 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 1, April, 2002 pp. 74-83 Experiences of Mothers with Antenatal, Delivery and Postpartum Care in Rural Gambia Michelle L Telfer1, Jane T Rowley2 and Gijs EL Walraven2 1Divisional Health Team,
North Bank East and US Peace Corps, The Gambia. 2Farafenni Field
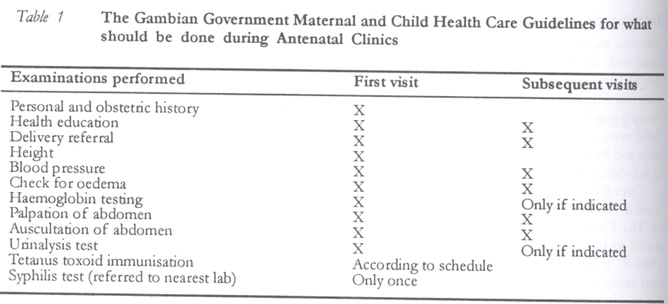
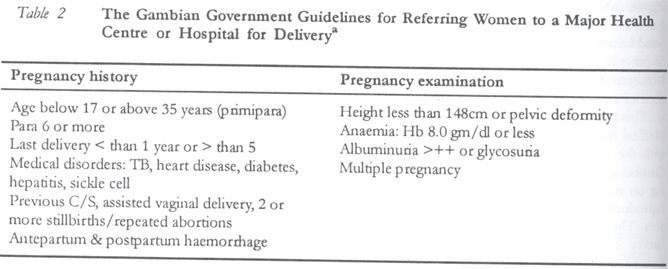
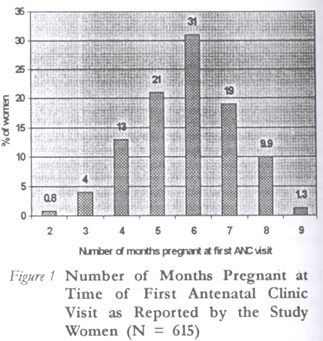
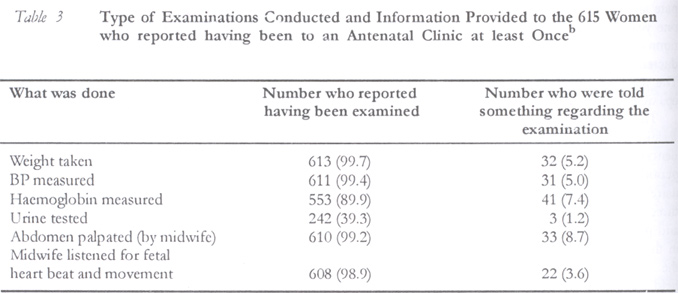
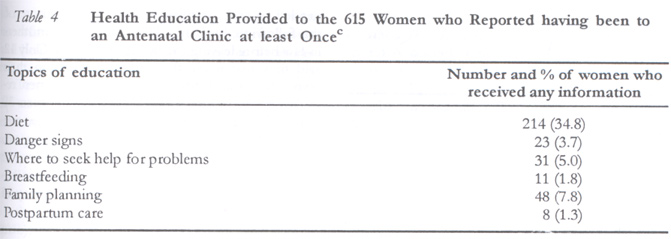
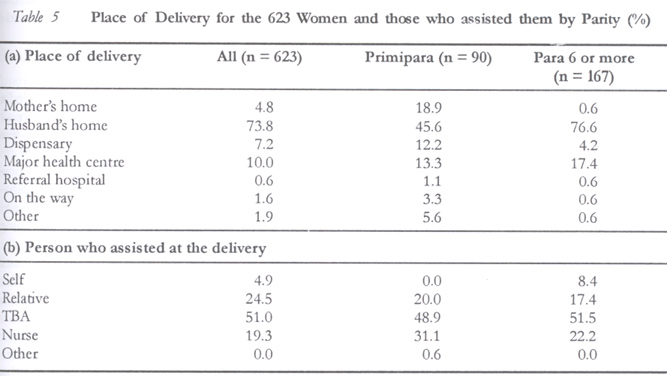
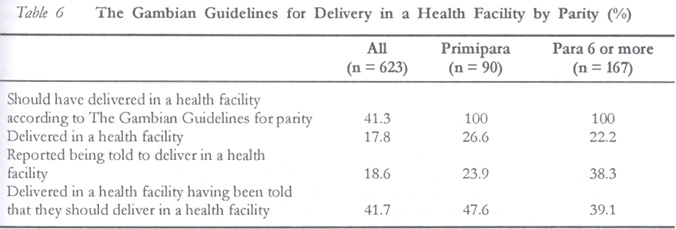
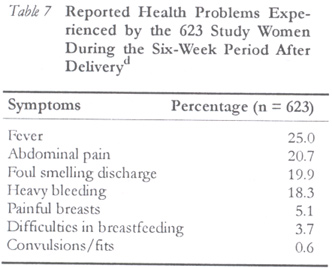
Station, Medical Research Council Laboratories, The Gambia. Code Number: rh02011 ABSTRACT Over the last two decades, the maternal mortality ratio appears to have fallen by up to 50% in the Farafenni, a rural area of The Gambia. This reduction almost certainly reflects improvements in access to essential obstetric services. The ratio, however, is still 50 times higher than in Western and Northern Europe or North America. This paper provides information from a community-based study of 623 women who had recently given birth in the Farafenni area. Information on how, when, and why care was accessed, and what type of care and information were provided were obtained from traditional and western methods of health care were during visits. Women were asked about their experiences during prenatal, delivery and postpartum periods. Results from this study highlight a number of opportunities for improving the quality of maternal health services that could be implemented relatively easily with existing resources. (Afr J Reprod Health 2002; 6[1]: 74–83) RÉSUMÉ Les Expériences des Mères face aux Besoins Prénatals à l'Accouchement et aux Soins Postpartum en Gambie Rurale. Au cours de ces deux dernières décennies, le rapport de la mortalité semble avoir baissé de jusqu'à 50% dans la Farafenni, une région rurale en Gambie. Cette baisse, si l'on veut, reflète certainement des améliorations par rapport à l'accès aux services obstétriques. Le rapport néanmoins est cinquante fois plus élevé qu'en Europe occidentale et l'Europe du Nord ou en Amérique du nord. Cet article fournit l'information recueillies d'une communauté dans le cadre d'une étude faite sur 623 femmes qui venaient récemment d'accoucher dans la région de la Farafenni. Nous avons pu obtenir des renseignements sur le comment, le quand et le pourquoi l'on a recherché le soin, ainsi que sur le type du soin assuré à travers les méthodes traditionnelles et occidentales de services de santé. On a posé des questions aux femmes sur leurs expériences pendant les périodes prénatales, de l'accouchement et du postpartum. Les résultats émanant de cette étude indiquent un certain nombre d'opportunités pour améliorer la qualité de service de maternité qu'on peut relativement mettre en oeuvre avec les ressources disponsibles. (Rev Afr Santé Reprod 2002; 6[1]: 74–83) KEY WORDS: Health care, antenatal, delivery, postpartum, The Gambia INTRODUCTION Maternal mortality ratio (MMR) is the health indicator with the largest gap between developed and developing countries, and it varies by a factor of over one hundred between the highest and lowest mortality settings. In 1995 it was estimated that there were over 515,000 maternal deaths worldwide and that over half of these deaths occurred in sub-Saharan Africa.1 Over the last two decades there has been a substantial decline in the MMR in the Farafenni area of The Gambia. In 1982–83 the MMR was estimated to be 2,362 per 100,000 live births, and by 1984–87 it had fallen to 1,091 per 100,000. A recent study suggests that the figure for 1993–1998 has continued to decline to 424 per 100,000.2 This reduction reflects improved access to care following the introduction of maternal health care programs and the launch of the WHO Safe Motherhood Initiative in 1986. However, the MMR is still 50 times higher than in North America, Western or Northern Europe, and much more needs to be done to reduce these inequities. This paper is part of a series of studies by the Medical Research Council (MRC) in collaboration with the Department of State for Health in The Gambia and the local divisional health team focusing on maternal mortality and morbidity, and the reproductive health of women in the Farafenni area. The paper reports on data collected from a survey conducted during 1998—1999 amongst women who had recently given birth to understand more about their access and use of health care before, during and after delivery. METHODS Maternal Health Care Services in The Gambia The Gambia is a small, low-income country in West Africa with a population of approximately 1.3 million. Access to health care facilities is good, with over 85% of the population living within 3km of a primary health care or outreach health post and over 97% of the population within 5km. The maternal and child health (MCH) program is run by the Department of State for Health (DoSH). In 1983 a primary health care (PHC) programme, which incorporated a strong mother and child health (MCH) component, was introduced in The Gambia. This programme included antenatal care (ANC), screening for high-risk pregnancies, a referral system for high-risk pregnancies and labour complications, and the identification and training of traditional birth attendants (TBAs) in each PHC village. National coverage of the program is close to 100%, with over 96% of women having had one or more antenatal care (ANC) visits, and 87% and 88% respectively of infants having been immunised against DPT and measles in 1999.3 The goal of the program is to reduce maternal and perinatal morbidity and mortality. Antenatal care services are available both through fixed clinics and mobile trekking clinics. The focus of these clinics is on screening for high-risk pregnancies, making appropriate referrals, and providing preventative and minor curative services (Tables 1 & 2). Women are encouraged to present early in pregnancy (first trimester) and to attend clinics monthly until delivery. A one-time fee of 5 Dalasi (approximately 0.5USD) is paid at the initial visit and entitles the woman to a health card and access to monthly antenatal clinics and delivery (overnight admissions are additional). Clinics are generally crowded and often understaffed, which can result in women waiting several hours before they have the requisite examinations. Up to five different people may be involved in taking weight, blood pressure, health history, haemoglobin, urine, physical examination and tetanus toxoid immunisation. The vast majority of women deliver at home either under the supervision of a traditional birth attendant (TBA) or a relative. In villages with a population of over 400 there should be at least one TBA who has received some government supported training. This training focuses on the recognition of complications, when to refer to health facilities, clean cord care and the administration of oral ergometrine tablets after delivery. Untrained TBAs also work throughout the area especially in the smaller villages and hamlets. After delivery women are to return for a postpartum visit, usually within four to six weeks of delivery. During this visit the woman is to be examined and the neonate registered and immunised. Study Area The study was conducted between October 1998 and May 1999 in forty villages near the town of Farafenni. The MRC has been supporting a continuous demographic surveillance system in these villages since 1981, which covers the registration of residents, migrants, births, and deaths. The total population in the study area on 31 March 1998 was 16,116, of whom 3,736 were women aged 15–49 years. Most people in the area are subsistence farmers and 45% have an income below US$150/year.4 Women marry for the first time at a mean age of 15 years and average 6.8 births.5 Islam is the dominant religion and approximately 98% of the population are Muslims. In the early 1980s medical facilities in the study area were limited to two dispensaries, one in Farafenni town staffed by a dispenser and a midwife, and another located in a large village (Ngayen Sanjal) east of Farafenni. Transportation was by bicycle, horse and donkey carts and some bush taxis travelling on dirt roads. In 1983 a new health centre opened in Farafenni town staffed by between two and four doctors, and essential obstetric services became increasingly available. Three mobile teams consisting of a midwife, a community health nurse, a public health nurse, and auxiliary workers started trekking monthly to eight villages in the study area to provide antenatal and child welfare services. Within the study area, 15 of the 40 villages were sufficiently large (population 400) in 1983 to be designated PHC villages and they continue to be the only PHC villages in the area. It is in these villages that there are trained TBAs. In the second half of the 1980s, regular bus services were begun between the larger villages and Farafenni on the North Bank Highway and ambulance services became available between Ngayen Sanjal dispensary, Farafenni health centre, and the referral hospital in the capital, Banjul. Telephone services were installed in the larger villages in the early 1990s. A maternity waiting home with six beds next to Farafenni health centre became operational in 1997, though it was mainly used to accommodate patient overflow from the health centre. Over the last 15 years there has been a marked change in the place of delivery. Between 1982 and 1998 the proportion of women delivering in a health facility had increased from 4.6% to 18.0%. DATA AND METHODS The Farafenni demographic surveillance system was used to generate a list of all women who delivered between October 1, 1997 and September 30, 1998. All of these women were invited to participate and were interviewed between six weeks and one year after delivery using a standardised questionnaire. The first round of interviews was conducted between October 1998 and January 1999. The team visited each village in turn and follow-ups were conducted between February and April 1999. The questionnaire focused on women's health-seeking behaviours, perceptions of care, and experiences during pregnancy, delivery and postpartum period. Prior to being administered, the questionnaire was forward and back translated into the three local languages (Mandinka, Wollof and Fula) and piloted. Interviews were conducted in private in the language of the woman's choice, usually in the woman's home, by one of five experienced field workers and lasted approximately 45 minutes. At the end of the interview each woman was asked to produce her antenatal card, if she had it, so that it could be photocopied and it was then photocopied and returned. The cards served a two-fold purpose: first as a check on what women reported and second to see how well the cards were being used by health care workers. The study was approved by the joint Gambian government/MRC ethical committee. RESULTS Background Of the 670 women identified in the surveillance system 623 (93%) were interviewed. Only two women refused to be interviewed and two were not eligible, as they had given birth outside the study area. The remaining 43 were either travelling or were at work and were not found at home during the two rounds (23), had moved out of the study area (13), or had died (four, one classified as maternal death due to postpartum haemorrhage, three as non-maternal by verbal autopsy).2 One woman was dumb and could not be interviewed. All but five of the women interviewed were married (99%); one woman was widowed, two were single and two were divorced. Two hundred and ninety seven (48%) of the women were in a polygamous marriage. The reported number of pregnancies (including the most recent pregnancy) ranged from 1 to 12, with 90 (14%) primigravidas and 101 (16%) reporting seven or more. Only 36 (5.7%) women reported having ever tried to avoid or delay pregnancy. Of these, 19 reported having used an injectable form of contraception and 15 the pill. Education levels in the study population were low. Only 16 (2.5%) had attended primary school for any length of time and just two had attended secondary school. Most of the women had received some Islamic education (520 or 83%), but this was generally for only one or two years. Pregnancy Period Attendance at antenatal clinics (ANC) was high, with only 8 women reporting not having gone at least once during their pregnancy. Over 50% of women presented for the first time in their fifth or sixth months of pregnancy (Figure 1). When asked what first prompted a woman to go for her first ANC visit, 406 (66%) responded that “it was time to go”, 161 (22%) cited access to delivery care, 36 (5.9%) said it was “for a healthy baby”, 9 gave other reasons and 3 did not respond. Ninety nine per cent of the women reported that they asked for permission to go for ANC. Nearly all of them reported asking permission from their husband (566 or 93%), who in most cases paid for the ANC card. Only 18 (2.3%) of the women paid by themselves. The mean number of ANC visits reported was 3.5, and 549 (88%) women said they had attended all of their scheduled appointments. The most common reasons given for missing an appointment were “too busy” (28 or 37%), “feeling ill” (23 or 30%) and “away or travelled” (16 or 21%). Mobile clinics covered the area widely and almost all (603 or 98%) walked to the ANC. During the clinic visits over 98% of the women reported having had their weight and blood pressure assessed and abdomen palpated and auscultated at least once. However, very few (3.6–8.7%, depending on the examination) were told anything about the examinations (Table 3). Nearly all (605 or 98%) women were given iron and folate tablets at least once. The number of months women reported taking them ranged from zero to eight, with a mean of 3.2 months. Forty six (7.6%) said they stopped taking the pills mainly because they made them “feel sick” (42). Women received almost no health education at ANC clinics especially with regard to pregnancy and delivery danger signs, where to seek help for problems, or postpartum care (Table 4). Only 13 (2.0%) reported being told during pregnancy or delivery to have a postpartum check on their health. TBAs played a minor role in providing care prior to delivery — only 74 (12%) of the women had reported seeing a TBA prior to the onset of labour. Delivery Nearly 90% of the women reported delivering where they had planned. Majority delivered at their husbands' home (460 or 74%) (Table 5a). For the whole sample, 111 (18%) delivered at a health centre, dispensary, or hospital and 10 delivered on their way to a health facility. Of the 111 who delivered in a health facility, 40% planned in advance to deliver there as a matter of preference, 33% were told to do so by a health care worker, 22% went because of labour difficulties, and the remaining 5% gave other reasons for going (e.g., sudden start of labour while visiting a relative who lived near the health facility). Four women had a caesarean section, giving a community caesarean section rate of 0.64%. One hundred and fifteen (19%) were told during one or more ANC visits to deliver in a health facility and of those only half (58) were told why. Less than half (48 or 42%) of those who were told to deliver in a health facility actually did so (Table 6). Despite the national guidelines, only 24% of primips and 38% of women who were para 6 or higher said they had been told to deliver in a health centre. Only 10 women who delivered at a health facility were at the health facility or the maternity waiting home when labour began. For those who weren't, the decision to go was made anywhere between 20 minutes and 48 hours after labour had started. Most of the women reported that they needed to seek permission from one or more of the following: husband, TBA, mother, or mother-in-law before leaving for the health facility. Only 12 said they had made the decision to go on their own. Once the decision was made 18 women reported having experienced a delay of between 30 minutes and 12 hours in setting off and all but two of such delays were caused by a lack of transport. Of the 500 women who planned to deliver at home only 19(3.8%) had made arrangements in advance for transport and 21 (4.2%) for money in case of any emergency. Few women reported delivering on their own (4.9%). Table 5b records the breakdown of the people who assisted them. TBAs and relatives assisted in 76% of all deliveries. Postpartum Period Nearly all (584 or 94%) reported having attended a MCH clinic within 30 days of delivery. Nearly all the women said their child was vaccinated at this visit. However, only 30% of the women (185) reported having being examined. The most commonly reported examination was abdominal palpation. Less than one quarter reported receiving any information on breastfeeding or family planning (122 or 20% and 138 or 22% respectively). Many women (Table 7) reported feeling unwell or experiencing unusual symptoms. Twenty five (4.0%) women reported that they or their babies had a problem that resulted in their going to a health facility within the first 35 days postpartum. TBAs continue to play an important role post-delivery. Most (442 or 71%) women were visited at least once by a TBA after delivery. The majority (337 or 76%) of TBAs came for the first 7 days postpartum (traditional length of confinement to the home after delivery). Antenatal Card Information ANC cards were recovered from 377 out of 615 (61%) women who reported visiting an ANC clinic. The number of visits recorded ranged from 1 to 9 with a mean of 3.2 and was similar to the number reported by women. None of the cards, however, had been consistently filled. Two hundred and fifty three (60%) cards had no reference to recommended place of delivery, 204 (54%) had no information on previous birth complications, and height measurements were missing on all but two. Test results were also erratically reported; urine dip test for proteinuria and glycosuria were marked as being performed for 278 (74%) women but results were only recorded for less than half (116 or 42%), of which 21 (18%) were positive. The one exception was haemoglobin testing. This was marked as being performed on 371 (98%) of the cards and results were recorded on 324 (88%), and ferrous and folate tablets were recorded as provided to 372 (99%) women for a mean of 3.1 months. DISCUSSION Attendance at ANC in The Gambia is very high, reflecting consistent and low cost care and the close proximity of trekking stations (almost all women were able to walk to the clinics). Charges for ANC are relatively low and are consistent with the national policy. The popularity must also reflect that women believe visiting ANC clinics is beneficial. The current government recommendations are for women to “come early and come often” to antenatal care; however, women frequently present well into the third trimester for their first visit (30% after 6 months). Part of this problem is cultural, as women do not usually “announce” a pregnancy but wait for other family members to discover it. There is also some reticence in not wanting to “tempt fate” by announcing too early and inviting miscarriages. Educational messages focusing on the importance and benefits of early and regular attendance at ANC need to be developed with sensitivity to the cultural issues surrounding early attendance. A major problem with late presentation is that it does not provide enough time to effectively treat or prevent anaemia, an important indirect cause of maternal mortality. While distribution of iron folate tablets is routine for all pregnant women in The Gambia regardless of haemoglobin level, the typical two to four ANC visits is not sufficient for oral iron folate to correct severe or even moderate anemia.6,7 Additionally, women frequently receive less than the recommended number of iron and folate tablets due to shortages and the perception among local health workers that women do not take the pills. Interestingly, in our study only 7.6% of women reported that they had stopped taking the pills. This may be due to lack of understanding of what the pills are for and what side effects they have. Options for improving iron and folate supplementation include reduction in frequency of administration and use of formulations that delay iron release in the stomach to decrease gastrointestinal side effects.8 TBAs and other primary health care workers can also improve the impact of supplementation programs by counselling women on why, how, and when to take iron and folate supplementation and by supplying the tablets.9 In countries where malaria is an important contributing factor to anaemia during pregnancy the prevention and treatment of malaria in pregnant women also has an important role to play. Community-based distribution schemes have been shown to be effective in addressing this issue.10 One option for improving ANC care is to make better use of the visits that do occur by tailoring activities. New WHO recommendations and the results from a number of studies suggest that measuring weight, and in some cases blood pressure, at every visit is not necessary or effective.11-15 By performing certain examinations at designated visits, depending on gestation, more focused care with specific goals can be provided. A potential difficulty with tailoring visits based on gestation is that women may feel slighted if they do not receive the same care at each visit or if they don't receive the same care as their companions.13 Illness during pregnancy was the main reason given for missing ANC appointments, and is a cause for concern. Illness should be a motivating factor for keeping appointments not a deterrent. Increasing awareness of this reason for missing ANC appointments amongst PHC workers and its inclusion in the design of health education messages are important first steps in mobilising pregnant women to seek care when sick. The fact that women receive little or no information regarding their ANC examinations, advice on where to deliver, or health education before or after delivery needs to be considered in order to make a change. Women in our study area appear to have limited understanding of the risks involved and the danger signs in pregnancy and delivery. They also need to receive information about the possible dangers during the postpartum period and how to recognise symptoms of infection and shock.15 Visits to the clinic need to be tailored such that each woman will be able to discuss with the health staff about her visit.16 ANC offers an excellent opportunity to provide women with the necessary information to recognise early warning signs of labour, delivery and postpartum life-threatening complications. Women at clinics are captive audiences, often for hours. While noise and multiple languages can pose difficulties in conducting health talks, pictorial banners, puppet shows and portable video shows can be used effectively to counter this difficulty. ANC cards can provide useful information for health care workers and for the woman and her family if properly filled for on-going and future pregnancies. The number of ANC cards that were recovered in our study is encouraging, however, the number of ANC cards that were not properly filled warrants attention. The recommended place of delivery and the woman's obstetric history are critical especially if she needs to go to a health facility in an emergency and cannot relay her history. In an illiterate and uneducated population, maintaining a written ANC card is not of use to the woman directly if the information is not available to her. Correctly filled ANC cards provide a record that even if the woman is unable to read a relative or neighbour, who is literate, can use to determine where she should deliver. Retraining of health staff on proper and consistent filling of cards needs to be carried out. Inclusion of pictorial representations of emergency conditions has been successful in some areas and might be a consideration for future cards.17,18 TBAs currently do not play an important role in antenatal care. They do, however, attend half of all deliveries and visit 70% of all women during the postpartum period. Unfortunately, their focus is almost without exception on the neonate after delivery. It appears that once a woman has delivered her health is no longer important because the health of her newborn is the focus of attention for TBAs and the health care system. A considerable proportion of maternal deaths occur during the postpartum period and septicaemia is the third most common cause of maternal death in the main referral hospital in The Gambia.19 While there is recent controversy over the usefulness in training TBAs, they are still the most accessible, culturally acceptable, and economically feasible birth attendants for low-risk deliveries.20 The training for TBAs should emphasise the postpartum care of the woman as well as the neonate. Besides, attention to hygiene during the delivery, at least one postpartum visit within one week of delivery, should be possible for the TBA. The TBA could check the mother for fever and abnormal lochia, to make sure that breasts and genitalia are kept clean, as well as making sure that satisfactory establishment of breastfeeding occurs. Arrangements for transportation and money in the event of an emergency are not being made. Lack of transportation was cited as the reason for delay in 16 out of 18 cases. This is a difficult obstacle to overcome in rural areas, and interventions have had little success.21 Encouraging women and their families to have an emergency plan in place that includes access to cash for transport and additional persons who can grant permission for her to seek care if her husband is not available could have some effect. Unfortunately, until rural areas have better access to modern roads and transportation, emergencies that arise during the night will not be averted, as horse and donkey carts cannot safely travel at night on mud roads that frequently wash out. Opportunities for improving care during the postpartum period include conducting more thorough examinations to identify current health problems, ensuring breastfeeding has been successfully established and encouraging use of family planning. Community-based distribution of iron folate supplements during the postpartum period deserves consideration, as high levels of anaemia persist and late first consultation precludes adequate supplementation during pregnancy. Improving access to and the quality of health care during pregnancy, childbirth and the often neglected postpartum period are important elements of efforts to further reduce maternal mortality and morbidity in developing countries, but they are not enough. Community perceptions and experiences must be taken into account. This highlights the need to devote more attention to sharing information with both women and men to ensure that they have a better understanding of pregnancy, childbirth, and how to take full advantage of the services available. The role of men in determining women's health care must not be ignored. While they may not participate in the intimacies of women's health care they play a paramount role both financially and in decision-making of when and where women receive health care. It is essential that men are not only included in future education campaigns but also have specific programs targeted at bringing them into an active role in maternal and child health. ACKNOWLEDGEMENTS We want to thank the field workers, Hawa Manneh, Khaddiatou Jallow, Emily Mendy, Louie Loppy and Sheikh Mafugi Dibba, for their assistance during the interviews. This study is part of a multi-site study involving seven demographic surveillance sites in three West African countries, The Gambia, Senegal and Guinea-Bissau, co-ordinated by Dr Jean-François Etard (IRD, Senegal). Funding for the project was provided by the European Commission/Fourth Framework Programme for RTD/INCO-DC (contract number: ERBIC18CT970248) and the UK Medical Research Council. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02011t6.jpg] [rh02011t1.jpg] [rh02011t3.jpg] [rh02011f1.jpg] [rh02011t7.jpg] [rh02011t2.jpg] [rh02011t4.jpg] [rh02011t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}