 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 51-59 Extension Personnel's Sexual Behaviour and Attitudes toward HIV/AIDS in South-Western Nigeria Olugbenga Jelil Ladebo1 and Adewunmi George Tanimowo2 1Department of Agricultural
Extension and Rural Development, University of Agriculture, P. O. Box 2316,
Sapon, Abeokuta, Ogun State, Nigeria. E-mail: ladebo@unaab.edu.ng 2Lagos
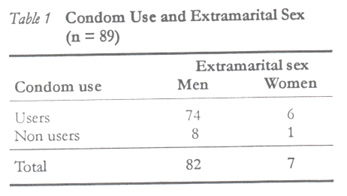
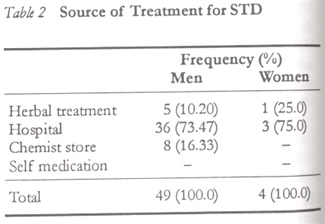
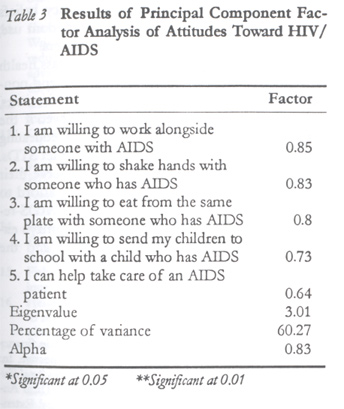
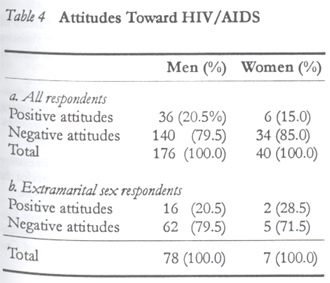
State Agricultural Development Authority (LASADA), Lagos, Nigeria. Code Number: rh02021 ABSTRACT This study examined the sexual behavioural pattern, knowledge and attitudes to HIV/AIDS of 216 extension personnel in south-west Nigeria. Information was obtained using a combination of structured interview schedule and focus group discussions. Results show that the extension personnel were young men and women, married, mostly Christians and educated. All the women had premarital sex, compared with 98.3% of the men, more men (46.7%) engaged in extramarital sex than women (18.4%), and 81.2% of the men were using condoms regularly, compared to 57.5% women users. All the respondents were fully aware of HIV/AIDS, while 79.5% of men and 85.0% of women expressed negative attitudes to HIV/AIDS. This has serious implications for the delivery efforts of focal extension agencies. (Afr J Reprod Health 2002; 6[2]: 51–59) RÉSUMÉ Comportement et attitudes sexuels envers le VIH/SIDA chez le personnel du service d'extension médicale au sud-ouest du Nigéria. Cette étude a examiné la nature du comportement sexuel, la connaissance et les attitudes chez 216 membres du service d'extension médicale au sud-ouest du Nigéria, envers le VIH/SIDA. Nous nous sommes renseignés à l'aide d'une combinaison du programme de l'entretien structuré et les discussions en groupe cible. Les résultats ont montré que le personnel du service d'extension étaient des jeunes hommes et des jeunes femmes mariés et en majorité des chrétiens et des gens instruits. Toutes les femmes ont eu des rapports sexuels avant le mariage en comparaison avec 98,3% des hommes. Plus des hommes (46,7%) se lancent dans des affaires sexuelles en dehors du mariage que des femmes (18,4%); 81,2% des hommes utilisaient régulièrement des préservatifs en comparaison avec 57,5% des femmes qui l'utilisaient. Toutes les personnes interrogées étaient tout à fait conscientes du VIH/SIDA. Ceci a de graves implications pour les tentatives de la prestation de la part des agences d'extension focale. (Rev Afr Santé Reprod 2002; 6[2]: 51–59) KEY WORDS: Sexual behaviour, attitudes, HIV/AIDS, extension personel, south-west Nigeria INTRODUCTION The village extension agent (VEA), as in other third world countries, is the primary source of agricultural information that smallholder farmers depend upon for production information in Nigeria.2,5,7,21,26 This grassroots extension worker forms the arrow head of the extension delivery efforts of the Agricultural Development Programmes (ADPs) in each of Nigeria's 36 states, and the Federal Capital Territory (FCT), Abuja. Generally, the ADPs were established to promote agricultural production and rural development. The VEAs perform specialised functions within the ADPs. At present the VEAs disseminate agricultural-related information and technical innovations to rural farmers. They teach farmers new skills on the use of technical innovations. The VEAs are also expected to send feedback information on farmers' needs and the farm environment to the extension agency and researchers. Generally, the VEAs assist rural people to find solutions to their day-to-day problems.7 With the reported epidemics of human immunodeficiency virus and acquired immune deficiency syndrome (HIV/AIDS) and its impact on agricultural productivity in Africa, experts are now advocating that extension agencies should be involved in the HIV/AIDS prevention efforts by educating the rural communities.32 Due to their developmental role(s), which is pertinent to boosting the country's agricultural production, the VEAs have been the object of research attention in recent times. This is with a view to unravelling the crucial factors that might make the VEAs more efficient as well as productive. Many of the studies, however, focused on factors that exert considerable influence on the motivation of agents. These include professional competencies of the extension agents6, supervisory effectiveness of extension agents24, organisational commitment of extension agents20, job satisfaction among extension agents3, gender of the extension agents as it affects farmers' access to and participation in extension21, and improving the functional effectiveness of the agents17. The contentious issue of funding the country's extension system has also come under scrutiny.1,4,27 Studies on sexuality of extension personnel that could be of major consequence for their health appear to be non-existent. The health status of the extension workforce is a critical element in work motivation and eventual productivity of the personnel.8 Research into the sexuality of VEAs is, therefore, imperative because of the nature of their work, which involves frequent travelling in the rural areas and sometimes living away from their regular sex partners. They may as a result get involved in multiple sex partnership, thus increasing their risk of being infected with HIV. HIV/AIDS is a health-related problem that has been strongly linked with the sexuality of an individual, and it could be a serious threat to the delivery of extension services to smallholder farmers in Africa. For instance, Spore reports that the extension services of Uganda, Zimbabwe and Ghana have lost more than 10.0% of their extension personnel to AIDS-related deaths.12 The disease affects sexually active adults who are coincidentally in their prime productive and reproductive years. Nigeria, like other developing countries, is characterised by high food prices and food insecurity. The economy is greatly dependent on rural extension as a viable option for increasing the productivity and production of the smallholder farmers, who dominate its agriculture. However, the provision of optimal extension service in the country is being hampered by low staff morale, inadequate funding of the ADPs and insufficient number of extension personnel.5,27 The high prevalence of HIV/AIDS is likely to compound the problems associated with extension delivery in the country. At present, an estimated 2.6 million adult Nigerians aged 15–49 years are seropositive. It has been projected that by 2003 4.9 million Nigerian adults will test positive to the human immunodeficient virus (HIV). The devastating impact of the disease has implications for the socioeconomic status of the nation, which includes increased budgetary allocation to medical care, depletion of the manpower base due to AIDS-related deaths and, generally, a decline in economic growth.14 The disease prevalence has no territorial exclusivity, since it has been reported in both urban and rural areas. There has been a general increase in the prevalence rate of the disease from 1.8% in 1990 to 4.5% in 1995 and to 5.4% in 1999. With this rather grim picture, it appears that no institution in the country can possibly claim immunity from the disease, since all institutions employ individuals who most likely engage in heterosexual intercourse, which is the commonest mode of transmission of the disease in the country as elsewhere in Africa.10,14 Since the ADPs represent an important institution in the country this study, therefore, examines the sexual behavioural pattern, knowledge and attitudes of extension personnel towards HIV/AIDS. METHODOLOGY Study Sample Due to the low financial support for the study only the Lagos and Ogun States ADPs (LASADA and OGADEP) were selected for the study out of the nation's 36 ADPs. The two states are contiguous to each other. Operational activities of the ADPs cover both rural and urban areas of the state. Both states are situated in the south-western part of the country. For operational purposes, the ADPs have four zones with a zonal manager (ZM) heading each zone. Each zone consists of six blocks, which are supervised by block extension supervisors (BES), and eight cells constitute a block. Furthermore, each of the cells is made up of eight or more villages. Male extension agents at the village levels are designated as village extension agents (VEAs), but the female workers (block extension agents [BEAs]) operate at the block level mostly with groups (and some individual) of women farmers. At the zonal levels are the subject matter specialists (SMS) for livestock, crops and fisheries, etc. The personnel reside within the operational site, but some have their families located in major towns or urban centres, who they visit during weekends or during public holidays and festivals. With the exception of the subject matter specialists who must possess a master's degree, the minimum educational requirement for extension agents is the ordinary national diploma (OND). In this study, the observed minimum educational qualification of extension personnel is the higher national diploma (HND) or bachelor's degree (B. Sc). A census of extension personnel of ADPs in the two states was undertaken. Questionnaires were administered on 63 extension personnel from LASADA (3 ZMs, 12 SMS, 15 BEAs, 4 BES and 29 VEAs) and 196 from OGADEP (4 ZMs, 20 SMS, 20 BEAs, 20 BES and 132 VEAs). Completed questionnaires were returned by 45 (71.4%) (1 ZM, 8 SMS, 12 BEAs, 4 BES and 20 VEAs) LASADA personnel and 171 (87.2%) (2 ZMs, 14 SMS, 20 BEAs, 18 BES and 117 VEAs) OGADEP personnel. The total response rate is 83.4% (216). The 16.6% non-response was due mainly to the non-inclusion of poorly completed questionnaires in the analysis; some personnel also could not fill their questionnaires due to work pressure at the time of data collection. Data Collection Data were collected through focus group discussions and structured questionnaire administration. Questionnaire administration was done during the fortnightly training sessions of the extension personnel at OGADEP, while the LASADA personnel were interviewed during pre-season training exercise. Attendance at the fortnightly and pre-season training sessions is compulsory for all extension personnel. Individual questions and observations made by the extension workers were attended to by the researchers. Discussions were conducted with extension personnel in groups of not less than five persons of the same gender. Discussions were held with personnel in gender homogenous groups to overcome gender bias and allow for proper self expression, which may not be possible with the presence of the opposite sex. Study Variables The following variables were examined in the study: (a) Personal information on the respondents including age, marital status, religion, family size and educational attainment. (b) Premarital sexual behaviour. (c) Extramarital sexual experience — defined as having sexual relationship with a person other than the regular partner or spouse. Having multiple sex partners is believed to play a significant role in the transmission of HIV/AIDS in Africa and elsewhere. Focus group discussions were employed to complement the questionnaire on the issue of extramarital sex. This was deemed necessary due to the sensitivity of the question, which could result in under-reporting of respondents' actual behaviour. During the focus group discussions, respondents were tactfully asked if they “play the field or play friendly matches” and their responses indicated in their questionnaires. (d) Condom use — it is believed that condom use decreases the risk of HIV and STDs transmission during intercourse.30,31 Condom use among the respondents was investigated either as a family planning device or to prevent unwanted pregnancies and infection with STDs including HIV in casual sexual relationships. (e) The practice of “dry and tight vagina” — information were elicited from respondents on whether they practised “dry and tight vagina”. Dry and tight vagina is a common practice in Benin, Cote d'Ivoire, Central and Eastern Africa (most especially Zaire, Malawi, Zambia and Kenya) and appears to be a possible risk factor that could predispose both men and women to infection with HIV.10 Certain intra-vagina substances are inserted into the vagina before intercourse to make the vagina dry as well as tight. Achieving dryness and tightness of the vagina during sexual intercourse is believed to increase sexual pleasure and satisfaction for both partners. However, the practice also produces undesirable side effects, which include itching, swelling and lesions of the vagina and uterine cervix membranes.9 Brown and associates observed that the most common methods employed in the practice include the use of leaves (Alchornea condifolia, Ocimum gratissimum, Cucurbita maxima, Hibiscus mechovii, Combretum sp and Mitragyna rubrostipulata, etc), powders, stones, pharmaceutical products (talcum powder, Vicks, and hydrolin and gyno-sterazin), wiping cloth and hot water.9 Though the practice of dry sex has not been formally reported in Nigeria, it was hypothesised that since it can be found in Benin Republic and Cote d'Ivoire10, neighbouring countries to Nigeria, the practice could have diffused into the country through cross-border migrations and international trade in recent time. While the male respondents were eager to discuss the topic of “dry and tight vagina”, the female extension personnel were less enthusiastic about the issue and most of them did not respond to the question. Due to the congenial atmosphere that prevailed during the survey exercise, and while in the all-female group, most of the female agents gave suggestions/reasons that may discourage them from practising dry and tight vagina. It was observed that if the vagina is too dry during intercourse, sexual exercise could be very painful and both the penis and vagina would be traumatised. Respondents agreed that a traumatised vagina is a high risk for contracting HIV/AIDS. Some of the female agents wondered why a man would insist that his woman be dry when the wetness of the vagina is part of the physiological makeup of a woman. They feel that no man has any justification to insist on dryness because it will be most traumatic to the woman. However, a few of the female agents said some women produce excessive vagina secretion during intercourse, and such women are sometimes advised to wash their vagina with alum before having intercourse. (f) Awareness of and infection with STD — correspondents agreed that STDs, especially those that are associated with genital ulcers may increase the risk of transmission of HIV. Previous infection with STDs associated with genital ulcers may facilitate the entry of HIV into the bloodstream.10,16,31 In view of this, the study also investigated whether respondents had been infected and treated for STDs in recent times. (g) The practice of anal sex and sex during menses — these practices are associated with higher risks of infection with HIV. In the United States of America, anal sex has been linked with sero-conversion between both homosexuals and heterosexuals.10,29,23 (h) Knowledge of and attitudes to HIV/AIDS — was assessed using a five-item adaptation of Stipp and Kerr scale.34 The Stipp and Kerr scale measures attitudes toward HIV transmission. Agreement with any of the items attracted a “Yes” response (1), while disagreement was given a “No” score (2). Minimum scores of five signify positive attitudes while scores ranging between six and 10 indicate negative attitudes to HIV/AIDS. Attitudes are indicators of a person's latent tendencies to respond to stimuli that are present in the environment. It can be employed to describe and explain the behaviour of the individual. A characteristic of attitudes is its persistence, i.e., it tends to persist over time unless there is a significant effort to change it.23 For instance, an extension worker who has positive attitudes about HIV/AIDS transmission is the one who has been able to reconcile his knowledge of transmission of HIV/AIDS and the reality of his personal safety when in contact with sero-positive individuals. Such an extension agent is more likely to work along a sero-positive co-worker or farmer. However, an agent who is less positively disposed in attitude to HIV/AIDS will find it more difficult working with a HIV infected co-worker or farmer despite the overwhelming evidence that transmission of the HIV is impossible by casual contact with infected individuals. The consequence is that the congenial and harmonious atmosphere that exists in the work environment of the extension agency will be jeopardised. Likewise, the unwillingness of the extension worker to interact with an HIV positive farmer and members of his household has negative implications for the credibility and performance of the extension service. On the bright side, an extension worker with a negative attitude to the transmission of HIV may suffer from fear of contracting HIV and consequently abstain from all behavioural acts that may put him/her at risk of contracting the disease. Data Analysis The dimensionality of the attitude scale was determined by subjecting the scale to principal component factor analysis.35 Obtained results could not be rotated since only a single factor was produced. This signifies that the attitude scale contains a single dimension, i.e., the items of the scale actually measure the same trait. Internal consistency reliability (Cronbach alpha) for the scale was 0.83. Finally, data were ordered and described using relative and absolute frequencies, means and mode as well as qualitative analysis. FINDINGS Personal Characteristics The extension personnel in the study were made up of 176 (81.4%) males and 40 (18.5%) females. Mean age for the men was 36.3 years while that of the women was 33.3 years. Most of the personnel were married (76.1% men and 82.5% women) and Christians (70.4% men and 75.0% women). The modal family size was one to three persons (54.5% men and 60.0% women), while the majority possessed either HND or B Sc. degrees (76.1% men and 72.5% women). Only 9.7% men and 22.5% women had M Sc. degrees, others were OND degree holders. Sexual Behaviour Premarital sex All the women (40) reported having had premarital sex, compared with 98.3% of the men. All the women had premarital sex with their boyfriends, while 97.2% of the men had it with their girlfriends, but 1.1% of the men claimed to have had premarital sex with commercial sex workers. Premarital sex is not an uncommon practice in south-west Nigeria19,28,36 and indeed in Africa.33 Extra-marital sex Ninety four per cent of the men were having sex with either regular partners (girlfriends) or spouses, while 4.5% were not engaged in any form of sexual activity because as practising Christians it is forbidden to have sexual relationships outside marriage. Ninety five per cent of the women were having sex with regular partners (boyfriends) or spouses, while 5.0% declined to comment. However, 18.42% (7) of the women currently having sex reported engaging in extramarital sex presumably with older men. None of the women having extramarital sex admitted it during focus group discussions. This may be due to the society's disapproval of the practice. Therefore, those women who involved in extramarital sexual relationships tried to avoid the stigma attached to such behavioural acts and instead opted to indicate their response in the survey schedule. This group of respondents cited reasons other than economic for engaging in extramarital sex. Sexual pleasure was given as the motive for involving in such behavioural acts. The proportion of those involved in extramarital sex was higher among the men, 46.7% (82). Men having extramarital sex claimed preference for students, young workers and sometimes older women and the motives for such acts included having additional pleasure and variety. The men believed that it could be sexually boring having only one partner and, besides, having multiple partners may confer certain prestige on the man among his friends. This finding reinforces the notion that the Yoruba of south-west Nigeria tend to be more permissive of male and female infidelity.28 The practice of extramarital sex among the study sample may be a reflection of the breakdown in values and the permissive attitude of the society. This study result is similar to those of Schopper and associates.33 Condom use All the respondents were aware of the condom. Eighty one per cent (143) of the men, compared with 57.5% (23) of the women, were using condoms regularly. Among those involved in extramarital sex, 89.7% (74) of men and 85.7% (6) of women were using condoms to prevent unwanted pregnancy and infection with STDs/HIV. Significant association exists between condom use and involvement in extramarital sex (chi-square = 0.07, degree of freedom 1) (Table 1). This implies that most of the agents who engage in extramarital sex use the condom. In particular, women having extramarital sex said they always insist that their casual partners use the condom. Users of condoms gave insight into the various grades of condoms that are available in the market. These include the high grade condoms, which make sex feel much more natural. However, non-users of condom explained that condom makes sex less stimulating and unsatisfying. Similar results have been reported by other studies.18,22,25 The practice of “dry and tight vagina” Some of the women admitted preference for tight vagina that is adequately lubricated to avoid “tears and injury” during intercourse. Putting in effort at making the vagina tight is meant to satisfy their partners as well as achieve personal satisfaction. Similar sentiments were expressed by 54.0% of the men, who preferred their partners to be tight but sufficiently lubricated to avoid excessive friction and injury during intercourse. However, few of the men expressed indifference to the issue. Others felt that “dry and tight vagina” is simply unimportant to them. Both male and female personnel who practised “tight but adequately lubricated vagina” explained the procedures commonly employed to do it as follows: (1) washing the vagina with alum before sexual intercourse; (2) constant washing of the vagina with water in-between sexual intercourse; (3) wiping the vagina with dry cloth/towel before and after sexual intercourse; and (4) minimal foreplay and early penile penetration before the woman gets sufficiently wet. None of the respondents was involved in anal sex or having sex during menses. Awareness of and infection with STDs All the respondents easily identified HIV/AIDS and other STDs. STDs that were identified by the extension personnel include gonorrhoea (96.0% men compared with 100.0% women), syphilis (87.5% men against 92.5% women) and herpes (61.9% men versus 60.0% women). Four women (10.5%) reported having been infected with STD before, compared with 27.8% (49) of the men. During group discussion, some of the men said there is nothing wrong with a man contracting STD. They believed it is evidence that they are sociable and popular with women. As shown in Table 2, 73.5% (36) of the men and 75.0% (3) of women who reported infection with STD sought for and were treated successfully at the hospital. Ten per cent of the men and 25.0% (1) of women received herbal treatment. Significant association exists between STD infection and treatment source among the sample (Chi-square = 1.37, degree of freedom 1). More men and women who contracted STDs sought for treatment at the hospital. Nevertheless, respondents refused to indicate whether they were infected through their regular partners, spouses or casual sex partners. Attitude towards HIV/AIDS All the respondents were aware of HIV/AIDS. No variation was observed in the level of awareness among the genders. Identified principal sources of information for the respondents were radio (100.0%), television (95.5%) and newspapers (79.5%). Less common sources of information include friends (46.4%), relations and farmers (44.6%). The respondents identified sexual intercourse as the main mode of transmission of HIV. Other perceived modes of transmission were needle sharing among drug users, maternal transmission, and transfusion of infected blood. Likewise, no variation was observed in the level of knowledge of the mode of transmission of HIV/AIDS among the genders. High level awareness and knowledge of HIV/ AIDS transmission exhibited by the extension personnel may be the result of the efforts of the two extension agencies at incorporating HIV/AIDS into the regular agricultural training schedule of their staff. In fact, at the time of the survey, HIV/AIDS formed part of the subjects taught at the regular training meetings witnessed by the authors. Respondents' attitudes toward the transmission of HIV were assessed due to the significant impact of a person's attitudes vis-à-vis his/her behaviour. Table 3 shows the result of the principal component factor analysis of the attitude scale to determine its dimensionality. Only a factor emerged, which explained 60.3% of the variance in the data of the respondents. The uni-dimensionality of the attitude scale indicates that all the items relate to the transmission of HIV. Therefore, summing scores on the five items constructed an additive index for each of the respondents. A score of five indicates positive attitudes to HIV, while scores ranging from 6 to 10 shows varying degrees of negative attitudes to HIV/AIDS. Study results show that 79.5% and 85.0% of the men and women respectively had negative attitudes to HIV/AIDS (Table 4A). These proportions of extension personnel might find it difficult working, or actually avoid any form of interaction, with sero-positive persons both at the workplace and in the field. Interestingly, among those having extramarital sex, 79.5% (62) of the men, compared with 71.5% (5) of the women, had negative attitudes toward AIDS (Table 4B). One would have expected that these sets of respondents would abstain from sexual behaviours that could put them at risks of sero-conversion. Results also show that these respondents actually used the condom. Condom use may give them a feeling of invulnerability to the disease. CONCLUSIONS The study respondents constitute a sexually active group. Some of the respondents appear to fall within the high-risk group, judging by their sexual behaviours or practices. Firstly, some of the extension personnel (46.7% men and 18.4%women) were involved in extramarital sex. To minimise the risks of contracting STDs/HIV, condom use was prevalent among those involved in the act. However, both users and non-users of condom having extramarital sex certainly constitute a high risk group, because it has been noted that condom use is not a full guarantee against HIV infection. It only reduces the risk of infection; the safest precaution against infection being total abstinence or adherence to a single sex partner by both parties.13 Secondly, all the extension personnel were fully aware and had sufficient knowledge of STDs/ HIV/AIDS, but few of the women (4) and sizeable proportion of the men admitted having contracted STD before. Most of those who had been infected with STD sought for treatment at medical centres, while few of the men (5) and women (1) had herbal treatment. Some of the respondents (both men and women) expressed preference for “tight but a lubricated vagina” during intercourse, which is a variant form of “dry and tight vagina” reported by Brown and associates.9 The methods employed for achieving the tight but moist vagina include washing with alum, mopping with wet piece of cloth, penile penetration before the vagina becomes sufficiently moistened, etc, could have adverse effects on both the vagina and penis during coitus. Findings show that the studied extension personnel would benefit from health education that is aimed at eliciting behavioural change. Most notable among the educational strategies is the information-motivation-behavioural skill (IMBS) developed by Fisher and Fisher15, which received empirical support from the study by Carey and associates.11 To optimise behavioural change in an individual the IMBS model specifies that (a) focal subjects must be provided with adequate information on HIV/AIDS transmission and prevention; (b) motivating the subjects to reduce HIV/AIDS risks. This involves building a commitment to change and assisting the subjects to develop an appreciation of the need for change of behaviour; and (c) teaching the behavioural skills for effective performance of the specific acts involved in risk reduction. Behavioural skill development should focus on self-management skills and sexual assertiveness training. Subjects are to be encouraged to (i) buy, keep and use condoms; (ii) identify high risk situations; (iii) attempt to alter cognition related to behaviour change by strengthening efficacy beliefs and countering negative attitudes to condom use; and (iv) negotiate condom use with partners. Though there has been tremendous mass health education sponsored by the government and non-government organisations (NGOs) in recent times, a lot more is needed and would be achieved if the extension agencies intensify efforts at educating their personnel about HIV/AIDS and other STDs. It is necessary for the agencies to conserve their human resource base, since they cannot afford to have their personnel depleted through AIDS-related deaths. It is well known that the country's extension system is insufficiently staffed and the farmer-extension ratio grossly low.5,27 REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02021t3.jpg] [rh02021t1.jpg] [rh02021t4.jpg] [rh02021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}