 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 1, April, 2002 pp. 50-64 Analysis of Women's Reproductive Health Situation in Bida Emirate of Niger State, Nigeria Mohammed Kuta Yahaya1 1Lecturer in Development Communication, Department of Agricultural Extension and Rural Development, University of Ibadan, Ibadan, Nigeria. E-mail: mkyahaya@skannet.com Code Number: rh02009 ABSTRACT This study examined the reproductive health situation in Bida Emirate of Nigeria, with a view to advancing frontiers in communication support for reproductive health education. Multi-stage sampling technique was used to randomly select 1,200 women respondents that participated in the study. Data was obtained on reproductive health and rights, reproductive health history, and personal and social characteristics of respondents. Data analyses showed that majority (68.1%) of respondents were aware of existing methods of birth control, while 31.9% were not. On the use of methods, abstinence, breastfeeding and use of condoms recorded 42.8%, 22% and 40.3% respectively. Respondents rarely used traditional methods of birth control. Forty five per cent blamed their husbands for not using family planning methods. Surprisingly, 84.8% of respondents had no idea of what HIV/AIDS is all about; only 13% and 3.1% could describe gonorrhoea and AIDS respectively. Results further revealed that there is no significant relationship between personal and social characteristics of respondents (religion, marital status and position, etc) and their attitude towards family planning. However, rural and urban women significantly differed in their health status (t = 0.2729; p < 0.001). Similar trend was observed for attitude towards family decision-making (t = 40; p < 0.001), sexuality and STD prevention (t = 90; p < 0.001), and maternity/childcare (t = 0.001; p < 0.001). In conclusion, the study reveals that there is a wide gap between social expectations of women's reproductive health and cultural realities in Nupeland of Nigeria. The study thus recommends, among others, the need for sustainable safe motherhood campaign in culture bound societies. (Afr J Reprod Health 2002; 6[1]: 50–64) RÉSUMÉ Analyse de la Situation de la Santé Reproductive de la Femme dans l'émirat de Bida dans l'Etat de Niger, Nigéria. L'étude a examiné la situation de la santé reproductive dans l'émirat de Bida, au Nigéria afin de pouvoir avancer les frontières en ce qui concerne le soutien de la communication pour l'éducation de la santé reproductive. La technique d'échantillon à étapes multiples a été adoptée au hasard pour selectionner les 1200 femmes qui ont participé à l'étude. Nous avons recueilli les données sur la santé reproductive et les droits, l'histoire de la santé reproductive ainsi que sur les caractéristiques personnelles et sociales des participantes. Les analyses des données ont montré que la majorité (68,1%) des participantes étaient au courant des méthodes actuelles du contrôle des naissances, alors que 31,9% n'en étaient pas. En ce qui concerne l'emploi des méthodes, l'abstinence, l'allaitement maternel et l'emploi des préservatifs, nous avons obtenu les chiffres suivants 42,8%, 22% et 40,3% respectivement. Les participantes ont rarement employé les méthodes traditionnelles de contrôle des naissances. 45% ont reproché à leurs maris de ne pas employer les méthodes du planning familial. Chose étonnante, 84,8% n'avaient aucune idée de ce que c'est le VIH/SIDA; seules 13% et 3,1% étaient capables de décrire la blennorragie et le SIDA respectivement. Les résultats ont montré davantage qu'il n'y a pas de rapport remarquable entre les caractéristiques personnelles et sociales des participantes (religion, état civil et situation) et leur attitude envers le planning familial. Pourtant, il y a eu une différence marquée entre les femmes rurales et les citadines par rapport à leur situation médicale (t = 0,2729; p < 0,001). Nous avons observé la même attitude envers la prise de décision (t = 40; p < 0,001). En conclusion, l'étude a montré qu'il existe un écart entre les perspectives sociales de la santé reproductive de la femme et les réalités culturelles chez les Nupé du Nigéria. L'étude préconise donc, entre autres, la nécessité d'une campagne en faveur de la maternité protégée durable dans les sociétés fortement marquées par la culture. (Rev Afr Santé Reprod 2002; 6[1]: 50–64) KEY WORDS : Reproductive health, safe motherhood, maternal mortality and morbidity, family planning, HIV/AIDS INTRODUCTION A decade after safe motherhood initiative was launched, Nigeria is still battling to make tangible progress in curbing the ever-increasing cases of maternal mortality and morbidity. In Niger State, as obtained in several other states, safe motherhood has received little or no attention in the last decade. The importance of mothers in societal development cannot be over emphasised; not only are they sources of joy to the entire family, they are significantly priceless virtues in social construction. Several evidences of problems associated with the gap created in broken homes, and several instances where women have assumed leadership roles in many households have helped to change societal view of the worth of women. Reporting the submission of experts at the 5th International Congress of the Society of Gynaecology and Obstetrics of Nigeria (SOGON) held in Benin City in November 1998, a deplorable picture was presented to the entire world with shocking figures of rising death of pregnant women in Nigeria. This has no respect for region or state. For instance, from Sokoto to Enugu, Ibadan to Kano, Port Harcourt to Maiduguri, mortality rates are still very high and in some cases have risen from 200 to 600 per cent. For example, maternal mortality at the University of Nigeria Teaching Hospital (UNTH), Enugu, from 1991–1997 shows worrisome figures. For every 100,000 live deliveries 1,259 were lost! This is almost a five-fold increase from the 270 per 100,000 deliveries recorded between 1976 and 1985. From the University College Hospital (UCH), Ibadan, maternal mortality rose from 1,102 in 1988 to 2,360 in 1991, with a peak of 3,157 in 1994. The situation in Sokoto is equally worrisome; apart from abandoned vesico vagina fistula (VVF) victims in various hospitals, maternal mortality is over 2,138 per 100,000 live births. Similarly, at the Obafemi Awolowo University Teaching Hospital, reports show about 227 abortions per 100,000 deliveries, where 25.8% of maternal deaths were recorded between January 1987 and December 1996.1 Pre-Conception Care in Reproductive Health The primary pre-occupation of pre-conception care (PC) is to make sure that women are in the best possible physical and emotional health when they conceive. It has been observed in a comprehensive obstetrical and gynaecological survey that pre-conception care is viewed from who needs it, who wants it, and how should it be provided? Findings from a survey conducted on health professionals and women aged 16 to 48 years at nine general practices in London reveal that fewer than 40% of women view PC as essential and more than 10% gave it no importance. In striking contrast, about 85% of physicians and 95% of nurses agreed that PC could lower maternal and neonatal death and morbidity as well as enhance mothers' psychological well being. In general, health professionals and women of reproductive age are aware of PC, but recognition of its importance is far from universal. For this reason, targeted educational efforts might well prove helpful.2 According to a World Health Organization (WHO) report,3 every minute of everyday a woman dies of pregnancy-related complications. For every woman who dies, at least 30% develop chronic and debilitating problems. Further statistics reveal that every year, nearly 3.4 million newborn infants die within their first week of life. And for every newborn baby that dies another is still born. Several of these women and their babies die for the same reason - poor health and inadequate care during pregnancy and childbirth. The World Health Organization reports that 71 out of every 1000 births in Africa are stillbirths; hence, stillbirth and death in the first week of life remain high in developing countries. Stillbirth claims as high as 130 and 120 out of every 1000 births in Guinea and Somalia respectively. Meanwhile 25 out of 1000 births are recorded for countries like Algeria and Botswana, while Nigeria and Ghana looses 90 out of 1000 births.3 Both mothers and infants suffer the threat posed by the worsening health situation in developing countries. Severe bleeding accounts for 25% of maternal deaths while infection and abortion account for 15% and 13% of maternal deaths respectively. Unsafe abortion, a preventable cause of maternal death, is having a devastating effect on the lives of pregnant women across the globe, particularly in the developing countries. The situation is more pathetic in Africa and Asia where abortion accounted for 42–45% of maternal deaths in 1997. These facts reveal that abortion related deaths are numerous in the developing world. In countries where other causes of maternal deaths have been addressed and overall level of maternal mortality is low, they may account for a substantial proportion of total maternal deaths.3 Lifetime risk of maternal death, defined as the risk of an individual woman dying from pregnancy or childbirth during her lifetime, which is a function of the maternal mortality rate in a country, is another serious issue when discussing maternal health. According to the WHO, a lifetime risk of one in 3000 represents a low risk of dying from pregnancy and childbirth, while one in 100 is a high risk. None of the countries in Africa meets this standard. Awareness and Use of Contraceptives In Nigeria, like most African countries, childbirth outside marriage is not acceptable, hence, several studies have been initiated to investigate contraceptive use pattern among various categories of sexually active population. It is quite revealing that awareness of modern combined methods of contraception is popular with reference to intrauterine device, combined pills, injectables, progesterone, sterilisation and use of condom.4 This is similar to another study that investigated perception and practice of emergency contraception by post-secondary school students in southwest Nigeria. The study reports that the concept of contraception was known to 75.7% of the respondents although only 17.1% had accurate knowledge of fertile period and 43% did not know any method of emergency contraception. Also, 32.4%, 20.4% and 19.8% of the respondents were aware that combined pills, progesterone only, or intrauterine device could be used for emergency contraception. Further statistical analysis of the situation reveals that neither awareness of the concept of emergency contraception nor its past use was significantly influenced by age, education or religion of the respondents.5 Similarly, earlier reports show that knowledge of at least one method of contraception was reported by 97.7% of male respondents and 98.4% of female respondents in a study of sexuality and contraception among Nigerian youths and adolescents.6 Furthermore, less than half of the males knew any method other than the condom and oral contraceptive pills. In general, females had better knowledge of contraceptive methods. However, only 72% of males and 81% of females who were sexually experienced had ever used contraceptives. Reports from a study among 190 sexually active respondents show that the most popular contraceptive method used was the rhythm method (46.8%).6 However, the report further reveals that current use of contraception was independent of respondent's age, religion, parental level of education and age at sexual debut among contraceptive users. One challenging phenomenon in the reproductive health practice in Nigeria now is the sudden and ravaging consequences of HIV/AIDS and the threat it poses to human continued existence. Investigations carried out on sexual practice and experience by social and medical scientists have been stepped up in the past few years, although implementation of action plan on the prevention of the spread have been considerably lower than the internationally agreed strategies. In an effort to bring to limelight the reproductive health situation among youths and adolescents in Nigeria to justify the need for sustainable intervention mechanisms, several studies have been carried out. Findings show different behavioural patterns among youths. For instance, boys usually satisfy their sexual desires through sex with girlfriends, some with prostitutes, and others through occasional raping of girls.7 Other findings are consistent with earlier reports, though it is apparent that little or no variations exist between male and female perceptions of certain stereotypes that have implication for sexual partnership, sexual act and child sexual abuse.8 The sexual activities of older siblings (parents and older men) do not seem to help the worsening sexual practice among teenagers. A preponderance of sexually active respondents of older working men who are sexual partners of teenage secondary school girls has been sparsely reported by many findings across Nigeria. Early initiation of female adolescents to sex is mainly for financial benefit and harassment by older and married male sexual partners.8 Other factors reported to be responsible include peer influence, initiation by parents and older siblings, the impact of film or video scenes, the urge to experience sex and to feel like a “real man”. The Pregnancy-Related Mortality and Morbidity Situation According to critical analysis of the situation in Nigeria, the adequacy of the assessment of maternal mortality depends on available data. The three principal sources of such data are vital registration, health services statistics, and population-based inquiries. The countries of sub-Saharan Africa do not differ significantly from other developing nations in this range of sources; the difficulty lies in generally lower levels of coverage, completeness and reliability.7 The issues raised by the above assessment of the magnitude of pregnancy related mortality and morbidity portends great and dangerous consequences as well as rendering efforts at curbing and reducing pregnancy mortality and morbidity non-effectual. Vital statistics, in particular death certificates that could conceivably provide reliable information on the cause, cover less than one tenth of national population.9 Given the enormous problem faced by national ministries of health, more deaths occur at home than in hospitals. Hence, reliable data on this very important issue has continued to undermine the significance of issues involved, which underscores the difficulty at putting in the right perspectives the magnitude and extent of damage humanity has suffered in pregnancy related mortality and morbidity in Nigeria. While a number of developing countries have had satisfactory experience with health information gathered by primary health workers, this is still a relatively rare practice in Nigeria. This implies that reasonable assessment and estimation of maternal mortality will be based on statistics provided by the hospitals and clinics where data is still not available as obtained in other countries. This is further compounded if one considers the fact that only small proportions of women have access and resources to use hospitals. Hence, one may conclude that data from such sources (hospitals and clinics) are only reflective of those who deliver in hospitals but exclude those who deliver at home, traditional birth attendants, herbalists and spiritualists. In Niger State of Nigeria, 84% of deliveries take place at home,10 as are 62% of deliveries in Nigeria.11 Further critical analysis of the above scenario suggests that those who can afford to go to hospitals may be citizens who are of average and higher socio-economic status, better education and exposure. Hence, they face or contend with little or no risk at pregnancy because they are more likely to have had access to health care during pregnancy. If this is so, mortality statistics may be an underestimation of community mortality and morbidity. Bearing these biases in mind the figures available for pregnancy-related mortality presented in much of literature might not even approximate the true situation.12 Majority of countries in sub-Saharan Africa, particularly Nigeria, is faced with sexual and reproductive health crisis. Most of the region is characterised by persistent high levels of fertility, maternal mortality and morbidity, problems of family planning as well as HIV/AIDS and other related sexually transmitted diseases. In the report of a committee set up by the Board of International Health,13 it was identified that maternal mortality and morbidity as a reproductive health problem is unlike other public health problems in several ways. According to the report, although mortality is an ever-present threat, most women wish to be pregnant and deliver a child at least once in their lifetime. Thus, although primary prevention is not entirely relevant, the prevention of unwanted pregnancies is not simply crucial, but it is the single most important preventive intervention to reduce mortality and morbidity. While maternal mortality is similar to infant mortality but unlike infant mortality, there are no magic bullets as obtained in the Expanded Programme on Immunisation (EPI) or Oral Rehydration Therapy (ORT). It can be implied from this report that prevention of unwanted pregnancies can be a way out of the menace caused by unsafe abortion being procured at alarming rate. In another dimension, unwanted pregnancies and unsafe abortion seem insurmountable, given the sexual behaviour of adolescents. This is further compounded by the failure to include adolescents as part of the target for family planning programs. For instance, adolescents are usually not targeted for family planning programs, and their use of contraceptives is low in Nigeria.14 In 1990, the Demographic and Health Survey (DHS) confirmed that only 11% of single, sexually active women, aged 15–19 years used modern methods, while 22% used traditional methods. These rates are much lower than in the industrialised countries, where 58% of adolescents in the US and up to 90% in Sweden use contraceptive methods. This situation is further worsened by the sexual behaviour of most adolescents; 62.8% of adolescents had sexual experience before marriage and in most cases the adolescents have multiple sexual partners.6 The increasing high rate of infection with sexually transmitted diseases (STDs) among adolescents is another dimension to reproductive health. This is partly due to the high level of sexual activity with multiple sexual partners. There is a common high level prevalence of STDs in the sub-Saharan African region. Another study in Nigeria reported that 16% of female patients presenting for treatment for STDs were adolescents below 15 years of age. Therefore, given this trend, the younger female population is at greater risk of HIV infection.12 While significant progress has been recorded in infant and child survival, less progress is been made in maternal survival. Every year, over half a million women worldwide still die as a result of complications associated with pregnancy or childbirth. It is, however, sad to note that 99% of these deaths occur in developing countries.15 Some of the pre and postnatal complications that usually result in mortality and morbidity include haemorrhage, infections, obstructed labour, hypertension or cardiovascular disorders and abortion. All these are complications resulting from lack of proper care especially during labour and delivery. The maternal mortality and morbidity rate leaves much to be desired and a cause for concern if one considers or compares the situation in Africa with that of developed nations. Inadequate funds to conduct necessary research once or repeatedly has limited the level of knowledge on the trend in maternal mortality and morbidity in Africa. This has also made it practically difficult to carry out meaningful scientific study on the subject matter for obvious reasons. Given the underlying problems of unavailability of data and the lack of baseline information, available research reports are inconclusive. It is apt for scientists to look for new ways or strategies that will ease the burden of women in procreation. This can be achieved on a sustainable basis through the adoption of new initiatives that will address pertinent issues relating to the most disadvantaged members of our society, particularly women, who hardly have a say on matters related to their lives. This study was, therefore, conducted to determine women's reproductive health situation in Bida Emirate, with a view to advancing frontiers in communication intervention that will sensitise the entire inhabitants of the emirate in particular and the state in general. Findings from the study will be useful for shaping the reproductive health situation in Niger State and serve as a lesson for other states with similar socio-cultural setting in designing and implementing intervention initiatives. Statement of Objectives General Objective The study generally investigates the reproductive health situation of women of reproductive age in Bida Emirate of Niger State, Nigeria. Specific Objectives
Statements of Hypotheses
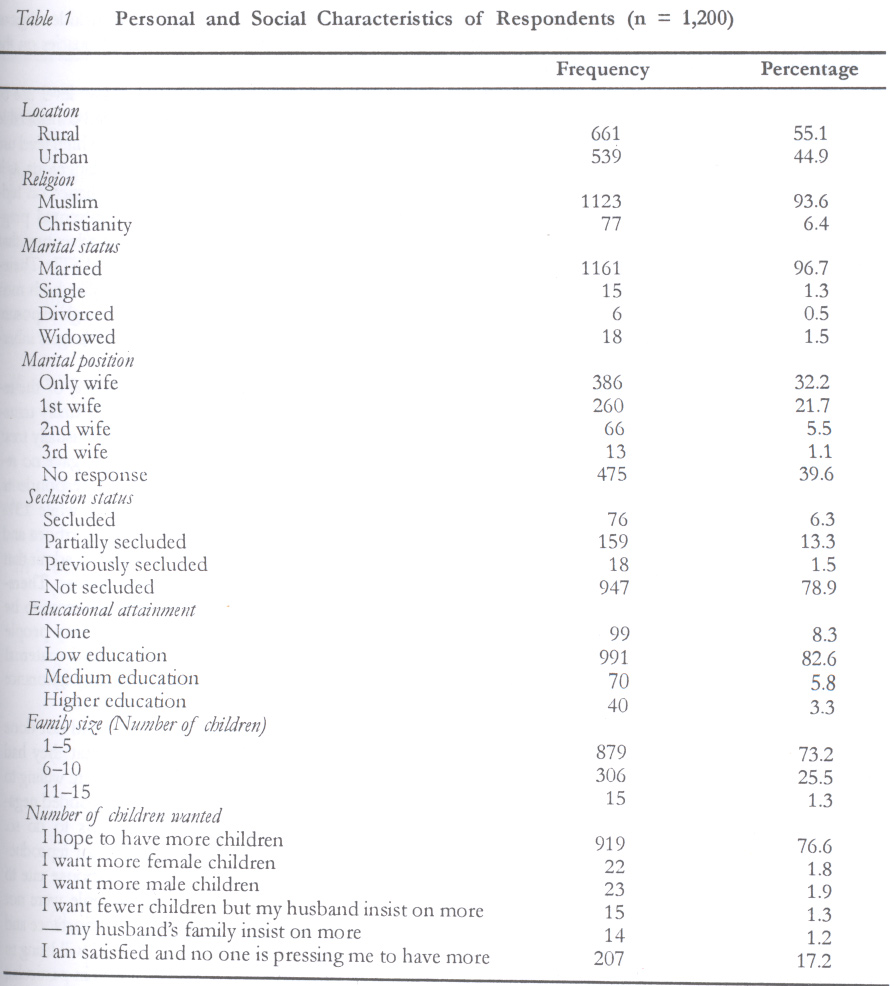
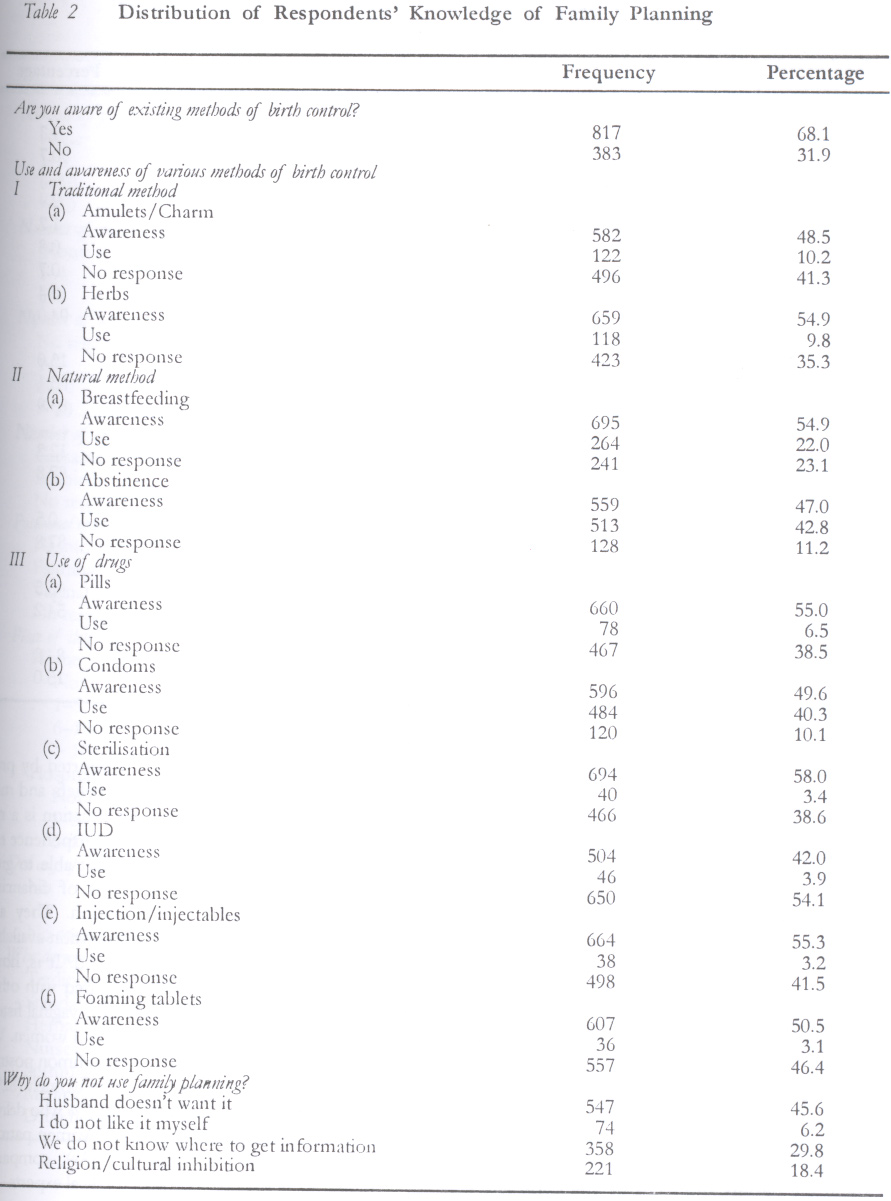
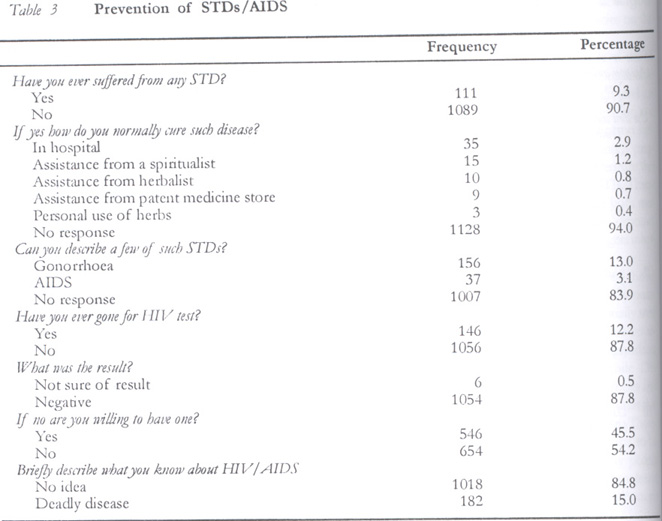
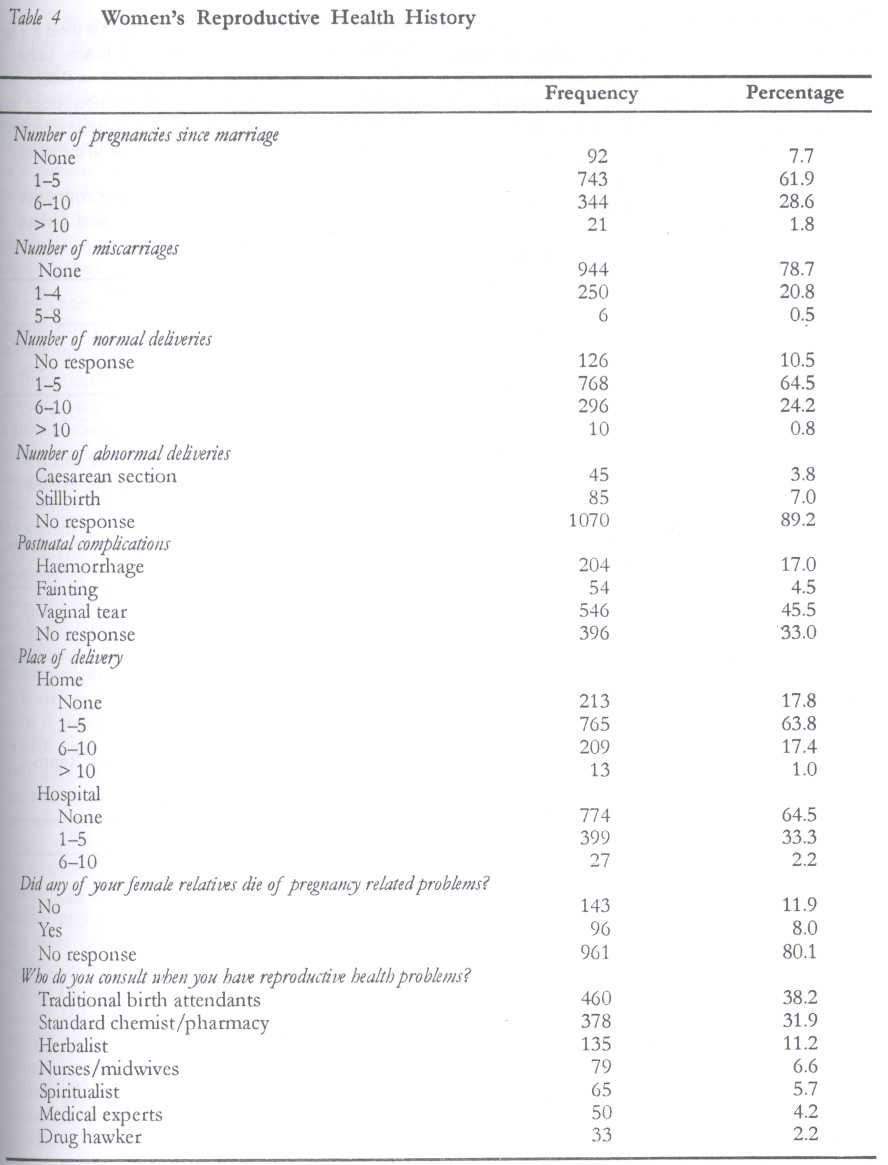
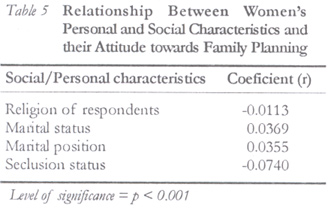
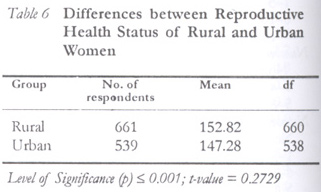
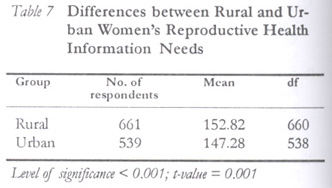
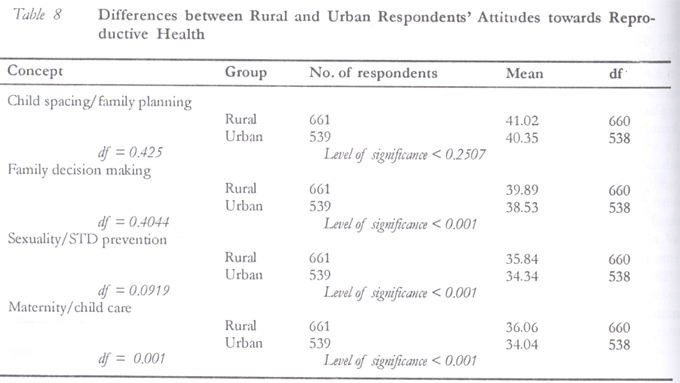
METHODOLOGY This study involved a field survey using questionnaire to generate data for correlation analysis with the statistical package for social sciences (SPSS). Area of Study The study was carried out in Bida Emirate of Niger State, Nigeria. Bida Emirate is located in the southwest of Niger State. The concept, emirate, was used in view of the significant role of traditional institutions on the pattern of life of the people. There are thirteen districts under the Bida Emirate Council, with the Etsu Nupe as the overall head (Emir). The districts are Bida township (north and south), Edozhigi, Doko, Badeggi, Rabba, Katcha, Kutigi, Lemu, Mokwa, Bokani, Gaba and Kede Districts. There are six local government areas in the emirate, namely, Lavun, Bida, Gbako, Katcha, Edati and Mokwa Local Government Areas. The native language of the emirate is Nupe, with other immigrant tribes like Hausa, Fulani, Yoruba, Ibo, etc. Majority of the entire population speaks Nupe, although Hausa is a lingua franca in the state, as is the case in several other northern states. The major occupation of the people is farming. There are two main religions in the entire Emirate – Islam and Christianity. The concept of emirate derives from the traditional kingship pattern where the Etsu Nupe presides over the entire Nupe Kingdom. However, the Emirate Council, under the leadership of the emir, exercises specific coverage and influence on those within Bida Emirate and beyond. There are other emirs in neighbouring smaller Nupe townships of Agaie and Lapai. However, considering the significance of the Etsu Nupe in Nupe kingdom, his overwhelming “Lordship” influence on his subjects determines the choice of the Emirate. Consequently, his legitimisation role was fully exploited in project execution. This had positive effect on our fieldwork and consequently accounts for successes in communities visited, given the sensitivity of the issues involved in the community. Sampling Procedure and Sampling Size A multi-stage sampling technique was used to select respondents for the study with the following procedure: Stage I Three rural districts, namely, Badeggi, Lemu and Mokwa, were randomly sampled while the two Bida urban districts were chosen for location comparison. Stage II The second stage in the study involved sampling of wards/villages in urban and rural districts. About 20% of wards/villages in sampled districts were randomly chosen from the list obtained from the village/ward head. Stage III A census of households in each of the wards/villages was conducted through the assistance of the ward/village heads. Consequently, about 10% of the entire households were randomly selected using systematic sampling procedure. Stage IV In the final stage, respondents for the study were randomly selected. The samples were stratified to allow sampling of women who were in their active reproductive years (15–45 years). All married women in each of the sampled households were interviewed. On the whole, a total of 1,200 women respondents participated in the study with more than one respondent in polygamous households. Measurement of Variables Personal and Social Data Respondents' personal and social variables measured include location (rural/urban), religion (Muslim/Christian), marital status (single/married/divorced/widowed), marital position (only wife/1st/ 2nd/3rd/4th wife), seclusion status (secluded, partially secluded, previously secluded, not secluded), educational attainment (none, low education, medium education and high education), family size (in terms of number of children). Knowledge of Family Planning Knowledge of family planning related variables were measured using awareness and use of various methods of birth control that respondents indicated. They were further asked to describe the methods and how they are used, after which they confirmed their use or non-use of the methods. During each interaction, their responses were scored; one point for correct answers and zero for wrong answers. The methods assessed included traditional, amulets/charms, herbs, natural method, breastfeeding, abstinence, modern methods, pills, condoms, sterilisation, IUD, injectables and foaming tablets. Prevention of STDs/AIDS Information was elicited from respondents on aware- ness about STIs and HIV/AIDS and whether they have suffered from any STD before. They were also asked details on how and where the disease was cured, description of any STDs/HIV test result or willingness to go for HIV test. Reproductive Health History (RHH) Variables related to reproductive health history of the respondents were measured, considering the number of pregnancies since marriage, number of miscarriages, number of normal deliveries, number of abnormal deliveries, postnatal complication, place of delivery, and experts consulted in case of any reproductive health problem. RESULTS AND DISCUSSION Table 1 indicates that majority of the respondents reside in the rural areas (55.1%). It further reveals that 93.6% of the women are Muslims while 6.4% are Christians. This wide variation is, however, due to the fact that only two Christian communities fall into the randomly sampled districts. It is apparent that the influence of Islam in Nupeland is quite significant to reproductive health reforms; hence, the fear of the unknown dominates the thinking of the people. That means reproductive health packages will continue to be limited to birth control and often interpreted as an attempt to reduce the number of Muslims who are already in the majority. There is, therefore, need to integrate religious leaders in development programs, because they enjoy spiritual and social respect from their followers. Table 1 excludes age due to inconsistencies noticed during interview sessions; some of the respondents were not sure of their approximate birth dates. For instance, a woman who was almost 35 years old could claim to be 20 years. Nobody wanted to be seen as an old woman because it could make the husband to go and marry a younger woman. It is evident from the study that most of the women had little or no formal education. Therefore, majority had elementary education and got married after. This development results in almost a case of no education. Hence, there was little or no room for variation or correlation. Majority of the respondents (96.7%) were married while only 1.3%, 0.5% and 1.5% were single, divorced and widowed respectively. On marital position, majorities were the first wives of their husbands (39.6%), while 31.2% were the only wife. Marriage in Nupeland is such an evergreen “enterprise” that remains a challenge to councillors and legislators. It is sad to see how young boys and girls are demobilised and forced into marriage even when they are not physically and economically prepared to undertake the tough obligations and challenges inherent in it. This is further worsened by the number of wives men like to have (one to four). Several questions needed empirical validation — How many married couples remain faithful after solemnisation? Does marriage prevent infidelity? Are men satisfied after having more than one wife and does this prevent them from engaging in extra-marital affairs? It is not the mandate of this paper to conclude, but it is evident from participant observation that there is still more work to be done in the area of community enlightenment and attitudinal change particularly among men. Women leaders must be encouraged to mobilise other women to take up the challenge, with every sense of commitment, to liberate innocent souls from the clutches of ignorance, morbidity, disease, depreciation and preventable deaths. It is sad to note here that women themselves are not helping matters when it comes to procreation. They often strongly desire to have more children even when morbidity cases are life-threatening, and reproductive health providers suggest that they stop having children. This is peculiar in polygamous households where competition to have sexual relationship with the husband is very high. On seclusion status, the table indicates that majority of the respondents (78.9%) were not secluded, while 6.3%, 13.3% and 1.3% respectively were secluded, partially secluded and previously but no longer secluded. This finding is peculiar to the socio-cultural setting in Nupeland. On educational attainment, majority of the respondents (82.6%) belonged to the low educational attainment categories, while 8.3% had no education at all. A lower percentage of 5.8% had medium education and 3.3% higher education. The low level of educational attainment observed for a majority of the women is not surprising, given the historical antecedents of gender discrimination in parental decisions on child education. Whenever the decision favours the female child, or in households where female children predominate, they are reluctantly given the opportunity that will terminate after a few years of elementary education. The generally low level of education among the women folk will affect the type of communication media to be used to reach them. Table 1 further reveals that majority of the women already had large family sizes, ranging from 1–5 children (73.3%) to 6–10 children (25.5%). This finding could be explained by the fact that the study area is largely an agrarian location where large family size is seen as security for farm labour. No matter the level of education children may attain or their level of involvement they are usually mandated to assist in the family farm. Table 2 provides an insight into respondents' knowledge of family planning. Findings reveal that majority (68.1%) of the respondents were aware of existing methods of birth control, while 31.9% were not. Respondents knew most of the methods but their level of use varied. Natural methods, namely, abstinence (42.8%) and breastfeeding (22%) were mostly used. Traditional methods were rarely used, while condom use was as high as 40.3%. This is not surprising because Nupe men are very jealous and would prefer to use condom when they feel the woman should not have a child. This corroborates women's response that their husbands were to blame (45.6%) for not using other known modern methods. The men feel if they allow the women to use modern methods they may engage in extra-marital affairs. The women generally knew that various family planning devices are available but could not use them for several reasons, principal among which is the husband's non-acceptance. Culturally, men decide for women, even when it directly affects the woman's life. Hence, a woman may desire to adopt or use a family planning method but the final decision will depend on her husband's approval, which she may never get. The situation is further worsened when she does not know where to get relevant information on family planning. Certain religious and cultural factors are also responsible for people's perception and appreciation of family planning. To break the jinx, therefore, both community and religious leaders must be involved in family planning programme campaigns in this study location. In another dimension, a general overview of the knowledge of respondents concerning family planning reveals that while awareness of traditional method is high, use is considerably low. The plausible reason for this is that people may just not know the advantages of such practices, or it may be due to the cultural influence of having more children for farm holding security/labour source. Other reasons may include religious misinterpretation and professional inadequacies on the part of health care providers. Comparatively, however, there is low level use of modern methods even though it recorded considerable level of awareness; respondents indicated high level use of abstinence. Abstinence is somehow dangerous, as it encourages fornication/adultery and reliance on hidden traditional practices to prevent unwanted pregnancy. This practice encourages sexual adventure that will lead to the spread of HIV/AIDS and STIs. Therefore, new strategies are needed to mobilise both men and women to adopt new methods through exposure to the advantages of these methods and dangers inherent in their current practices. Table 3 indicates that majority (90.7%) of the respondents had not suffered from any sexually transmitted disease. On how the respondents usually treat such diseases if infected, majority (94%) gave no response. Eighty three per cent of the respondents could not describe any of the diseases, while 13% and 3.1% respectively could describe gonorrhoea and AIDS. It is not easy for people generally to admit that they ever suffered from any venereal disease. Therefore, it is not surprising that everybody seems to be “free”. However, it is noteworthy that many people could not differentiate between STIs and maternal complications. This probably explains why ignorance about HIV/AIDS still characterises social life. On HIV testing, majority (87.8%) had not done any HIV test, while 12.2% indicated that they had done the test before. On whether they were willing to undergo HIV test, majority (54.5%) responded negatively, while 45.5% indicated willingness to do so. This finding has significant implication for reproductive health education, given the low response rate to questions on STD infection; many people were not willing to discuss the issue. Given the importance and relative advantage that safe motherhood will bring to humanity in general and the women folk in particular, reproductive health development is a challenge to humanity; therefore, concerted efforts must be made to tackle the poor sexual and reproductive health situation in Nigeria. The first step in this direction is to declare and recognise reproductive health as a public health problem not only through professional development but also through legislative support. Therefore, their causes, prevention and cure must be vigorously pursued. These assertions are significant to Niger State in particular and Nigeria in general. Table 4 shows the reproductive health history of respondents. Overall, 61.9% have had 1–5 pregnancies, while 28.6% have had 6–10 pregnancies. This is also similar to the trend in number of children. Hence, women were very proud to reveal the number of children they had, given the socio-cultural significance of having children in the study area. However, the situation is not the same with abnormal deliveries, which many perceive as a misfortune and would rather not discuss. On the contrary, postnatal complications are rather associated with the hazard of childbirth that must always be accompanied with such complications as haemorrhage, fainting and vaginal tear (45%). However, vaginal tear is most common. Given the premature age at which girls get pregnant, they lack both physical and mental development needed to withstand the rigours and pains of childbirth and general maternity. This is further supported by previous investigations of traditional beliefs and maternal mortality.17 This prevailing situation is a result of economic difficulties women experience especially when their husbands are not able to give the much needed support in terms of financial, moral and psychological consolation. They are therefore made to use the cheapest option available to them no matter the risks involved. It is, however, a better situation when compared with other states in northern Nigeria where vesico vaginal fistula (VVF) has had such a devastating toll on women. Vagina tear and haemorrhage are very common postnatal complications because majority of women (82%) deliver at home, compared to only 35.5% who deliver in hospitals. Secondly, 38.2% of the women patronise traditional birth attendants (TBAs), compared with only 4.2% who consult with medical experts. HYPOTHESES TESTING Ho1 — Significant relationship exists between women's personal and social characteristics (religion, marital status, marital position, and seclusion status) and their attitude towards family planning. Table 5 indicates that though weak relationships exists there is a significant relationship between personal and social characteristics of the respondents and their attitude towards family planning as a key variable in reproductive health and safe motherhood. This implies that women's attitude is influenced by their personal and social characteristics. Ho2 — Variation exists in the reproductive health status of rural and urban women of Bida Emirate. The result of the t-test analysis for differences in reproductive health status of rural and urban women as shown on Table 6 reveals that there is a significant difference in reproductive health status of urban and rural women (t = 0.2729; p < 0.001). The plausible explanation for this is the concentration and attendance of health centres in urban areas while only few functional rural clinics are available in the emirate. Ho3 — Significant difference exists between rural and urban women's reproductive health information needs. The result of the t-test analysis on Table 7 shows the differences in information needs of urban and rural women (t = 0.001; p < 0.001). This may be due to variations in exposure to reproductive health information from the two locations and perception of issues involved. Therefore, any intervention in this regard must take into consideration the particular needs of information starved rural areas. Ho4 — There is significant difference between rural and urban women's attitudes towards family planning and other reproductive health issues. The result of the t-test analysis on Table 8 shows that while there is no significant difference in attitude towards child spacing/family planning based on location (t = 425, p = 0.25). Therefore, women's attitude towards family planning is not based on their location. Hence, both rural and urban women perceive family planning in the same manner. The probable explanation for this is the sensitivity of family planning among the people. Thus, the use of child spacing notwithstanding, the people are already biased about reducing human population. No doubt, “poverty breeding” remains an unabated phenomenon irrespective of location. There are disparities in attitude based on location as it affects family decision making (t = -0.40, p < 0.001); sexuality and STD prevention (t = 0.09, p < 0.001); and maternity/child care (t = 0.001, p < 0.001). Therefore, the peculiar nature of rural areas must be the reason for these variations. This could be attributed to gender roles and expectations in the two locations. For instance, women in the rural communities are more actively involved in agricultural activities than their urban counterparts; hence, their level of involvement in family decision-making may be affected at different levels and for different activities. In another dimension, the same cannot be said of maternity exposure of urban women who lack the opportunity to participate in maternity routine in urban hospitals and clinics. Low level awareness about sexually transmitted diseases may be responsible for the apathy towards reproductive health in general. However, more specifically, variations in the concealment of history of suffering from these diseases could also account for this observation. CONCLUSIONS AND RECOMMENDATIONS In conclusion, the study has shown that there exists wide disparity between social expectations of women's reproductive health and cultural realities in Nupeland of Nigeria. The following conclusions could be made from the study: (i) Women are aware of common STDs like gonorrhoea and syphilis but are not aware of the dreaded acquired immune deficiency syndrome (AIDS). (ii) Women are aware of and use natural methods of birth control such as abstinence, breastfeeding and withdrawal but there is low awareness and use of drugs. (iii) Women usually consult traditional healers for assistance in reproductive health problems more than they do with medical experts in hospitals and rural health centres. (iv) There is a difference in the reproductive health information needs of rural and urban women. (v) Differences exist in the attitude of women towards reproductive health issues among both rural and urban dwellers. Based on these findings the following recommendations are made towards sustainable safe mother- hood campaign in culture bound societies like Bida Emirate: (i) In view of the significance of safe motherhood, awareness campaign and health education is of paramount importance if abortion, excessive bleeding and postnatal complications that are common reproductive health problems in the community are to be eradicated. These problems still exist because of ignorance of the opportunities available in orthodox medicine to address reproductive health problems. (ii) The rate at which women deliver at home could account for bleeding and other postnatal complications identified as one of the commonest reproductive health problems in the area. Hence, the traditional media can be used to reach the populace on the need to register at the hospital right from the beginning of pregnancy to delivery in order to reduce the rate of maternal mortality and morbidity in the community. (iii) In view of the variations discovered in the reproductive health needs of the rural and urban women as well as reproductive rights and decision-making, future intervention programs should put into consideration the differences in relation to their specific needs. (iv) Establish reproductive health services delivery centre in strategic locations in the rural and urban areas for information dissemination. (v) Update state health data bank with findings in reproductive health to serve as a viable statistical database for use in reproductive health policy formulation and implementation. (vi) Organise training programs for traditional birth attendants (TBAs), who are the closest maternal care providers at the grassroots level. In view of the gap created from these findings, it is suggested that further research into the following areas should be carried out: (i) Intervention programs that will recognise the personal and social characteristics of the people. (ii) Action programs that will involve community and religious leaders in mobilising the people for participation in reproductive health development programs. (iii) Further investigation into the status of sexually transmitted infections among women by health care providers. (iv) Mass awareness campaign and mobilisation to adopt recommendations and packages that will ensure safe motherhood in such culture bound societies. ACKNOWLEDGMENTS This study was sponsored by the MacArthur Foundation's Fund for Leadership Development (FLD) program in Nigeria, which provided enormous support for data collection and analysis. The author also appreciates the assistance of all those who participated in data collection, particularly, Razak Olajide, Mohammed Nda Aliyu, Nma Idris, Ndagi Yahaya and Kudu Liman; and the respondents who had to wait patiently during the lengthy interview sessions. The author solely bears responsibility for the shortcomings in this study. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02009t5.jpg] [rh02009t3.jpg] [rh02009t2.jpg] [rh02009t4.jpg] [rh02009t8.jpg] [rh02009t6.jpg] [rh02009t7.jpg] [rh02009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}