 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 1, April, 2002 pp. 41-49 The Nature of Puerperal Psychosis at Muhimbili National Hospital: Its Physical Co-Morbidity, Associated Main Obstetric and Social Factors Noah K Ndosi1 and MLW Mtawali2 1Department of Psychiatry,
MUCHS, P. O. Box 65051, Dar es Salaam, Tanzania. 2Department of
Obstetrics
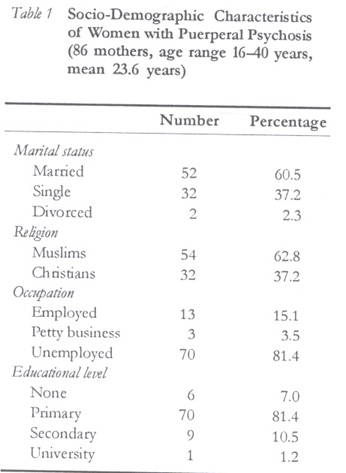
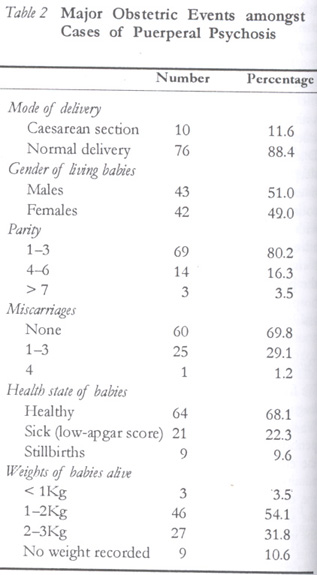
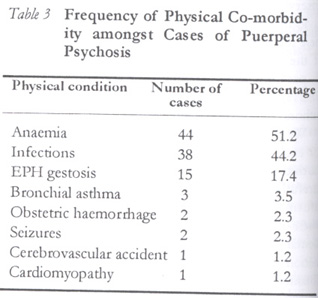
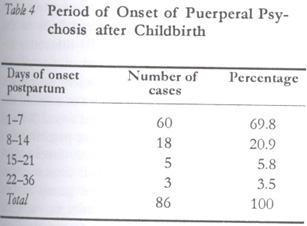
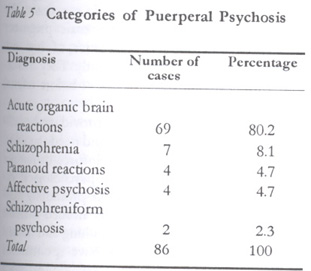
and Gynaecology, MUCHS, P. O. Box 65051, Dar es Salaam, Tanzania. Code Number: rh02008 ABSTRACT Eighty six in-patients suffering from puerperal psychosis within six weeks after childbirth were prospectively investigated in Muhimbili National Hospital during two years. Formal psychiatric history, mental status evaluation, research and diagnostic criteria including ICD 10 and clinical progression were employed for diagnosis. Using a structured questionnaire, the socio-demographic characteristics, concomitant physical disorders, major obstetric events, period of onset of puerperal psychosis following delivery and social support given were established. Mean age was found to be 23.6 years; the majority was primiparous women with parity of between one and three children. Main physical co-morbidities included anaemia in 51.4% of cases, infections in 44.2% and EPH-gestosis in 17.4%. Most mothers received social support from their extended families. Organic psychosis was found in four fifths of the mothers and schizophrenia in 8.1%. A high rate of early onset puerperal psychosis (3.2/1000 births), predominantly in young primiparous women, was found. (Afr J Reprod Health 2002; 6[1]: 41–49) RÉSUMÉ La Nature de la Psychose Puepérale à l'Hôpital National de Muhumbili: Co-morbidité, Obstétrique Principale et Facteurs Sociaux. Quatre-vingts malades hospitalisés atteints de la psychose puerpérale six semaines après l'accouchement ont été enquêtées à l'Hôpital National de Muhimbili pendant deux ans. Pour le diagnostic, on s'est servi de l'histoire psychiatrique formelle, l'évaluation de l'état mental, les critères de la recherche et du diagnostic y compris ICD 10 ainsi que la progression clinique. Nous avons établi les caractéristiques socio-démographiques, les désordres physiques concomitants, les principaux évenements obstétriques, le début de la psychose puerpérale après l'accouchement ainsi que le soutien social donné à l'aide d'un questionnaire structuré. L'âge moyen était 23,6 ans; la plupart des femmes étaient des primpares ayant une parité d'entre un et trois enfants. Les principales co-morbidités physiques comprennent l'anémie chez 51,4% des cas, les infections chez 44,2% et la gestose-EPH chez 17,4%. La plupart des mères ont reçu le soutien social de la part de leurs familles étendues. On a découvert que 4/5 souffraient de la psychose organique et que 8,1% étaient atteintes de la schizophrénie. On a découvert également qu'il y a un taux élevé du commencement de la psychose puerpérale (3,2/1000 naissances) surtout chez les jeunes femmes primpares. (Rev Afr Santé Reprod 2002; 6[1]: 41–49) KEY WORDS : The nature of puerperal psychosis Muhimbili National Hospital INTRODUCTION Recent studies indicate that 85% of women develop some form of postpartum mental illness1 and up to half of parous women with manic depression develop an episode of severe psychiatric disturbance within a few days after giving birth.2 The relative risk for puerperal psychotic illness has been found to be 29% in subsequent pregnancies especially after an affective episode in the first 30 days after delivery.3,4 Postpartum psychosis is not a unitary clinical entity, and psychiatrists also disagree on the time interval after birth varying from six weeks to one year.5,6 Epidemiological studies conducted in USA and Great Britain using research diagnostic criteria for psychosis and depression have defined the postpartum period occurring from two weeks to one year following birth and the peak incidence is within the first three months.7,8 However, the 10th international classification of mental and behavioural disorders considers puerperal psychosis as personality disintegration and loss of contact with reality occurring within six weeks after childbirth.9 The clinical picture may take the form of an affective psychosis, manic or depressive disorder, or schizophrenic or schizo-affective type. The incidence of puerperal psychoses in USA and Great Britain has been estimated to be low (about 1 to 2 per 1000 births).10-12 In many developing countries, only few studies have been carried out on this problem and the incidence is not known. Postpartum psychoses are believed to result from stress undergone during pregnancy and the period of about six weeks post-delivery. The causes include a precipitous reduction in the brain oestrogen environment,13,14 alterations in body image, which activate unconscious psychological conflicts pertaining to pregnancy and the intrapsychic reorganisation of becoming a mother. Women with previous episodes of puerperal psychosis or manic-depressive illness have a hundred fold high rate of puerperal psychosis (one in five) and it has been further revealed that in the first post-delivery month, a woman is twenty two times more likely to be admitted with psychosis than a non-pregnant woman of childbearing age.8,12 Other reported factors that are associated with puerperal psychosis include primiparity, antenatal complications, marital instability, and lack of social support. Caesarean sections, perinatal death, a female baby, and if the family has had a history of mood disorder are additional factors.15 A prior episode of postpartum psychosis increases the risk of a second attack from one in fifty to one in seven or even less. Existing observations on the rate of occurrence of psychiatric problems affecting women are based on few institutional statistics and not on the community. Complications of pregnancies and puerperal psychoses pose a disproportionate burden to females in sub-Saharan Africa, and the majority of women who suffer from this morbidity often remain at home with their families under the care of traditional healers.16 Since a worrying number of mothers who suffer from this severe mental illness are not identified, they remain vulnerable to greater maternal mortality. There are hardly any studies that report on the nature and magnitude of mental problems among Tanzanian women, and the incidence of puerperal psychosis is unknown. This clinical study investigates women who had a first episode within six months after parturition so as to contribute to greater understanding of some of the health problems that afflict mothers after parturition. METHODOLOGY This is a prospective clinical study conducted at Muhimbili National Hospital on mothers suffering from a first episode of puerperal psychosis. It investigates the categories of puerperal psychosis, associated socio-demographic characteristics, major obstetric events, concomitant physical disorders, health status of born babies and social support given to the mothers and the duration of onset of puerperal psychosis. The Maternity Wards Muhimbili National Hospital, the largest referral hospital in Tanzania, is the main university teaching hospital that provides health services to an estimated three million residents in Dar es Salaam region. The obstetric and gynaecological department, which has three wards, is one of eighteen departments of the hospital. Each ward is supervised by a senior obstetrician, supported by a junior specialist, a resident, and a team of nurses and midwives under a nursing officer. The maternity wards have 247 beds. On average, 55 expectant mothers are admitted there daily. The percentage of bed occupancy is 81% and the average duration of hospital stay is four days. The majority of complicated obstetric cases referred to Muhimbili hospital come from three district hospitals of the city and other health centres within the region. Often, the cases demand prompt assessment and treatment on an emergency basis. Due to congestion in the wards, many patients sleep on the floor. Both mothers and infants are at times predisposed to infections. The high parity countrywide, a heavy burden of expectant mothers with complications, physical health problems, inadequate specialists and obstetrical facilities are some of the reasons that significantly contribute to the prevailing burdensome referrals to Muhimbili hospital, which is near and easily accessible to city residents by road. Patients and Materials We first explained the purpose of our study to colleagues and nurses working in the labour wards. We then solicited their cooperation throughout the period of study. From the beginning of 1996 to the end of 1998, 34,620 expectant mothers were admitted to the Muhimbili maternity wards. After the daily ward rounds, the attending doctors and the supervising nurses of each ward reported to the investigators any conspicuous abnormal behaviour of each mother after delivery. One hundred and ten of all consecutive admissions (0.32%) were observed to have displayed notable abnormal behaviour. After explaining to the individual patients, their relatives, spouses and caretakers the purpose of the study, we obtained their informed consent to participate in the study. Only 86 of them (78.2%) consented and cooperated reliably with the authors till the end of the study. We conducted a thorough physical examination for each patient to establish and record any co-morbidity. Clinical notes of each case were then carefully studied by the authors and additional information sought from the attendant doctors when necessary. A formal psychiatric history, mental status evaluation and corroborative information from relevant sources for each subject were obtained. A working diagnosis was made before treatment with psychotropic medication was started. After each subject had acquired reliable insight into the prevailing hospital situation, a structured questionnaire, which contained socio-demographic details (age, religion, occupation, marital status, duration of marriage, and educational level), major obstetric events concerning mode of delivery, gender of baby, body weight and health status of each baby, number of pregnancies, parity, and miscarriages was completed. The duration of onset of clinical symptoms and signs after childbirth in each case were noted. The clinical presenting features were closely studied in cross-sections and longitudinally and they were counter-matched to the research diagnostic criteria for schizophrenia and affective disorders by Endicott and Spitzer17 and the 10th international classification of mental and behavioural disorders9 for a final diagnosis at discharge. Those patients who had not recovered at discharge from the maternity wards were transferred to the psychiatric unit where they continued with treatment. They were then followed up as outpatients at intervals of two, four, and twelve weeks and six months following discharge. RESULTS Socio-Demographic Characteristics As shown in Table 1, 52 (60.5%) women were married, 32 (37.2%) single and 2 (2.3%) had divorced. Fifty four subjects (62.8%) were Muslims, while 32 (37.2%) were Christians. Seventy (81.4%) probands were unemployed, 13 (15.1%) were employed, and 3 (3.5%) engaged in petty business. Six (7%) mothers had not attended school at all, 70 (81.4%) had primary education, 9 (10.5%) had attained secondary level and 1 (1.2%) was a university graduate. From Table 2, seventy six mothers (88.4%) had normal deliveries and 10 (11.6%) underwent lower segment caesarean sections. Sixty nine (80.2%) mothers, of which 40 (46.5%) were primiparous had parity of between 1 and 3 children, 14 (16.3%) had between 4 and 6 children, while 3 (3.5%) had seven and above. Sixty subjects (70%) had not lost any babies, 25 (29.1%) reported between 1 and three miscarriages, and only one (1.2%) had four miscarriages. Of the 85 live babies, 43 (51%) were males while 42 (49%) were females. There were four twin pairs (9.4%) of all living babies. Sixty four babies (68.1%) were healthy, 21 (22.3%) were sick with low apgar score, of whom 6 (7.1%) died within two weeks after birth. There were nine (9.6%) stillbirths. Of the living babies, three (3.5%) weighed less than 1kg, 46 (54.1%) weighed between 1 and 2kg, 27 (31.8%) weighed between 2 and 3kg, and no weights were recorded for 9 (10.6%) of the live babies. According to Table 3, of the 86 mothers, 44 (51.2%) were anaemic, 38 (44.2%) suffered from various infections, which included malaria (22), sepsis (4), human immunodeficiency virus (3), diarrhoea (3), dermatitis (3), tuberculosis (2) and otitis media (1). Fifteen women (17.5%) had EPH gestosis, 3 (3.5%) had bronchial asthma, 2 (2.3%) obstetric haemorrhage, 2 (2.3%) seizures, 1 (1.2%) cerebrovascular accident, and 1 (1.2%) cardiomyo-pathy. Social Support The mothers needed psychological support after childbirth, including food, clothing and money to buy medicines. Of the 78 fathers (90.7%) who accepted their babies, sixty three (73.3%) supported their partners satisfactorily but five (5.8%) did not give any assistance. In 18 (20.9%) cases fatherhood was denied; the fathers did not support the mothers and babies. Twenty four subjects (27.9%) received support from both parents, whereas 22 (25.6%) were supported by their fathers alone, and 10 (11.6%) by their mothers only. Seventy nine subjects (91.9%) were supported by their relatives while 7 (8.1%) had no support at all. Table 4 shows that sixty mothers (69.8%) developed psychosis within one week after delivery, 18 (20.9%) within a fortnight, 5 (5.8%) within three weeks, and 3 (3.5%) within six weeks postpartum. Table 5 shows that sixty nine mothers (80.2%) suffered from acute organic brain reactions, 7 (8.1%) schizophrenia, 4 (4.7%) had paranoid reactions, 4 (4.7%) affective psychosis, 2 (2.3%) had schizophreniform psychosis. Seventy six subjects (88.4%) were in their first psychotic episode while 9 (10.5%) had a previous non-puerperal psychotic episode, and one mother (1.2%) had experienced two episodes unrelated to childbirth. Only five patients (5.8%) had a history of psychotic illness in their families. DISCUSSION Puerperal disorders demand prompt attention in order to avoid any adverse outcome for both mother and infant. Puerperal psychosis is the most severe and most dramatic among all postpartum psychiatric disorders12 and it was one of the causes of mortality amongst admitted mental patients at Muhimbli hospital.18 The prevalence of puerperal psychosis in this study was 3.2 per 1000 births, which is at least twice the incidence reported in studies from Great Britain and America.2,8,19 However, Turkson in Ghana20 found a higher prevalence of 6 per 1000 births. The incidence of puerperal psychosis in Dar es Salaam could even be higher since this study investigated cases referred to one hospital within six weeks after parturition. Had the study covered the formal six months or a whole year, the prevalence would have most likely been higher. Moreover, a considerable proportion of Tanzanians suffering from psychological problems does not seek treatment in hospital but seek help from traditional healers at.21 Furthermore, expectant mothers who deliver at Muhimbili Hospital are mostly emergency cases with high physical co-morbidity. Mothers' average age of 23.6 years is low because in recent years Tanzania has had a higher prevalence of teenage pregnancies.22 Young expectant mothers have a higher educational level and they seek help in hospital more readily when compared to older women with lower education who often seek help from traditional birth attendants. However, only 11.7% of the cases in this study had secondary education and above. The greater part of Tanzanian population lives in poverty and 51.1% belong to soft-core poverty, while 35.9% belong to hard-core poverty.23 As shown in Table 1, 81.4% of the mothers were unemployed and 37.2% single. The majority of these mothers were poor and lived in overcrowded urban areas without adequate sanitation and clean water. Most disorders have their highest prevalence among the poor and disadvantaged.24 Ten mothers (11.6%) had caesarean section. Muhimbili, being a teaching hospital, receives an increased proportion of high-risk cases, some of which need operation to avert perinatal and maternal mortality. The rate of these operations in this study is in line with the recommended 10%.25 Of the 69 mothers who had a parity of between one and three children, 40 (58%) were primiparous. Ifabumuyi, in a Nigerian study of mothers of corresponding age with puerperal psychosis, found 66% to be primiparous.26 Young primigravida are most probably ill-prepared psychologically to cope with motherhood together with stress of marriage system. Significant stress factors in the genesis of puerperal psychosis among Tanzanian mothers was also reported by Swift thirty years ago.27 Nearly one third of the cases had miscarried and one tenth had stillbirths. Intrauterine fetal death is a devastating condition in pregnant women, which usually causes psychological stress and anxiety of carrying a dead fetus in-utero.28 Miscarriages of pregnancies are often related to complications that cause morbidity and mortality amongst women of childbearing age. The high rate of abortions amongst mothers suffering from puerperal psychosis suggests consequent complications of increased psychological morbidity among the mothers. The association of development of psychosis with poor outcome of babies has not been successfully established. However, while a recent study of black women in South Africa has identified intensive medical care or death of the baby as a risk factor for puerperal psychosis,29 perinatal death has also been reported to be associated with an increased risk of psychological stress contributing to high psychiatric morbidity in India.30 Physical illness may be a direct cause of psychiatric illness and it can act indirectly as a non-specific precipitant of mental illness.31 Physical morbidity and psychiatric disturbances during puerperium have profound long-term implications not only for the wellbeing of the mother but also for her relationship with family members and the development of the child.32 Anaemia in pregnancy is associated with about 60% of maternal deaths in developing countries and it is a leading cause of maternal deaths at Muhimbili hospital.33 It is noteworthy that more than half of the mothers in this study suffered from anaemia (Table 3). Psychosis in anaemic women has been reported by Meyer and Salaam.34,35 Acute organic psychosis can also be caused by bacteria, viruses, parasites, including released toxins, high fever and electrolyte imbalance.36 One quarter of the patients suffered from infections, of which Falciparum malaria accounted for most of the malarial cases. Cytoadherence and endothelial damage are important factors believed to account for the pathogenesis of cerebral malaria, which can present with psychotic features.37 Current data in the Muhimbili maternity wards indicate the prevalence of HIV among pregnant women to be about 13.7%.38 Only 3.6% of the subjects were found to have HIV infections because no screening was undertaken for all the women. This investigation was solely undertaken to find out the causes of infections in some of the probands. A recent study by Susser found 3.8% of patients with HIV infection to have psychotic features. HIV infections may have both direct and indirect effects on the aetiology and clinical course of puerperal psychosis.39 Cerebral anoxia due to respiratory impairment, haemorrhages, seizures and cardiac failure are known to frequently cause acute mental dysfunctions. When these physical disorders are severe and persistent psychotic symptoms may present for long durations. Approximately 4% of pregnant women develop toxic symptoms from pregnancy and it is associated with significant maternal and fetal morbidity and mortality.40 Severe EPH gestosis can cause hypertensive encephalopathy with organic psychosis. The high number of mothers with toxic pregnancy (17.4%) in this study is suggestive of high-risk primiparous mothers predominantly. They had received poor antenatal management before referral to Muhimbili hospital. A support system is a group providing the individual with physical, emotional and needy supplies. Supporting individual buffers reinforce or nurture the recipient by mobilising his psychological capacities and inner resources while promoting mastery.41 After childbirth, mothers needed material supplies in the form of food, clothing and money. Many Tanzanian communities have spontaneous support systems frequently based on extended families as evidenced by social and material support rendered to over 90% of the mothers by their extended families. However, one fifth of the mothers had inadequate support after fatherhood was denied, while seven mothers were despondent without any support. The majority of these subjects were not only poor but also displaced in an overcrowded urban setting with deprivations of various amenities of life. These mothers were vulnerable to the stressful life events and lack of social support, which have variously been reported to predispose individuals to mental illnesses.42,43 The period of onset of puerperal psychosis varies. At least 90% of the cases developed puerperal psychosis within two weeks. The majority of 192 cases in an Indian study also developed puerperal psychosis within two weeks.44 A British study of 100 consecutive admissions found that 56 of mothers with puerperal psychosis were admitted within two weeks of onset of psychotic illness.45 In this study, concomitant organic factors could have given an impact, which contributed to the early onset of the puerperal psychosis. By using control cohorts of women of corresponding ages, further research is needed to determine the extent of risk to contract puerperal psychosis when various physical disorders are involved. There are no unitary views regarding the aetiology and nosology of puerperal psychoses, and there are only few studies that relate to nosology of puerperal psychosis. While some authors consider them to be undifferentiated psychoses lacking evidence of nosological independence, others categorise them into psychotic depression, schizophrenia, schizophreniform psychosis and undifferentiated psychoses.4,30,43 Although no control cohort was used to determine risk factors from the accompanying physical disorders, the high frequencies of severe anaemia, infections, toxaemia of pregnancy, haemorrhages and other physical disorders, as indicated in Table 5, are likely to have had either direct or indirect impact, which with other factors probably triggered the psychotic illness. Consequently, in four fifths of the cases the psychotic illness had organic features of overriding delirium characterised by disturbances of consciousness and attention, incoherence of thinking, amnesia, disorientation, and insomnia. Other symptoms and signs included restlessness and fluctuating clinical conditions. Nearly one third to half of patients attending some urban hospitals in East Africa were found to suffer from organic brain syndromes and they recently accounted for 36.7% of mortality in the Muhimbili psychiatric ward over a five-year period.18,46,47 A study of postpartum psychosis among 250 consecutive mothers in The Netherlands found affective, schizoaffective and unspecified psychoses as the main categories.48 Schizophrenia was diagnosed in 8.1% of cases. The subjects experienced third person auditory hallucinations, psychomotor disturbances, self neglect and incoherent thinking with poor insight for a duration exceeding one month. Schizophrenia has been documented in previous studies and greater input of nursing care and service resources was required than in other diagnostic categories.44,49,50 Clinically, four patients presented with paranoid reactions, three were unmarried and two had stillbirths. They predominantly exhibited paranoid ideas towards the attendant nurses and relatives and believed that their meals had been poisoned by the caretakers. Puerperal depression has been considered to be probably the same illness as depression at other times.51 This affective disorder has been associated with increased likelihood of severe life events in the twelve months preceding illness.52 An unmarried, unemployed mother, together with a mother with a sick baby suffered from depressive psychosis. Two subjects presented with clinical mania. Up to half of parous females with bipolar disorders develop an episode of puerperal psychosis within a few days after giving birth.53 Only two patients suffered schizophreniform psychosis for a duration of less than four weeks. A Danish study of admitted mothers with a first episode of puerperal psychosis also found a minority to be suffering from schizophreniform psychosis.54 One tenth of the patients had a previous non-puerperal psychosis. An incidence either as high as 1:5 in women who have suffered a previous psychosis during childbirth or otherwise has been reported in Great Britain.55 Most clinical and genetic evidence suggests that puerperal psychosis is closely related to factors associated with genetic models.56 In conclusion, puerperal psychosis and concomitant physical disorders amongst young primiparous women contributes significantly to ill-health of women in puerperium. Anaemia, infections and toxaemia of pregnancy demand greater control. More research on female morbidity after childbirth is needed so as to understand the underlying causative factors and progression of the illnesses. Ways and means of reducing the extent of morbidity and mortality among these women are urgently needed. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02008t3.jpg] [rh02008t5.jpg] [rh02008t4.jpg] [rh02008t2.jpg] [rh02008t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}