 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 1, April, 2002 pp. 65-73 Can Mothers Afford Maternal Health Care Costs? User Costs of Maternity Services in Rural Tanzania Marga Kowalewski1, Phare Mujinja2 and Albrecht Jahn1 1Institute of Tropical
Hygiene and Public Health, University of Heidelberg, Germany. 2Institute
of Public Health, Muhimbili University College of Health Sciences, Dar es Salaam,
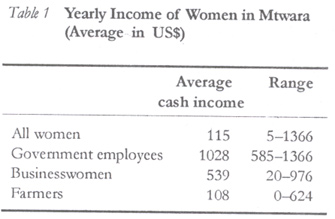
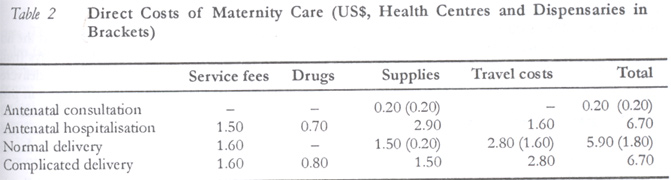
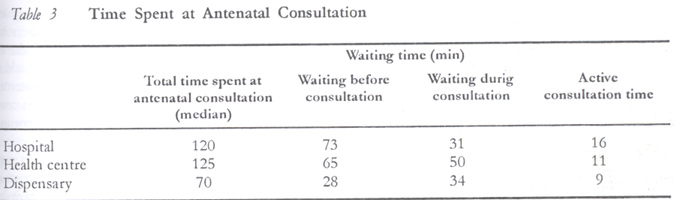
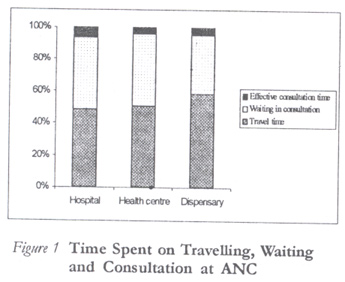
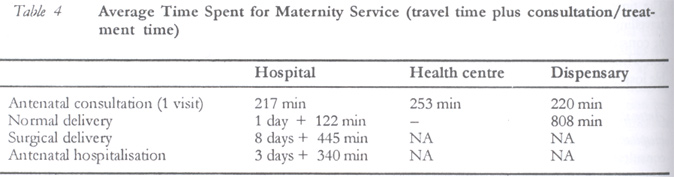
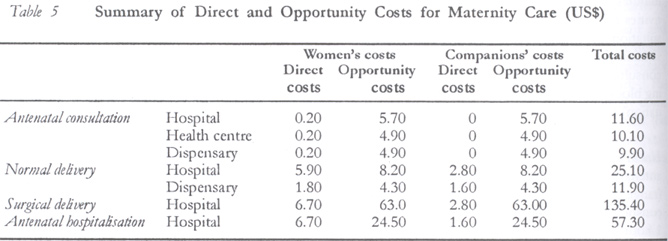
Tanzania. Code Number: rh02010 ABSTRACT Following the difficult economic situation various countries introduced health sector reforms, including user charges to finance the system. The assessment of user costs for maternity services in Tanzania was part of a larger study, which covered inputs, outputs and efficiency of services. The study was carried out from October 1997 to January 1998 in Mtwara urban and rural district in South Tanzania. One hundred and seven women attending a quarter of government health facilities were randomly selected and interviewed. Twenty one key informants were also interviewed and service procedures observed. Users of maternity services pay mainly for admission, drugs, other supplies and travel costs. Travel costs represent about half of these financial costs. The average total costs vary between US$11.60 for antenatal consultation and US$135.40 for caesarean section at the hospital. Unofficial payments are not included in the calculation. The amounts vary and payment is irregular. We therefore conclude that time costs are constantly higher than financial costs. High direct payments and the fear of unofficial costs are acute barriers to the use of maternity services. User costs can substantially be reduced by the re-organisation of service delivery especially at antenatal consultation. (Afr J Reprod Health 2002; 6[1]: 65–73) RÉSUMÉ Les Mères, Peuvent-elles se Payer les Services de Maternité? Les Coûts d'Ultilisation des Services de la Sante Maternelle en Tanzanie Rurale. Suite à la situation économique difficile, plusieurs pays ont introduit des réformes dans le secteur de la santé, y compris les frais d'utilisation pour financer le système. L'évaluation des coûts d'utilisation des services de maternité en Tanzanie faisait partie d'une grande étude qui a englobé les rapports et les rendements et l'efficacité des services. Cette étude a été menée entre le mois d'octobre 1997 et le mois du janvier 1998, dans les districts urbains et ruraux de Mtwuara au sud de la Tanzanie. 107 femmes qui fréquentaient un quart de facilités de santé mises en place par le gouvernement ont été selectionnées et interviewées au hasard. 21 principales informatrices ont été observées. Les usagers des services de maternité paient essentiellement pour l'admission, les médicaments, d'autres provisions et des coûts de voyage. Les coûts de voyage représentent à peu près une moitié de ces coûts financiers. Le coût total moyen varie entre US$11,6 pour la consultation prénatale et US$135,40 pour l'opération césarienne à l'hôpital. Les paiements non-officiels ne figurent pas dans le calcul. La somme payée varie et le paiement n'est pas régulier. Nous concluons donc que les coûts de temps est constamment plus élevés que les coûts financiers. Les paiements directs coûteux et la peur des coûts non-officiels sont les obstacles majeurs aux services de maternité. Les coûts d'utilisation peuvent être considérablement réduits si l'on reorganise la prestation de services, surtout la consultation prénatale. (Rev Afr Santé Reprod 2002; 6[1]: 65–73) KEY WORDS: User costs, opportunity costs, maternity services, antenatal care, obstetric care, Tanzania INTRODUCTION The economic perspective of health care has become a very pertinent issue because of the difficult economic situation of most developing countries, following the world-wide economic crisis of the 1980s. Reforms of the health sector have been introduced in various countries including decentralisation of health services and introduction of user charges to finance the system. However, several authors claim that user fees are implemented as policy objective instead of policy instrument and divert the neediest from the modern health care system.1,2 Users' contribution to health care is generally underestimated and opportunity costs are often not considered at all. The assessment of user costs was part of a baseline study on the costs of maternity services in south Tanzania, which included assessment of inputs to maternity service, outputs, and efficiency of services. It is generally agreed upon that household expenses for health care constitute an important share of total health care expenditures. Even cost-free services still impose opportunity cost.3 Household costs are generally divided into time and financial costs. The time costs include opportunity costs of foregone wages by the patient and time spent on travel, waiting and treatment. Also, the time invested by the caretaker or accompanying person of the patient has to be considered. Financial costs comprise all direct expenditures for health care by the household such as transport and drug costs, admission fees, and the costs of food and living at the treatment site for the patient and the caretaker. Berman4 reports that travel costs average about one third of the total costs per patient contact at health centres. Opportunity costs may be an important determinant of health service utilisation. More so, as Sauerborn5 found, time costs of illness consistently exceed financial costs. Consumers are assumed to be willing to pay quite high amounts for a service they value.6 However, Donaldson7 showed in his study that the willingness to pay did not imply the actual ability to pay. Abel-Smith3 found that more than 60% of the households would have borrowed money to pay for the services they received. In Tanzania 32% of rural and 22% of urban households found it difficult to pay for health care. When the same amount of service fees was introduced between two health facilities while perceived quality of care was different, people migrated to the facility perceived to be providing the higher quality service.8,9 Berman10 suggested that reporting on inputs, outputs and cost information become routine. The service costs of maternity care, as well as present and future user costs, are a necessary prerequisite for planning a more adapted programme for delivering maternity care. The costs of maternity services in Tanzania have not been investigated systematically and have not included user costs. This led us to the study question: What resources are spent by the users of maternity services to obtain the current level of care? MATERIAL AND METHODS Study Setting The study was carried out in Mtwara urban and Mtwara rural districts in the south-east of Tanzania from October 1997 to January 1998. The Mtwara region comprises five districts, and borders the Indian Ocean in the east. In the south, the River Ruvuma separates Tanzania from Mozambique. The region belongs to the less developed parts of Tanzania. About 90% of its population live in the rural area on subsistence farming. Health indicators are among the less favourable in Tanzania. The two Mtwara districts comprise a population of 274,325. Hospital-based maternal mortality rate of Mtwara region is reported to be 231 per 100,000 live births.11 The first level of care in the region is represented by health centres and dispensaries. The two districts have a total of 37 government dispensaries, 4 health centres (including one non-government) and 8 private urban dispensaries. All government as well as non-government health facilities supply mother-child health services (MCH). The study of Gilson12 found the MCH and delivery service at dispensary and health centre level to be of similar quality. The referral level (where comprehensive essential obstetric care is provided) is represented by the Ligula Hospital in Mtwara town. Other hospitals of the region are far away (100–200km). Inflow and outflow of patients in the region is balanced. Methodology This study used mainly quantitative methods. If, as in this study, the main interest is the costs incurred by maternity patients, it is justified to concentrate on service users only rather than doing a household survey.2 To establish the user costs, maternity care documents were reviewed, key informants (n = 21) were interviewed and structured interviews with 107 women at antenatal clinics (n = 59) and maternity wards (28 deliveries, 10 antenatal hospitalisations) were held at hospital, health centres and dispensaries. The questions were on time spent on travelling; waiting and treatment at the health facility; cash payments for service fees, travel, drugs and supply cost; the number of accompanying persons and their occupations; occupation of the woman herself; and the woman's annual cash income. Interview data were compared and verified by observing waiting and treatment time at antenatal clinics. Information on travel time and cost were compared with data from a study in 1996 on referral patterns in the same region.13 Information on service fees was compared with the official hospital cost sharing regulations. Unofficial costs (under-the-counter payments), which vary very much in amount and are not applicable to all patients, were not considered in cost calculation. They generally occur at hospital level and more often in complicated cases. Financial costs were directly calculated from the information on direct payments. The time costs were calculated on the basis of the foregone income of employees and businesswomen for the time spent in seeking maternity care. For farmers the foregone income (time costs) was an extrapolation of the once a year cash income for selling the harvest plus the costs of self-consumed farm produce (estimated by key informants at US$0.80 per day). The one-time income was spread over the full year to calculate a daily income. The total (economic) costs were the addition of time and financial costs. Reflecting the actual situation in Mtwara, the majority of women in our study population were peasant farmers (83%), 11% business or craftswomen, 3% government employees and 3% housewives without personal cash income. Fifty six per cent of peasant farmers did not earn cash income and lived on subsistence farming. Businesswomen and employees were concentrated in town and had a considerable higher average income than farmers. Sampling Process and Data Sources Health facilities were selected by random sample procedure except for the maternity ward and the MCH clinic of the regional hospital, which were chosen purposely. A random sample was drawn by lottery stratified for distance and access to hospital (< 10km from the hospital, 11–50km, > 50km). The sample includes nine dispensaries and one health centre, and represents a quarter of all government health facilities in Mtwara. The selected health facilities were asked to complete a detailed questionnaire. Five of the dispensaries and one health centre were visited by a research team to check for consistency of information and to complete missing information. Documents were also reviewed and interviews held. Two female interviewers, fluent in Kiswahili and English, were employed for conducting interviews with women who use maternity services. Questionnaires for interview with maternity users were prepared in English, translated by a research assistant and tested with five women at the MCH clinic and three women at the maternity ward. Incoherence in questions and answers were checked for misleading wordings in both English and Kiswahili questionnaires. The Kiswahili version was then retranslated by a third person to check for correctness. Limitations The calculation of time costs has its limitations and requires a set of assumptions.14 Government employees, for example, generally do not lose income by being absent from work. For peasant farmers the calculation of a daily cash income is based on the assumption that the annual income can be spread over one year and thus gives a daily rate. In reality the loss of time in planting or harvesting incurs much higher income losses than absence in the dry season. The calculation of opportunity costs for a few hours spent on antenatal consultation is equally arbitrary. A woman undertaking small scale farming usually looses a whole work day on the fields if she leaves in the morning for the health facility. RESULTS Financial Costs Users of the maternity services pay for four main categories of services — admission and bed fees, drugs, other supplies (like syringes and bandages), and travel costs. Admission and bed fees are paid once per admission. Direct Costs at Hospital Hospital services for pregnant women comprise antenatal consultation (US$0.20), antenatal hospitalisation (average costs to women = US$6.70), normal delivery (US$5.90) and surgical or other complicated delivery (US$6.70). Antenatal Consultation Antenatal consultation at any level of care is free. The financial costs of antenatal consultation (US$0.20) are due to direct payment for syringes (for vaccination). Travel costs are generally not incurred by women attending antenatal care because they come generally on foot and are not accompanied. Antenatal Hospitalisation Antenatal hospitalisation attracts financial costs of admission and bed fees (US$0.80 each) and drugs (average US$0.70, range US$0.20–US$1.60). The women also spend on average US$2.90 (range US$0.80–US$11) on medical supplies (syringes, gloves and IV and blood administration sets). Travel costs are incurred by the pregnant women and by their companions. One person's travel costs for coming to the hospital averages US$2.80. Normal Delivery For a normal delivery at hospital women pay the delivery fee (US$1.60). Patients at all levels of care do not pay anything for drugs necessary in normal delivery or for postnatal conditions. But half of the women bought syringes and gloves for treatment and a quarter of the women bought soap for personal hygiene upon advice of health workers. On average US$1.50 is spent on these items (range US$0.20–US$2.60). For hospital delivery, about one fifth of patients are accompanied by two people. A female relative will stay with the woman throughout her treatment at the health facility; the other person accompanies them on the way (often the husband or an elder relative who is also responsible for the money). One person's travel costs for coming to the hospital averages US$2.80. Complicated Delivery The costs of a complicated delivery comprise the same as normal delivery plus drug costs (usually antibiotics), which average US$0.80 (range US$0.10– US$1.60). An exemption system for maternity patients does exist although it is applied inconsistently, and usually hospital staff and their relatives are the beneficiaries. The financial costs of antenatal hospitalisation and complicated delivery only include official costs. Under the counter purchases (generally for drugs and medical supplies, which should be available at the hospital and should be covered by the hospital fees) were not included in the cost calculation because the payments are so irregular and amounts vary. They are reported by some women to range between US$0.20 and US$20 (median US$2.00). Direct Costs at Health Centres and Dispensaries Generally, delivery, hospitalisation, treatment and antenatal consultation at the dispensary or health centre level are free of charge. At one dispensary the purchase of syringes (US$0.20) was reported. Patients at health centres or dispensaries usually come on foot and pay only extraordinary travel costs (on average US$1.60). The few patients who are hospitalised at the dispensary or health centre before delivery pay on average US$1.60 for transport. Time Costs The time a user of maternity services spends on travelling, waiting for service, and during treatment or consultation results in loss of income. The person who accompanies the patient incurs comparable losses depending on how much time is spent. Antenatal Consultation Hospital: At the hospital antenatal clinic the median consultation time is 2 hours, with a range of 30 minutes to 4 hours. On average 61% (1 hour 13 minutes) is for waiting before the consultation activities start and 13% (16 minutes) for active consultation and treatment. Due to the service administration the patient also waits between the different consultation processes (registration, weighing, taking blood pressure, physical examination and vaccination) for about 31 minutes. Health centres: At health centres the median time for antenatal consultation is 2 hours and 5 minutes (range 20 minutes to 4 hours 30 minutes). Before consultation starts the women wait on average for 1 hour and 5 minutes (52% of the total time). The actual consultation takes on average 11 minutes (9% of the total time), and waiting in-between 50 minutes (40% of the total time). Dispensaries: At dispensaries it takes 1 hour 10 minutes (range 20 minutes to 4 hours 30 minutes). Forty per cent of this time is spent on waiting before consultation (28 minutes) and 12% of the time in active consultation (9 minutes). About 48% of the time (34 minutes) is spent waiting between the different consultation processes. Seventy three per cent of the women travel 30 minutes (median) or less for antenatal consultation at the hospital clinic. At the health centre, 25% of the women arrive within 30 minutes and 81% reach the health centre within one hour (median). At the dispensary 60% of pregnant women arrive within 30 minutes (median) and 71.9% within 1 hour. Normal Delivery At hospital women stay for one day on average for normal delivery. At health centres delivery patients stay for 12 hours on average and at dispensaries they leave after three to four hours. Forty per cent of women arrive at the hospital within 30 minutes for delivery, 61% reach there within one hour. To reach their dispensary women travel for 44 minutes on average. Figure 1 Complicated Delivery Women undergoing a caesarean section leave the hospital on average after 8 days. Antenatal Hospitalisation Antenatal hospitalisation is only offered at the hospital. On average women stay for 3.1 days (range 2–5 days) before they are discharged or delivered. Forty per cent of women with problems in pregnancy reach the hospital within 30 minutes. The average travel time is 1 hour 40 minutes. Rare antenatal admissions from the periphery of the districts sometimes travel for 8 hours or more. The people accompanying a woman delivering in a health facility were 84.2% peasant farmers, 7.9% crafts persons and 5.3% business people and employees. For delivery, almost all pregnant women (18.4%) were accompanied by two persons, of whom one stayed with the woman until she returned home. These accompanying persons add to the opportunity costs of the woman's maternity care and to the travel costs. Pregnant women coming for antenatal consultation were only accompanied in 20.3% of cases. Table 5 summarises all expenses for drugs, supplies, hospital fees and travel costs and the costs of time loss for hospital treatment of a farming woman. The main costs for users are the opportunity costs. The costs of antenatal care are similar at all health facilities. Hospital delivery is at least twice as expensive as dispensary delivery, and a caesarean section costs users at least five times more than a normal delivery at a hospital. In an extreme case at antenatal hospitalisation the cash payment amounted to US$41 (half of it unofficial payments) plus time costs of about US$49. Affordability of Services The yearly average cash income of a farmer in rural Mtwara is US$115. Our finding that about 45% of all women in the districts do not have any cash income (subsistence peasant farmers) highlights the problem of financial costs. In our interviews women elaborated mainly two things. First, the women manage to find 20 cents for antenatal consultation but can hardly afford higher amounts without selling assets or borrowing money. However, if the women feel their health situation requires treatment at a health facility the vast majority find the means to meet the cost of admission. This finding is supported by our earlier findings on reasons to use hospital services.16 Second, the high time costs are borne with complaints especially in antenatal consultation. The feeling of wasting time at consultation is often aggravated by the fact that drugs are not available or the laboratory tests are not ready. To use the day more efficiently the women go to the market or visit friends. DISCUSSION This study showed two main results. First, the opportunity costs are consistently higher than financial costs. But secondly cash payment for maternity services can be an acute barrier to use of maternity care. Time costs (opportunity costs) contribute between 32% (normal delivery) and 97% (antenatal care) of the total costs borne by maternity users at the hospital. In Burkina Faso5 the pattern for time costs was comparable to the one found in this study. Time costs consistently exceeded financial costs. The ways of dealing with time costs are also comparable. Women coming to antenatal consultation economise time by combining several activities on the same day, like going to the market. The time spent for institutional delivery is hard on multiparous women. Our study in 199613 showed that women with more than four children and women older than 35 years avoided actively hospital delivery and gave the following as reason: the mother is urgently needed to help with the farm work and there is no additional person free from farm work to care for the children during hospital admission. At Mtwara hospital 40–50% of time costs for antenatal care is for travelling to the treatment site. Only about 5% time costs go to consultation itself. The remaining time costs are for waiting in consultation. Waiting before the active antenatal consultation starts is part of the service provision policy. Health education sessions usually take place before any other activity starts and, therefore, these talks start only after a large group of women gather at the clinic. The waiting time during consultation could be much reduced by a re-organisation of service delivery. Instead of having six to seven stations in the course each staffed with one person, it could be reduced to maximum of three stations (registration, examination and counselling, and vaccination). This would also increase the contact time with one health worker who could have more chances to talk with the patient. The financial costs of maternity services can surpass the financial capacities of the families. But several studies3,6 showed a clear commitment of people finding quite high amounts to pay for emergency treatment (in this case caesarean sections). But the willingness to pay for maternity services is generally higher than the actual ability to pay.3 However, if the women feel their health situation requires treatment at a health facility the vast majority finds the means to afford the admission. Therefore, more than 90% of women with a previous caesarean section came to the hospital for their next delivery. In these cases the community and the health experts agreed on the necessity of hospital treatment, which facilitates the families' allocation of resources.15,16 The perception of the aetiology and appropriate treatment of a condition is important for the families' decision to contribute to costs. A study in rural Tanzania17 showed that in case of a traditional treatment the whole extended family participates in the costs. If a modern treatment is chosen the nuclear family generally has to bear the cost themselves. The unofficial costs of drugs and treatment are often higher than official payments. Unofficial purchase of drugs and medical supply has been described in many studies and is the rule and not the exception in almost all health facilities.18-21 Women gave these costs to be one of the most important reasons to avoid or delay hospital treatment. They fear more the unpredictable variations in the amount than the fact that these costs exist, because it is so difficult to be prepared for something unknown.22 Consequences for Service The national legal texts put free antenatal consultation as a right of each woman. An increasing number of health officials interpret this as free consultation, but drugs and materials are chargeable. Antenatal hospitalisation is generally payable and has, apart from caesarean section, the highest direct costs for service users. But fees and other costs are not uniform for all women, relatives of staff are often treated free of charge. Thus, the feeling that the hospital in Mtwara is only for rich people or those who know somebody at the hospital is not too far from reality.15 Abel-Smith3 found that 32% of rural households in Tanzania and 22% of urban households found it very difficult to pay for health care, and more than 60% of the Tanzanian households would have to borrow money to pay for the service they received. The same pattern was found in Bangladesh23 where the household costs of normal delivery were estimated at US$32 in a region with a median income of US$75 per month, which meant that 30% of families had to borrow money to cover their expenses in a “free maternity care” system. The introduction of user fees on top of indirect costs borne by patients forced some 20–26% of patients in Kenya out of the modern health care system.1 Another report from Swaziland shows that up to one third of people who stopped using modern health services were from the lower income group.24 CONCLUSION We therefore conclude that user fees should be well publicised, should be stable over longer periods, and be applied to all users of service. Thus, patients can prepare in time for the eventual expenses on delivery. A workable exemption system for the neediest should be developed and applied. Exemptions for civil servants and their families need to be re-assessed and possibly replaced by health insurance systems. An increase in user fees should be accompanied by sufficient improvements in service quality; otherwise a substantial fall in health service utilisation may be expected, like the examples from neighbouring countries have shown. Quality improvement could start by reducing the time costs in antenatal clinic (waiting time), being the service with the highest proportion of time costs. Travel and waiting time correlate negatively with service utilisation, whereas time spent in treatment associate positively with the utilisation of health services. Waiting before consultation for general health education talks has no proven impact on health-seeking behaviour of families. Individual health advice could be more effective. By re-arranging the flow of patients the contact time with one health worker could be increased and individual counselling become the central focus of consultation. Mothers can rarely afford the costs of maternity services. In most cases direct costs surpass the financial capacities of the nucleus family and they have to borrow money. The opportunity costs of waiting times and hospitalisation are especially hard on peasant farmers and mothers with many children. But in cases where hospital treatment is considered necessary by the family efforts are made to cover direct and opportunity costs. ACKNOWLEDGEMENTS We gratefully acknowledge the co-operation and invaluable help of staff at the regional hospital, the health centres and dispensaries of Mtwara Urban and Mtwara Rural health districts. Special thanks to Mrs. H. Kitundu, regional reproductive health coordinator, Drs Kimatta and Budeba, former and present regional medical officers, for actively supporting the study. Prof. S. Flessa (Nürnberg), Mr. F. Stierle (Frankfurt) and Mrs. S. Sax (Heidelberg) gave helpful comments on the study design and on earlier versions of this paper. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02010t2.jpg] [rh02010t1.jpg] [rh02010t4.jpg] [rh02010t5.jpg] [rh02010t3.jpg] [rh02010f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}