure does not reach 140/90mmHg. Again, since the lowest mean diastolic blood pressure recorded during pregnancy was approximately 64mmHg, it means that a relative rise in diastolic blood pressure of at least 26mmHg may be necessary in some subjects before a diagnosis of hypertension (defined as DBP > 90 mmHg) can be made. The above observations support the definition of pre-eclampsia first advocated by Redman and Jefferies14 and later validated by other workers,15 based on blood pressure criteria alone. They reported that the combination of (i) a first antenatal visit diastolic pressure below 90mmHg (ii) a subsequent increase of at least 25mmHg during pregnancy and (iii) a maximum reading of at least 90mmHg selects a group of women with the characteristics of pre-eclampsia. Among the group of women meeting these criteria, there was a higher proportion of primigravidae, more proteinuria, lower birth weight and increased perinatal mortality.14 Tables 3 shows that diagnosing hypertension as a relative diastolic blood pressure rise of 15mmHg without reference to the absolute diastolic blood pressure level will include some 48% of subjects whose pregnancies will have normal outcome. This is not desirable. Although Villar et al6 presented evidence that women with a relative blood pressure rise > 30/15mmHg during pregnancy have a higher risk of developing absolute blood pressure > 140/90mmHg than those with a relative blood pressure < 30/15mmHg. A relative blood pressure rise > 30/15mmHg ought to be an indication for increased surveillance, the diagnosis of hypertension only being made when an absolute blood pressure of 140/90mmHg is reached. Further studies of other Nigerian populations need to be done to determine if the current practice of diagnosing pre-eclampsia on the basis of a relative blood pressure rise of 30/15mmHg in the pregnant Nigerian should be abandoned. The decision to use the fifth phase of the Korotkoff sounds (K5) as the diastolic endpoint in this study deserves a comment. During the initial two weeks training of participants in this study, it was noted that inter-observer error was less with the fifth phase than the fourth phase as the diastolic endpoint, hence the decision to use the former. This smaller inter-observer error has also been observed by other workers7,14 and so justifies the use of K5 in this study. This study suffers from several limitations. Because of the strict eligibility criteria, many antenatal subjects were excluded from the study. These included women who booked after 16 weeks of gestation, those who delivered preterm and others to whom the findings in the present study might not apply. Although efforts were made to minimise inter-observer and systematic errors in blood pressure and other measurements by standardisation, the number of observers and observations might have militated against these efforts. Furthermore, the varying circumstances of the observations might have added to the difficulty in minimising errors. For example, the noisy labour ward environment obviously differed from the situation in the antenatal clinics. The extent to which this affected the blood pressure measured in the former is difficult to determine. Preventing contamination of urine specimens by vaginal discharge, liquor and lochia might not have been possible on all the occasions during which urine samples were collected and tested. Additionally, the dipstick method of testing for proteinuria has its limitations. Since total protein estimation or urine cultures were not carried out on all patients with positive dipstick tests, the conclusions drawn from some of the findings must be accepted with caution. Apart from proteinuria, the other outcome variables might also have been affected by several obstetric conditions including intrapartum care, which could not be controlled for. Finally, any analysis of blood pressure dynamics during pregnancy must take into account the gestational age at initial measurement, the gestational age at final measurement, the interval over which any rise occurs and the absolute level reached. In the present study, the gestational age at initial measurement (< 16 weeks) was similar for all subjects. Although the gestational age at final measurement (37+ weeks) was also similar for all subjects, whether to use the highest blood pressure before or during labour was a difficult decision. The latter option was chosen because of the rather small rise in the systolic/diastolic blood pressure (5/4mmHg) before labour (Table 2), the rapid rise in blood pressure intrapartum (Table 2), and the documented high incidence of intrapartum hypertension in our population.17 This choice has its limitations. Women with preterm births were excluded from the study because their inclusion would have made it difficult to control for gestational age at final blood pressure measurement. In some subjects, the highest blood pressure might only have been transient and might not have affected any of the outcome variables measured. The interval over which any blood pressure rise occurred could not be controlled for, but since most rapid rises occurred intrapartum it was unlikely that this had any significant effect. With respect to the absolute level of blood pressure reached, a simple classification based on the current definitions of hypertension was used. Such a simple classification may provoke some controversy, as some would prefer a multivariate modelling approach. A more extensive study using such an approach is currently in progress. A worrisome aspect of this study is the high maternal mortality ratio (MMR) of 1255 per 100,000. This figure is even lower than the 1406 per 100,000 recorded in a previous study of the worsening MMR in our hospital over the previous decade.18 The major factors responsible for the high MMR include institutional delays, non-availability of materials, and decayed infrastructure, amongst others consequent upon a depressed economy.18 In the meantime and subject to the above limitations, it is concluded that the absolute blood pressure of 140/90mmHg is a better predictor of feto-maternal outcome than is a relative blood pressure rise from mid pregnancy, which does not reach this level. Therefore, diagnosing hypertension based on a relative blood pressure rise of 30/15mmHg alone in Nigerian pregnant women needs to be reviewed. ACKNOWLEDGEMENTS The author is grateful to his hospital for funding the study and to the following persons who helped with data collection: Drs F. Ezugwu, I. Okafor, and M. Chikani; Mrs. A. Obionu (a matron); Mrs. C. N. Okafor and Mrs. R. Okafor (both nursing sisters); Miss R.U. Chime and Miss C.O. Alichie (both staff nurses/midwives). REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02007t3.jpg] [rh02007t2.jpg] [rh02007t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}