 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 23-29 Correlation Between Intrapartum Fundal Height and Birth Weight HE Onah1, ACC Ikeme1 and PO Nkwo1 1Department of Obstetrics
and Gynaecology, University of Nigeria Teaching Hospital, Enugu,
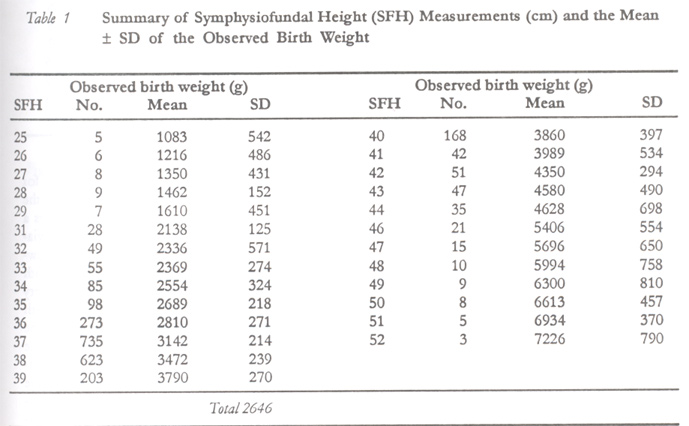
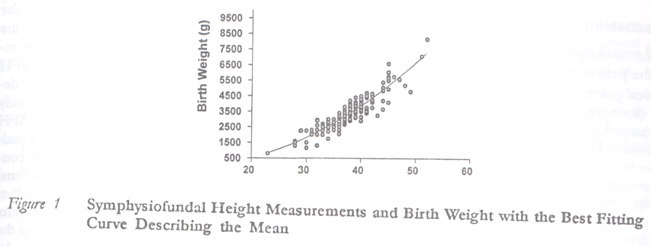
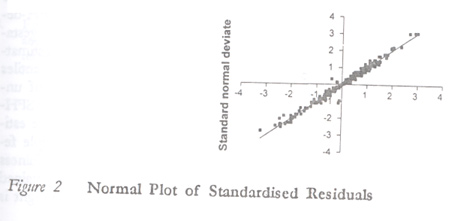
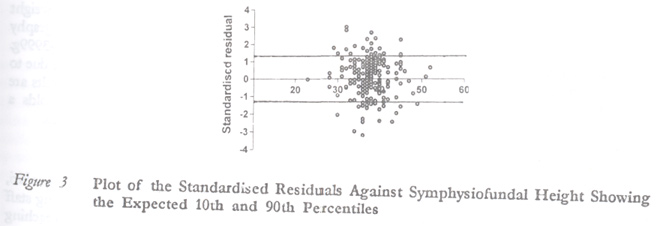
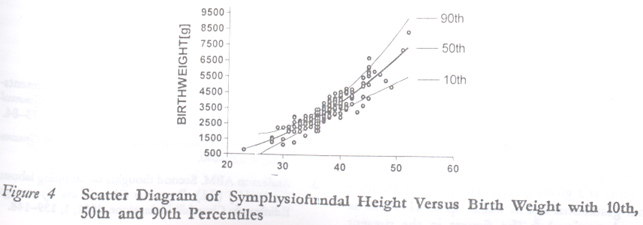
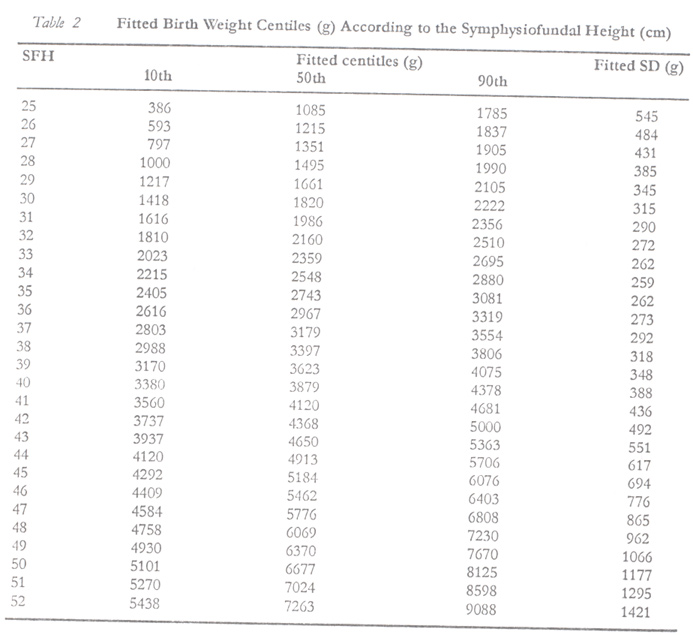
Nigeria. Code Number: rh02018 ABSTRACT In a prospective cross-sectional study, the correlation between symphysiofundal height (SFH) and birth weight was evaluated in 2646 consecutive parturients at the University of Nigeria Teaching Hospital, Enugu, over a 19-month period. The standard deviations of the observed birth weights were least when the SFH measured 33–39cm, which corresponded to the birth weight range 2500–3999g. The overall standard deviation was 275g. A second order polynomial fitted the data best, giving the equation y ± 258.1-62.9x-3.8x2, where y represents the observed birth weight in grams and x the SFH in centimetres. The R2 statistic for the model was 0.82. This and other assessments showed a good model fit. The birth weight centiles for the various SFH measurements were derived and their usefulness discussed. It was concluded that the SFH-derived birth weight centiles are useful alternatives to ultrasonography especially in the birth weight range 2500–3999g. (Afr J Reprod Health 2002; 6[2]: 23–29) RÉSUMÉ La Correlation entre l'Intrapartum de la Hauteur Utérine et le Poids de Naissance. Dans une étude transversale perspective, nous avons évalué la correlation entre la hauteur utérine symphose (HUS) et le poids de naissance chez 2646 parturientes consécutives au Centre Hospitalier Universitaire d'Enugu au Nigéria, à travers une période de 19 mois. Les écarts types de poids de naissance observés étaient à leur niveau le plus bas quand la HUS mesurait 33-39cm qui correspondait à la zone de poids de naissance 2500-3999g. L'écart type global était ± 275g. La polynomie du second ordre convenait le mieux aux données, ce qui a donné l'équation y = 258,1–62,9x–3,8x2, là où y représente le poids de naissance observé en grammes et x représente la HUS en centimètres. La statistique R2 pour le modèle était 0,82. Cette évaluation ainsi que les autres se révélaient de bons modèles. Les centiles de poids de naissance pour les différentes mesures de la HUS ont été obtenues et leurs avantages ont été discutés. La conclusion était que les centiles de poids de naissance obtenues à partir de la HUS sont des alternatives utiles à l'utltrasonographie, surtout dans la zone 2500–3999g. (Rev Afr Santé Reprod 2002; 6[2]: 23–29) KEY WORDS: Symphysiofundal height, birth weight, correlation INTRODUCTION Accurate determination of fetal weight remains a challenge for obstetricians in cases of breech presentation, previous difficult labour, fetal macrosomia and previous caesarean section.1-3 While ultrasonography, clinical palpation and gestational age derived birth weight centiles remain the main methods of birth weight estimation,3-6 each of these methods has varying degrees of accuracy and limitations. In developing countries, these methods are associated with additional limitations. In these countries, ultrasonography is available in only a few centres for a limited part of the day. Even when available, not all patients can afford the cost. Clinical estimation by palpation depends on experience, which may be lacking in many obstetric care personnel in these countries. Virtually all currently available gestational age derived birth weight centiles are for singletons and so are unsuitable for multiple gestations. Additionally, approximately 20% of the rural obstetric population in these countries are unsure of their dates.7 Gestational age derived birth weight centiles are also unsuitable for those women with unsure dates who cannot afford or access ultrasonography. The inexpensive and easy availability of the non-elastic tape makes it attractive for use in fetal weight estimation particularly in developing countries, hence the attempt in this study to revisit its use for this purpose despite previous poor predictive reports.8,9 MATERIALS AND METHODS This was a prospective cross-sectional study of consecutive parturients who presented at the University of Nigeria Teaching Hospital, Enugu, Nigeria, from 1st September 1998 to 31st March 2000. Those with clinical or ultrasonic evidence of uterine fibroids, polyhydramnios, oligohydramnios, fetal anomalies or death, and unsure dates were excluded. All other parturients were included irrespective of gestational age, number of fetuses, membrane status, maternal weight, head descent, route of delivery and presence of pregnancy complications other than the ones in the exclusion criteria. A research team consisting of a senior registrar and three registrars took all the measurements. All members of the research team had been using a non-elastic tape to routinely measure the symphysiofundal height for at least three years previously. As soon as a parturient meeting the above criteria was admitted for vaginal or abdominal delivery, a member of the research team measured the distance from the top of the fundus to the top of the symphysis-pubis three times to the nearest centimetre using a non-elastic tape with the centimetre side of the tape facing down, the patient supine, her urinary bladder empty and uterus relaxed. The mean of the three readings was then obtained to the nearest centimetre. The birth weight of the baby was measured in grams to the nearest 50g by the midwife on duty within six hours of delivery using a weighing scale. The midwives who weighed the babies after birth were blind to the intrapartum estimates of fetal weights. The method of data analysis used was that described by Altman et al.10 The mean birth weight for each symphysiofundal was estimated by fitting a polynomial regression model to the raw data. First, second and third order polynomial curves were tested for best fit to the data using the graph pad prism statistical software. The residuals between the observed birth weight values and the fitted line were plotted against symphysiofundal height to show if and how the variability changes with symphysiofundal height (SFH). Next the standard deviation (SD) of the birth weights for each SFH was calculated and this was modelled as a function of SFH. A second order polynomial fitted the standard deviations best. For each observation, the standardised residual (or standard deviation score, SDS) was calculated from the formula: SDS = (observed value - fitted mean)/fitted standard deviation. These standardised residuals were used for checking the assumptions underlying the modelling and for calculating the centile corresponding to any observation. The goodness of fit of the model was assessed in three ways. First, the R2 statistic was calculated. Second, a plot of the standardised residuals against SFH was examined for the existence of any patterns. Additionally, the standardised residuals were assessed for normal distribution by plotting them against the standard normal deviates. Third, the proportions of the observations above the 90th and below the 10th centiles were calculated. Finally, the centiles were derived by reference to a table of standard normal distribution. For example, the 10th and 90th centiles were obtained as mean ± 1.285 SD. The 50th centile corresponded to the fitted mean. All the calculated centiles were superimposed on a scatter diagram of the observations as a final check of the fit. RESULTS Two thousand six hundred and forty six out of the 2789 parturients who delivered during the study period satisfied the inclusion criteria and their data were analysed. The mean maternal age was 29.3 ± 5.5 years (range 17–42 years). The mean parity was 2.6 ± 2.2 (range 0–8). The mean gestational age was 38.5 ± 2.6 weeks with a range of 28–42 weeks. Two hundred and thirty one pregnancies (8.7%) were under 37 weeks, 1988 (75.1%) at 37–40 weeks and the remaining 427 (16.1%) pregnancies at or beyond 41 weeks gestation. The mean birth weight of the 2767 babies was 3225 608g (range 850–5050g). Two hundred and fifty four (9.2%) babies weighed less than 2500g, 2195 (79.3%) weighed 2500–3999g, while 318 (11.5%) weighed 4000g or more. In further analysis, the combined weights of the multiple fetuses have been used as single entries. Table 1 summarises the number of women and the mean ± SD of the observed birth weights for each SFH. The table shows that the standard deviations of the observed birth weights were least when the SFH measured 33–39 cm. Below 33cm and above 39cm, the standard deviations were wide. The overall standard deviation was ± 275g. Of the first, second and third order polynomial regression models tested for best fit to the raw data, the second order polynomial fitted best (Figure 1), giving the equation: y = 258.1 - 62.9x + 3.8x2, where y represents the observed birth weight in grams and x the symphysiofundal height in centimetres. The R2 statistic for the model was 0.82. Similarly, the second order polynomial fitted the standard deviations best with the regression equation as y = 4377 - 242.6x - 3.6x2, where y is the standard deviation in grams and x the symphysiofundal height in centimetres. Figures 2 and 3 show the diagnostic plots for the symphsiofundal height. Figure 2 shows the normal plot of residuals, while Figure 3 shows a plot of the standardised residuals (standard deviation scores) against symphysiofundal height showing the expected 10th and 90th percentiles. Both plots show that the data meet the assumptions very well. Figure 4 shows a scatter diagram of the birth weight versus symphysiofundal height with the 10th, 50th and 90th centiles superimposed. Some 8.2% of the observations were below the 10th centile while 13% of the observations were above the 90th centile values. The estimated birth weight centiles for the various symphysiofundal height measurements are shown in Table 2. DISCUSSION The overall standard deviation of ± 275g obtained in the present study is superior to the ± 450g for clinical palpation and ± 450g for biparietal diameter (sonography) reported by other researchers.11 As judged by the standard deviations (Table 1), the estimated birth weight is most accurate when the symphysiofundal height measures 33–40cm, which measurements correspond to the birth weight range 2500–3999g, a finding similar to ultrasonic birth weight estimates.4 Thus, estimation of birth weight by symphysiofundal height measurement is a useful alternative where ultrasonography is not available or affordable. However, sonography is superior to SFH in estimating low birth weight babies, while both methods show wide standard deviations for birth weights above 4000g.4,12 The wide variability of the birth weights when the SFH is less than 33cm can be explained by the fact that most of these extreme preterm pregnancies are pathological. On the other hand, wide variability of the birth weight when the SFH is 40cm is similar to the observations of other workers with regard to other fetal measurements — head circumference, biparietal diameter, etc.13 The SFH derived birth weight centiles will be found most useful in clinical situations where knowledge of the minimum, maximum and the approximate fetal weight are all required for clinical decision-making. For example, with an SFH measurement of 37cm, there is 80% probability that the birth weight of the baby will lie between 2803g (the 10th centile weight) and 3553g (the 90th centile) with a mean of 3179g. Therefore, a woman with a previous difficult delivery of a 4000g baby but with an SFH measurement of 37cm at term in the index pregnancy may be allowed a vaginal delivery in the index pregnancy. The overall R2 statistic of 0.82 and Figures 2,3,4 show a good model fit for the data, a contrast to the results of previous authors8,9 who used linear regression models and obtained poor correlations. Table 3 shows a comparison of the 50th percentile birth weights derived from gestational age14 and from SFH (present study) in our population. The table was based on the assumption that the mean SFH (cm) at a given gestational age corresponded to that gestational age in weeks up to 41 weeks as reported previously.8 The figures in the present study are consistently higher, which means that the assumption of equivalence does not hold at the gestational ages shown as confirmed by a more recent study.7 A multiple linear regression of SFH and gestational age with birth weight as the dependent variable from the data in the present study showed beta weights of 231.7g per cm for SFH and -13.4g per week for gestational age with a multiple R of 0.9 and R2 of 0.81. This further confirms that the higher the SFH at a given gestational age, the bigger the weight of the fetus. In other words, the SFH at a given gestational age is a more important determinant of birth weight than is the gestational age. Hence, the superiority of SFH-derived birth weight centiles over those of the gestational age derived birth weight centiles in estimating birth weight. Secondly, SFH-derived centiles have an advantage in the common finding of unsure dates in developing countries.7 Thirdly, SFH-derived birth weights has applicability in the estimation of the combined weights of multiple fetuses.12 A prospective validation of the usefulness of the SFH-derived birth weight centiles obtained in the present study in estimating fetal weight is currently in progress. We conclude that SFH-derived birth weight centiles are useful alternatives to ultrasonography especially in the birth weight range 2500–3999g. Previous poor results with this method were due to the use of wrong models. If the present results are validated by future studies, the method holds a great promise for use in developing countries. ACKNOWLEDGEMENTS The authors are grateful to Drs C. M. Ogbuokiri, U. Nwagha and A. Eze-Nliam and the nursing staff of the labour ward, University of Nigeria Teaching Hospital, Enugu, for assisting with the study. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02018t2.jpg] [rh02018f3.jpg] [rh02018f2.jpg] [rh02018t1.jpg] [rh02018t3.jpg] [rh02018f4.jpg] [rh02018f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}