 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 39-50 Infant Feeding and Lactational Amenorrhea in Sagamu, Nigeria OA Dada1, FA Akesode1, DM Olanrewaju1, OA Olowu1, O Sule-Odu1, TA Fakoya1, FA Oluwole1, BV Odunlami1 and WHO Task Force on Methods for the Natural Regulation of Fertility2 1 Centre for Research
in Reproductive Health, Obafemi Awolowo College of Health Sciences, Ogun State
University Teaching Hospital, Sagamu, Nigeria.2United Nations Development
Programme/World Health Organization/World Bank Special Programme of Research
Development and Research Training in Human Reproduction World Health Organization,
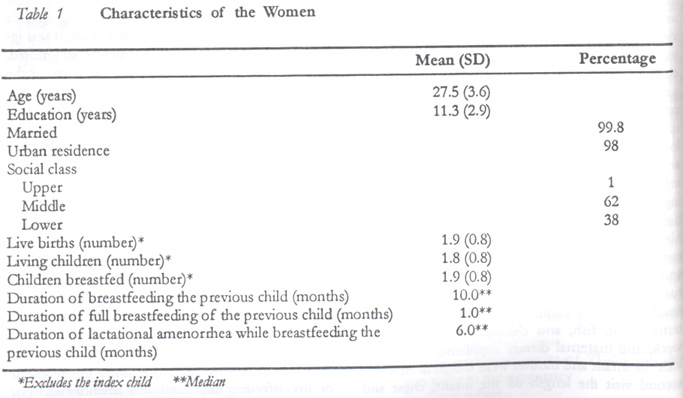
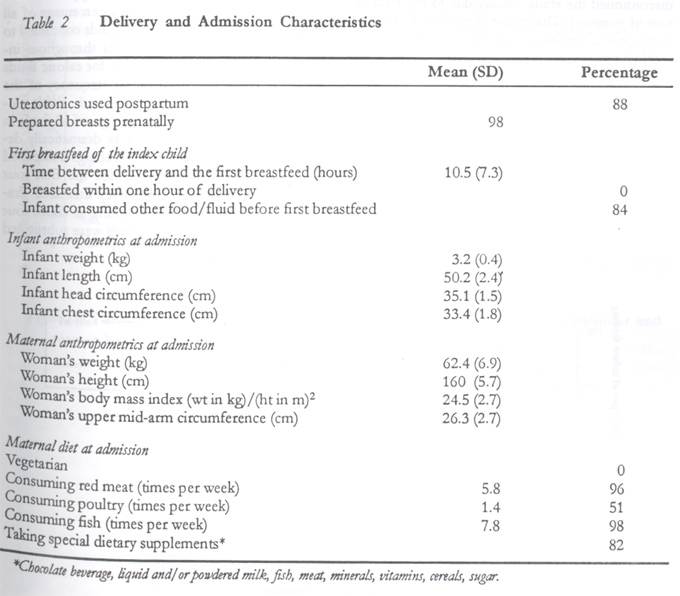
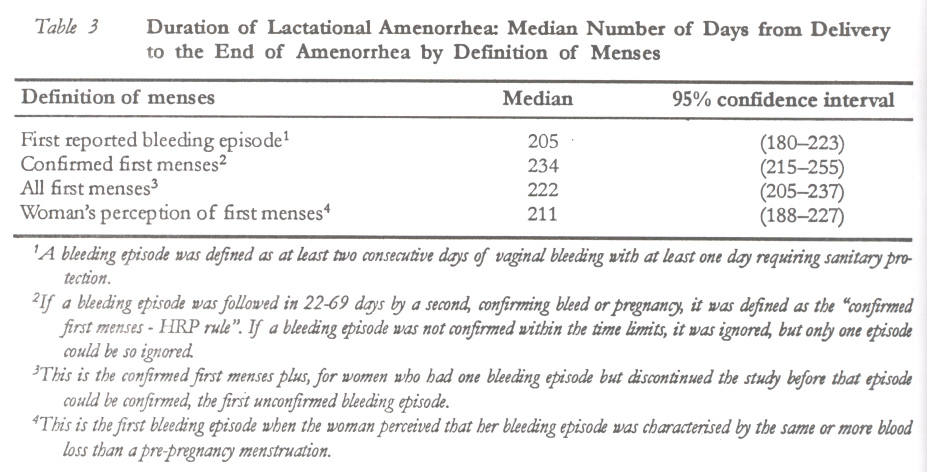
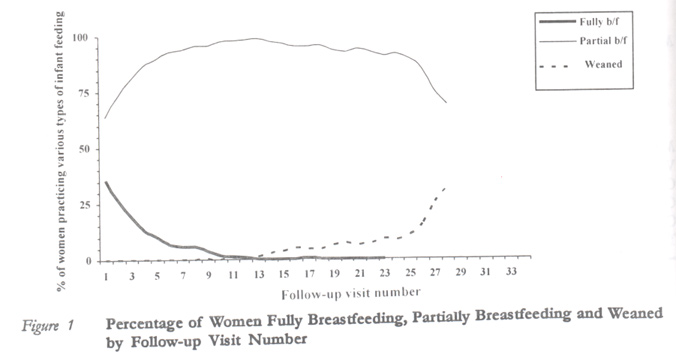
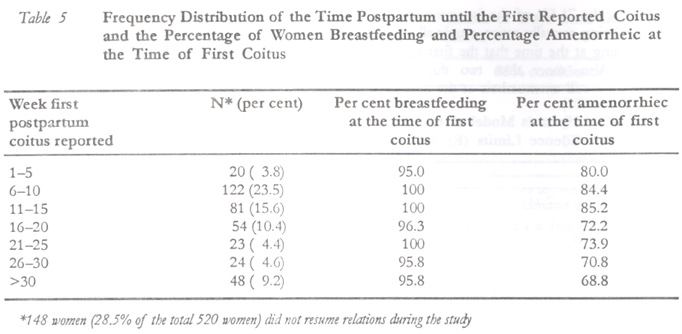
Geneva, Switzerland. Code Number: rh02020 ABSTRACT Five hundred and twenty educated, breastfeeding women in Sagamu, Nigeria, were observed prospectively in order to describe their infant feeding practices and to determine whether any predictors of the return of menses could be identified. The women remained amenorrheic for seven months. Compared with similarly selected women in other countries, they regularly fed their infants with supplements from a very early age, yet breastfeeding frequency and duration did not decline dramatically. Semi-solid food was introduced at about four months and such supplementation, as well as earlier supplementation with milk/milk-based feedings, was associated with the return of menses. The median duration of abstinence was about four months but the mean may have been much longer. No woman became pregnant until her infant was weaned. (Afr J Reprod Health 2002; 6[2]: 39–50) RÉSUMÉ L'allaitement et l'aménorrhée qui se rapporte à la lactation à Sagamu, au Nigéria. Cinq cent vingt femmes instruites et allaitant à Sagamu ont été observées prospectivement afin de décrire leurs pratiques d'allaitement et pour déterminer s'il était possible d'identifier quelques indices du retour des règles. Les femmes sont restées aménorrhéiques pendant sept mois. Comparées aux femmes qui ont été selectionnées de la même manière dans d'autres pays, elles nourrissaient régulierement leurs enfants du supplément dès leur très jeune âge; pourtant la fréquence de l'allaitement et la durée n'ont pas baissé de façon dramatique. A l'âge de presque quatre mois, on a initié les enfants à la nourriture semi-solides. Une telle administration d'un supplément aussi bien qu'une administration antérieure d'un supplément du lait et d'autres nourritures à base du lait, ont été associées au retour des règles. La durée médiane de l'abstinence était à peu près quatre mois, mais la moyenne a probablement duré plus longtemps. Aucune femme n'est devenue enceinte qu'après avoir sevré l'enfant. (Rev Afr Santé Reprod 2002; 6[2]: 39–50) KEY WORDS: Breastfeeding, fertility, Nigeria, infant, amenorrhea Africa INTRODUCTION Breastfeeding has always been vital in Nigeria. Its natural anti-infective properties and ideal nutritional characteristics have long facilitated infant survival. The natural contraceptive effect of breastfeeding has also enabled infant survival by delaying subsequent pregnancy long enough to allow an infant to be nourished and immunologically protected by her/his breastfeeding mother. The period of breastfeeding in communities in Nigeria has been characterised by abstinence from sexual relations, which also has had an important child-spacing effect.1 International interest in the relationship of infant feeding patterns to lactational infertility prompted the World Health Organization to conduct a prospective study to describe the duration of lactational amenorrhea in relationship to breastfeeding practices in seven different populations.2-5 The study attempted to establish whether there are real differences between these populations in the duration of lactational amenorrhea for similar breastfeeding practices, and to learn about the determinants of lactational amenorrhea. The study saw important differences in infant feeding practices2, in the duration of lactational amenorrhea3, and even in postpartum lochia5 across the study centres, as well as significant protection from pregnancy during lactational amenorrhea.4 It also identified ten variables associated with the duration of lactational amenorrhea in the seven centres combined.3 The seven study centres were located in Australia, Chile, China, India, Guatemala, Nigeria and Sweden. Centres were chosen that were geographically and culturally diverse and which had the capacity to perform the research, including the ability to recruit an adequate number of subjects. The African research centre in the multinational study was located in Sagamu, Ogun State, Nigeria, operated by the Centre for Research in Reproductive Health at Obafemi Awolowo College of Health Sciences, Ogun State University Teaching Hospital. The purpose of this analysis is to describe the Sagamu data on infant feeding, lactational amenorrhea, postpartum abstinence and pregnancy, and to determine whether there are any predictors of the return of menses in the Sagamu sample. Any important differences between Sagamu and the six other country centres will also be explored. Sagamu is the largest urban area in Ogun State, Ogun being nearly the southern-most western state in Nigeria. Around the time of this study, the town enjoyed the highest levels of education in the country, the lowest total fertility rate and teen pregnancy rate, highest age at first birth, and most knowledge and use of contraception in Nigeria.6 At the time of the study, the median duration of breastfeeding in Nigeria was 19.5 months, although this was lower in the southwest (16.1 months), in urban areas in general (15.3 months), and in women who completed secondary school education (13.3 months). Early supplementation to breastfeeding in the country is very common, beginning at 1 1/2 months and at 1/2 month in urban areas and the southwest. The first breastfeeding after birth is commonly delayed, with only 17% of women in the southwest beginning to breastfeed within an hour of birth and 43% within a day of birth.6 The median duration of postpartum amenorrhea (largely but not entirely lactational amenorrhea) in the country has been estimated at 14.6 months, but this duration is lower among women below the age of 30 years (13.8 months), women in the southwest (13.2 months), urban women in general (12.0 months) and women who have completed secondary school (8.5 months).6 Postpartum abstinence is reportedly practiced for a median of 10.8 months in the country overall, 13.8 months among women below 30 years of age, 13.2 months in the southwest, 12.0 months among urban women, and 8.5 months among women who have completed secondary school.6 METHODOLOGY Procedures The study methodology can be read in detail elsewhere.2,3 The research procedures that apply to the present analyses are included here. Normal, healthy, breastfeeding, full-term infants and their mothers were admitted into the study within one week of delivery if they met these additional criteria:
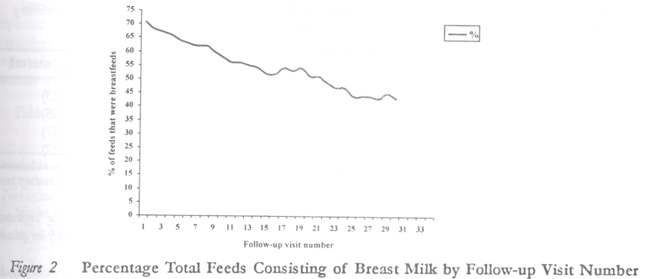
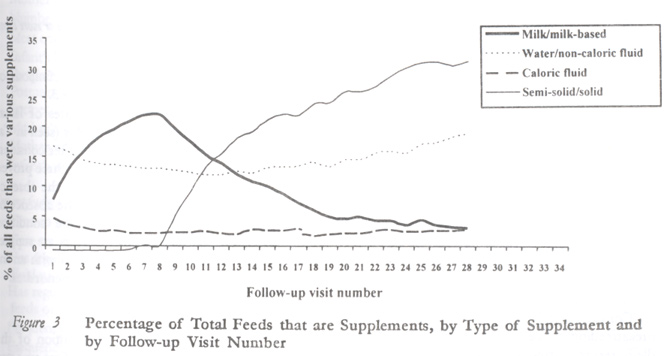
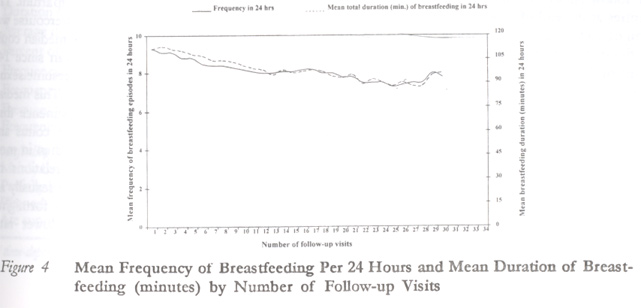
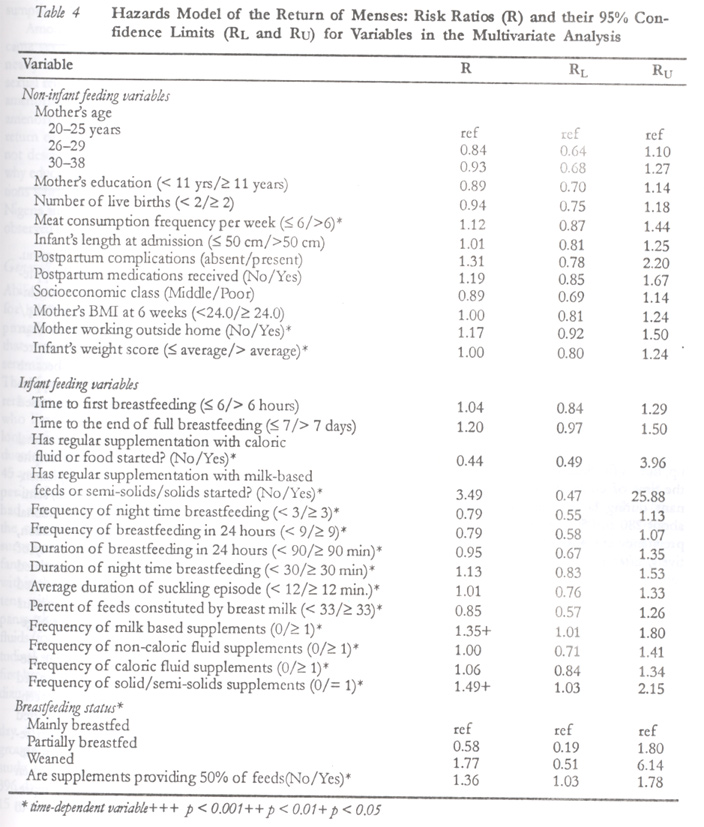
Upon admission, background characteristics of the mother, father and infant were obtained, including age, marital status, education, occupation, social class, ethnic group and place of residence, mother's medical, gynaecological, obstetric and family planning histories. Others were details relating to the birth, infant feeding pattern during the first 4–7 days postpartum, the infant's birth weight, infant's sex, mother's weight and height, diet and use of nutritional supplements. Follow-up interviews occurred in the mothers' homes every two weeks. Mothers completed a daily diary record chart of vaginal bleeding and infant feeding, and completed a detailed diary card of the time and duration of breastfeeds and the frequency and nature of other feedings once every two weeks. At the follow-up visits information was transferred from diary cards to follow-up data collection forms. Such information included summary of the infant feedings including all foods other than breast milk, breast expression, the use of pacifiers, and vaginal bleeding episodes. Mothers were asked about the number and type of maternal and infant illnesses and medications, family planning practice and coitus, maternal work patterns, number of cigarettes smoked per day, alcohol intake, frequency of maternal meat, fish, and chicken consumption per week, and maternal dietary supplements. At each visit the infant and mother were weighed. At every second visit the length of the infant, chest and head circumference were measured. The mother's nutritional status was assessed by measuring skin fold thickness of the biceps, triceps, subscapular and abdomen. To be defined as a breastfeeding episode, a breastfeed lasted at least two minutes and was separated from other episodes by at least 30 minutes. Three infant feeding categories were defined. “Full breastfeeding” is when the infant received only breast milk, vitamins/medicine, non-caloric fluids, and only “tastes” of other foods. During “partial breastfeeding” the infant could receive caloric supplements in amounts greater than tastes. When the infant was no longer breastfed the feeding category was designated “weaned”. All episodes of vaginal bleeding or spotting were recorded by the participants prospectively. The analysis ignored any bleeding associated with a gynaecologic procedure or within fourteen days of the end of lochia. A bleeding episode was defined as at least two consecutive days of bleeding per vaginum with at least one day requiring sanitary protection. If a bleeding episode was followed in 22–69 days by a second, confirming bleed or pregnancy, it was defined as the “confirmed first menses – HRP rule” (named after the WHO Human Reproduction Programme, which created the definition as a way to define the occurrence of a fertile or potentially fertile cycle). If a bleeding episode was not confirmed within the time limits, it was ignored, but only one episode could be so ignored. “All first menses – HRP rule” was the term for the confirmed first menses plus, for women who had one bleeding episode but discontinued the study before that episode could be confirmed, the first unconfirmed bleeding episode. When a woman perceived for the first time that her bleeding episode was characterised by the same or more blood loss than a pre-pregnancy menstruation, that episode was defined as the “woman's perception of the first menses”. The endpoints of the study were (1) the occurrence of two ostensibly normal menses, (2) the occurrence of a confirmed pregnancy, or (3) withdrawal from the study for any other reason. STATISTICAL ANALYSES Survival analysis was used to estimate the durations of breastfeeding and lactational amenorrhea.7 For the calculation of the duration of lactational amenorrhoea, cases were censored at weaning or withdrawal from the study, while for the duration of breastfeeding cases were censored at the return of first menses or withdrawal from the study. The 50th percentile of each distribution was taken as the summary index. Breastfeeding frequency, duration and the intervals between breastfeeding were calculated considering only women who were still breastfeeding and amenorrheic. Cox's non-parametric hazards regression analysis8 was performed to determine the variables associated with the duration of lactational amenorrhea. The duration of lactational amenorrhea, defined as the confirmed first menses – HRP rule, was used in the analysis. Eighty two variables – characteristics of infant feeding as well as the other variables about the mother and infant collected at admission and during follow-up – were considered for inclusion in the multivariate model. Variables were included in the model if, upon univariate analysis, they were related to the duration of lactational amenorrhea at p < 0.20 or if they were otherwise known to be biologically related to the duration of lactational amenorrhea. In this way, a total of 27 variables were selected for the final multivariate analysis. Modelling was done with the use of PROC PHREG of the software package Statistical Analysis System (SAS) Version 6.8 (SAS Institute, Cary, NC). The study was approved by the ethical committee of the Ogun State University Teaching Hospital and the World Health Organization Secretariat Committee on Research Involving Human Subjects. All women participating in the study gave informed consent. RESULTS Study Subjects Five hundred and twenty women were admitted into the study in Sagamu. The mean age of the infants at the time of admission into the study was 5.4 days. The study was completed by 420 women (81%) when they experienced two ostensibly normal menses (415) or when they became pregnant (5). Among the remaining women, 41 were lost to follow-up, 35 desired to withdraw from the study, 3 infants died, 2 women started a hormonal method of contraception, and 19 left the study for other reasons. Table 1 describes selected characteristics of the women in the study. The mean age of the women was 27 ½ years, and the mean number of years of education was 11.3. Ninety two per cent of the women described their ethnic group as Yoruba, 98% lived in an urban environment, and 99.8% were married. Thirty eight per cent were of lower socioeconomic class and 62% were middle class. Excluding the infant that they were breastfeeding, the women had an average of 1.9 live births, 1.8 living children, and apparently breastfed all of their previous children. None reported being a smoker, and 17% reported that they drink alcoholic beverages. Of the infants admitted into the study, 46% were female and 54% were male. Delivery occurred in a hospital or health centre in 91% of the cases, and 99% were vaginal deliveries. Complications during delivery were reported in 4% of the cases. Uterotonics were used before delivery in 9% and after delivery in 88% of the women (see Table 2). Nearly all of the women (98%) reported that they prepared their breasts for lactation during pregnancy. Nipple massage with oil was reported by 85%, and 5% said that they massaged the breast with a sponge. Inverted nipples were reported by 3%. Infant Feeding Practices Table 1 also shows that the women reported breastfeeding the previous child for a median duration of 10 months (mean = 10.3 months), and breastfeeding without supplements for only 1.0 months. The prospectively determined median duration of breastfeeding the current infant in this study was 13.0 months. Although it appears that mothers breastfed the index children longer than their previous infants, this current duration is clearly an underestimate, since the end of lactation is known for only 141 women. (Many infants were excluded from continued contribution to the breastfeeding duration lifetable when their mothers discontinued the study, usually due to the resumption of menses.) The reported median duration of lactational amenorrhea experienced when breastfeeding the last child was 6 months (mean = 6.9 months). In the current study, the median duration of lactational amenorrhea, calculated from prospectively collected data, was 6.7 to 7.7 months, depending on the definition of the return of menses used (Table 3). Figure 1 shows the type of infant feeding practiced by the women in the study by time postpartum (i.e., by follow-up number). At the first follow-up (which occurred at an average of 18 days postpartum) roughly one third of women were fully breastfeeding, and two thirds were partially breastfeeding, reflecting the practice of very early supplementation. Less than 1% of infants were weaned prior to the 13th follow-up (about six and 2 months), and by one year only 10.9% were weaned. Figure 2 shows the percentage of all feedings that were breastfeeding over time. Compared with the other centres in the study, the women in Sagamu reported the lowest proportion of all feeds as breastfeeding until almost nine months postpartum. However, as can be seen in the figure, the decline in the percentage of feeds that were breastfeeds was gradual, in fact the most gradual of all the centres. Figure 3 shows the types of supplements to breastfeeding given over time as a percentage of all feedings. Water and non-caloric fluids continued to be given at about the same level throughout infancy. A similar pattern is shown for caloric fluids except at about one third of the frequency of the non-caloric fluids. Milk/milk-based fluids increased dramatically as a percentage of all feeds in the first four months and just as dramatically declined again. Solid/semi-solid feedings comprised less than 1% of supplements for the first four months, and then their frequency increased dramatically. It appears that, beginning at about four months, solid/semi-solid feedings were substituted for milk/milk-based supplements. The mean frequency of breastfeeding in 24 hours over time is seen in Figure 4. The women reported breastfeeding 9.3 times per 24 hours (6.3 times by day and 3 times by night) at the first follow-up. This number had declined to 7.8 times by the 30th follow-up. As the mean frequency of suckling decreased, the mean longest interval between breastfeeding increased accordingly, from 273 minutes at the first follow-up visit to 338 minutes at the 30th follow-up visit (not shown). The mean duration (number of minutes) of breastfeeding in 24 hours is also seen in Figure 3. The mean duration gradually decreased from 111 minutes at the first follow-up to 96 minutes at the 30th follow-up. Compared with the other centres in this study, breastfeeding in Sagamu was a little below the middle in terms of frequency and duration at the start of follow-up and virtually at the middle of all the centres at the end of follow-up. The median duration of lactational amenorrhea in Sagamu was also in the middle of the seven centres, always ranked third or fourth out of seven, depending on how the return of menses was defined. However, compared with the other centres, the introduction of supplements was profoundly early in Sagamu. Return of Menses In the Sagamu sample of breastfeeding women, the confirmed first menses as per the HRP rule occurred at a median of 7.7 months or 234 days (95% CI = 215–255). The close concordance of the time of return of menses across the four definitions of the return of menses is illustrated in Table 3. Univariate analysis of the correlates of lactational amenorrhea yielded 27 variables (seen in Table 4) for the multivariate analysis. After considering all 27 factors simultaneously, only three proved to be significant at p < 0.05, namely, the absence of milk or milk-based supplements, the absence of solid/semisolid supplements, and the condition wherein less than 50% of the feedings are supplements. All three factors are associated with an increase in the duration of lactational amenorrhea. Postpartum Abstinence Table 5 presents a frequency distribution of the number of days from delivery to the first reported occurrence of sexual intercourse postpartum. The median time until the first reported intercourse was approximately four months, but this median could be substantially shorter than the mean since 148 women (28.5% of the total) did not resume sexual relations while they were in the study. This median represented 200% more days of abstinence than the centre with the earliest return to coitus and over 100% more days of abstinence than in most of the other centres. After sexual relations resumed, the Sagamu women who were sexually active reported relations in 81% of the fortnightly follow-ups, which was one of the lower rates among the centres. Among the 71.5% of the Sagamu sample who reported being sexually active, nearly all were still breastfeeding at the time that the first coitus was reported. Also, more than two thirds of the women were still amenorrheic at the time of the first coitus (see Table 5). The proportion amenorrheic at the time that coitus returned generally decreased over time, but so did the proportion of women who were amenorrheic. Contraception and Pregnancy The study protocol excluded women who intended to use hormonal methods of contraception after childbirth, and two women who started a hormonal method during follow-up were discontinued. Forty per cent of the women in the Sagamu centre started a non-hormonal method during lactational amenorrhea, with a mean starting time of 81 days (95%CI = 79–93). Of these women, 57% started using a barrier method and 30% used withdrawal. Five women became pregnant during follow-up, but all five had already weaned their children at the time of conception. Thus, none became pregnant during lactational amenorrhea. There were about 280 and 500 woman-months of exposure to pregnancy at 6 and 12 months postpartum respectively, after censoring for abstinence and contraceptive use. DISCUSSION The hallmark of the Sagamu centre in the multinational study in terms of infant feeding is the very early introduction of supplements and the regularity with which they were fed. Despite feeding infants other foods, women in the Sagamu study breastfed consistently, illustrating that supplementation was concomitant with only a gradual decline in breastfeeding frequency or duration and not with the termination of breastfeeding. Supplementation and breastfeeding appeared to be equally common aspects of infant feeding in Sagamu. However, the presence of milk/milk-based supplementation or solid/semisolid supplementation increased the risk of the return of menses. Solid/ semisolid supplements were introduced later than the other supplements, and may even have replaced milk/milk-based feeds as the child became older. When 50% of all feedings were supplements, the risk of the return of menses increased significantly. This study measured the duration of lactational amenorrhea with certainty and found that despite continued high levels of breastfeeding, supplementation with milk/milk-based feedings or solid/semi- solid feedings shortened the duration of lactational amenorrhea. Three measures of supplementation, and no other factors among a very large array of possible determinants are significantly associated with the return of menses among these educated women. This rate of the return of menses appears to be substantially earlier than among other Nigerian women. Although there was a profoundly longer median duration of postpartum abstinence reported in the Sagamu centre compared with the other centres in the multinational study, the median reported here is substantially shorter than the median reported in a large retrospective survey representative of women in Nigeria.6 Although women in the Sagamu sample may not have been representative of the community, the time of return to coitus reported here is also an underestimate. On the other hand, the study reported here was prospective and may have produced more valid data on postpartum abstinence than the retrospective survey, which required women to recall the resumption of coitus up to 24 months in the past. Among the 71.5% of Sagamu women who became sexually active when they were in the study, nearly all were breastfeeding when they resumed sexual relations, and most resumed relations during amenorrhea. Neither breastfeeding nor the state of amenorrhea appears to have been a barrier to the return of coitus in this sample. This research was not designed in a way to gain further insight as to why educated women in Sagamu resume sexual relations when they do, i.e., earlier than the usual time in Nigeria and later than in other cultures, such as those observed in the WHO multi-centre study. Generalisability of Findings Ability to read and write was required in this study for participants to reliably record information prospectively. This literacy requirement implied that women in the study might not be representative of the communities in which they lived. Therefore, Sagamu investigators undertook a “current status survey”9 of more than 2000 women who lived in the same areas as the women in the longitudinal study. Personal interviews were conducted with a random sample of women aged 15–45 years who delivered infants within a 24-month period. Indeed the women in the longitudinal study had about one to two years more education than the community women in the survey. Among the survey respondents, 96.8% reported that their infants consumed fluids other than breast milk within the first three days of birth, which is consistent with the 84% of longitudinal study participants who reported that their infants received other fluids/foods before the first breastfeed. In the longitudinal study the median hours from delivery to the first breastfeed were 10.5, which was close to the median value for the survey respondents. The median frequencies of breastfeeding per day (6) and per night (3) were similar in both groups of women. However, in the longitudinal study the median duration of breastfeeding was 396 days (about 13 months) as compared to about 15 months estimated from the survey data. While this difference underscores the fact that the longitudinal study underestimates the duration of breastfeeding due to the study methodology, that same methodology provides a rigorous estimate of the duration of lactational amenorrhea. The median duration of lactational amenorrhoea in the study was 234 days (about 7.7 months) while the estimate from the survey was about 11 months, which may contain some inflation due to recall problems. Nevertheless, it appears that the women in the longitudinal study who were better educated than the women in their immediate communities remained amenorrheic for fewer months. However, when placed in the perspective of the rest of Nigeria6, they are not very different from other urban women from the southwest with better education. Implications for Guidance on Infant Feeding and Family Planning Infant feeding, postpartum abstinence and postpartum contraception should continue to be closely examined for their effects on the reproductive health of women and on infant survival and nutrition. Contraceptive methods should be made readily available for use by postpartum women immediately on the return of menses or the regular consumption of caloric supplements by the infant. CONCLUSION Educated breastfeeding women in Sagamu, Nigeria, remained amenorrheic for seven months despite the early introduction of supplements. The early supplementation and early return of menses seen in this sample of women in Sagamu may herald the direction of future infant feeding practices and fertility in Nigeria. ACKNOWLEDGEMENTS This study was funded by the UNDP/UNFPA/ WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction. The report contains the collective views of an international group of experts and does not necessarily represent the decisions or the stated policy of the World Health Organization. The authors are indebted to the mothers (and babies) who gave so generously of their time to participate in this study. The principal investigators of the multicentre study were Shakuntala Bhatnagar, National Institute of Health and Family Welfare, New Delhi, India; Henry G. Burger, Prince Henry's Institute of Medical Research, Melbourne, Australia; Hernan L. Delgado, Institute of Nutrition of Central America & Panama (INCAP), Guatemala City, Guatemala; Olukayode A. Dada, Department of Pathology, Ogun State University, Sagamu, Nigeria; Barbara A. Gross, Department of Medicine, Westmead Hospital, Sydney, Australia; Yngve Hofvander, Department of Paediatrics, Uppsala University, Uppsala, Sweden; Pablo A. Lavin, Department of Obstetrics and Gynaecology, University of Chile, Santiago, Chile; Tang Guang-hua, Family Planning Research Institute of Sichuan, Chengdu, People's Republic of China. Data co-ordination and statistical analysis were performed by Olusola Ayeni, Alain P.Y. Pinol, Annie J.M. Chevrot, Milena Vucurevic, Vikram S. Nagi, UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland. The publication advisory committee to the multicentre study included Paul F.A. Van Look, and H. von Hertzen, UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, Geneva, Switzerland; Anna Glasier, Department of Obstetrics & Gynaecology, University of Edinburgh, UK; Peter W. Howie, Department of Obstetrics and Gynaecology, University of Dundee, UK; Kathy I. Kennedy, Family Health International, Research Triangle Park, North Carolina, USA; Jean-Christophe Thalabard, Unité de Pharmacologie Clinique, HCL, Lyon, France; Miriam Labbok, Institute for Reproductive Health, Georgetown University, Washington DC, USA This manuscript was prepared by Kathy I. Kennedy, Olusola Ayeni, Olukayode A. Dada, and Alain P.Y. Pinol. Inquiries and correspondence should be addressed to Paul F.A. Van Look and Helena von Hertzen, UNDP/UNFPA/WHO/World Bank Special Programme of Research, Development and Research Training in Human Reproduction, World Health Organization, 1211 Geneva 27, Switzerland. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02020f4.jpg] [rh02020f3.jpg] [rh02020f1.jpg] [rh02020t5.jpg] [rh02020t2.jpg] [rh02020t4.jpg] [rh02020f2.jpg] [rh02020t1.jpg] [rh02020t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}