 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 60-70 Sexuality, Contraceptive Choice and AIDS Awareness among Nigerian Undergraduates AO Arowojolu, AO Ilesanmi, OA Roberts and MA Okunola Obstetrics and Gynaecology Department,
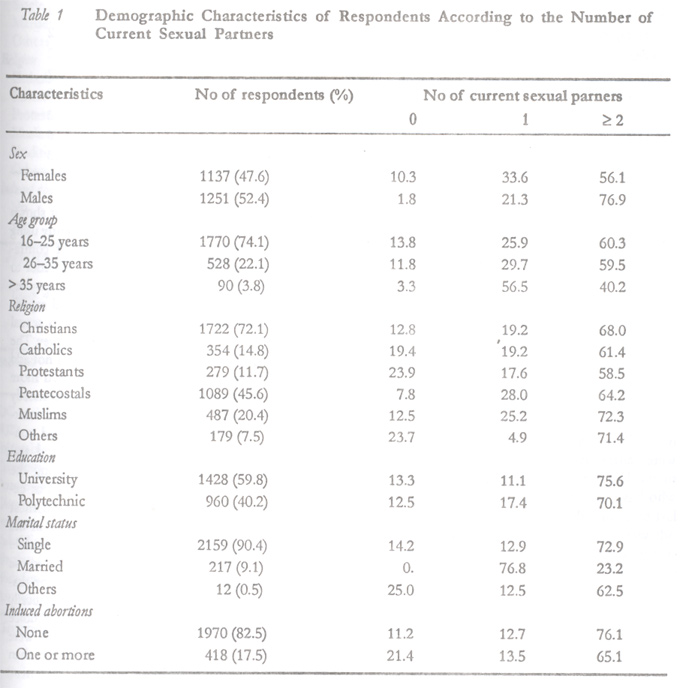
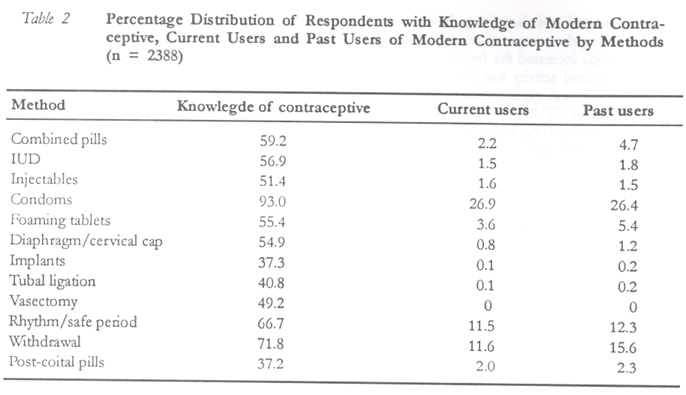
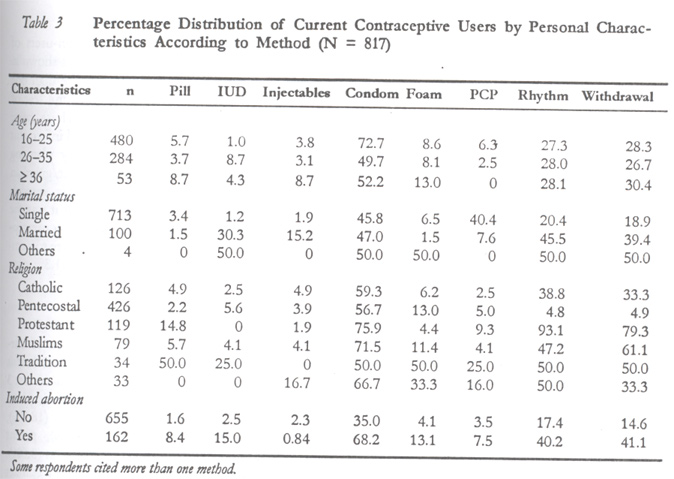
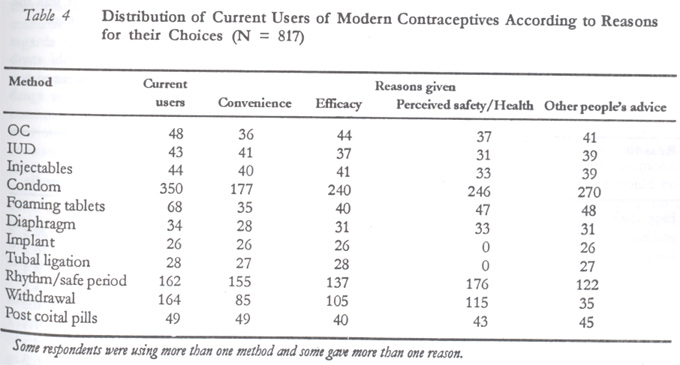
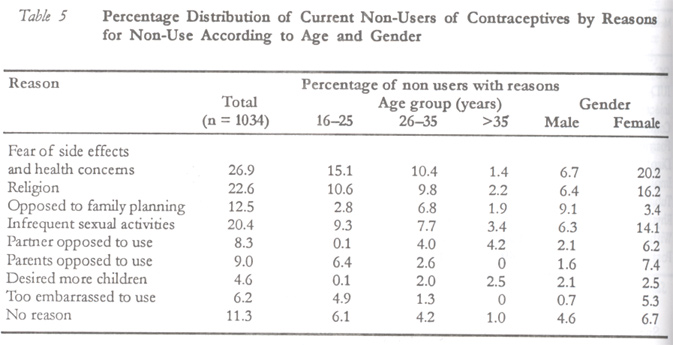
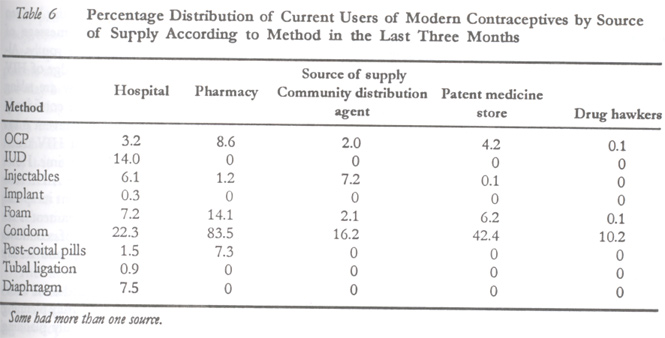
University College Hospital, Ibadan, Nigeria. Code Number: rh02022 ABSTRACT A survey of 2388 Nigerian undergraduates revealed that 87% were sexually active and 66% had more than one sexual partner, while 17.5% have had clandestine abortions. All respondents were quite knowledgeable about HIV/AIDS but few sexually active ones took precautions to prevent HIV transmission. Majority (87.5%) were knowledgeable about contraception and approved of its use, but only 34.2% were current users of contraceptives. About 58% of these cited pharmacy shops as their source of contraceptives. The attitudes of the students were below expectation. Specially designated centres for the provision of appropriate contraceptive services to students by trained personnel are needed in the institutions in order to tackle their reproductive health problems. (Afr J Reprod Health 2002; 6[2]: 60–70) RÉSUMÉ Sexualité, choix de contraceptif et la prise de conscience du SIDA chez les étudiants universitaires. Une enquête menée sur 2388 étudiants universitaires a révélé que 87% étaient sexuellement actifs dont 66% avaient plus d'un partenaire sexuel, alors que 17,5% se sont faits avorter clandestinement. Tous les répondants s'étaient bien renseignés sur le VIH/SIDA, mais quelques-uns qui étaient sexuellement actifs prenaient des précautions pour prévenir la transmission du VIH. La majorité (87,5%) s'étaient bien renseignés sur la contraception et ont approuvé son usage; mais seuls 34,2% étaient actuellement des usagers. Environ 58% d'eux ont déclaré qu'ils achetaient leurs contraceptifs à la pharmacie. L'attitude des étudiants était au-dessous de toutes espérences. Il faut des centres spécialement construits pour fournir des services de contraceptif aux étudiants, services qui seront assurés par un personnel formé pour s'occuper des problèmes de leur santé reproductive. (Rev Afr Santé Reprod 2002; 6[2]: 60–70) KEY WORDS: Sexuality, contraception, AIDS, youths, Nigeria INTRODUCTION Pregnancy and sexually transmitted diseases among youths continue to be a public health problem of immense concern in developed and developing countries.1-5 Most of these pregnancies are unplanned and unwanted. They are often terminated illegally by charlatans in secrecy. About 500,000 clandestine abortions took place in Nigeria in the1980s, some of which had disastrous consequences for the abortion seekers.6-10 It is evident that increased sexuality among youths would be responsible for increased unwanted pregnancies and subsequent clandestine abortions.2,11-14 Therefore, counselling and use of modern contraceptives should prevent the sequelae of these abortions.6,8,15,16 Furthermore, indiscriminate sexual intercourse exposes youths to the risk of sexually transmitted diseases especially where it involves multiple sexual partners.9,11,12 The implications of this is far-reaching, considering the several complications of STDs especially AIDS. Heterosexual transmission accounts for as high as 90% of HIV/AIDS in sub-Saharan Africa17, where about 14 million people were estimated to be infected with HIV.18 In Nigeria, evidence suggests that about one million HIV infected people exist, this prevalence is increasing due to high risk sexual behaviours.19,20 While the knowledge of AIDS as an incurable disease is high among Nigerians in general, AIDS transmission reduction measures are inconsistently taken among sexually active individuals.20 This is more so among the adolescents and youths20,21, who have an increased risk of infection with STDs. About half of all HIV infections occur among individuals younger than 25 years worldwide.22 The risk of HIV infection is especially high among those with multiple or risky sexual partners and who engage in unprotected sexual intercourse.23,24 Several studies have shown that young people lack knowledge about prevention of STDs and contraception, and often have erroneous ideas about reproduction.25 The implication of this for the future generation is alarming. Therefore, the government and non-governmental organisations in Nigeria have intensified their campaign against HIV transmission by way of public enlightenment and distribution of condoms. Previous studies have reported an increase in the use of condoms among adult Nigerians, but it is doubtful if such response occurs among youths.20 It is worthwhile to determine if the anti-HIV/AIDS campaign has got through to the youths at the moment. The lower age limit for admission into most Nigerian higher institutions is 16–17 years. This means that majority of undergraduates are in their late teens and early twenties. Most of them live away from home in school hostels or rented apartments close to their institutions. These arrangements weaken parental control and supervision of students' activities. They are often exposed to influences that encourage casual sexual relationships and have to take personal important decisions about their social and reproductive lives. These include decisions about sexuality and contraceptive use. Unfortunately, the use of contraceptives among Nigerian youths is poor due to the fear of side effects and the negative cultural attitudes of parents/guardians to contraceptive use.2,26,27 Various other factors are responsible for the unmet needs of the youths. These include the role of gatekeepers in facilitating or hindering their access to reproductive health services, the judgemental attitude of providers when they serve the youths and the poor organisation of services designed to meet youths' needs.27-29 Sexuality education is not part of the secondary schools' curriculum in Nigeria. There are no obvious policies in most Nigerian higher institutions on the provision of reproductive health services, including contraceptives to the students. Most of the health institutions on the campuses do not have specially designed facilities where students can obtain necessary advice on contraception to enable them to make informed choice in confidence. In fact, there is no official monitoring of the contraceptive methods that require some form of interaction with the health system. Therefore, contraceptive behaviour by the undergraduates is private and most often inconsistent. This study was performed to understand the sexual behaviour and contraceptive practice among Nigerian undergraduates as related to their awareness of HIV infections. This information should serve as basis for policy formulation on the current contraceptive needs and prevention of HIV transmission in the country. METHODS This survey was carried out among students in the University of Ibadan; University of Lagos; Ogun State University; Lagos State University; The Polytechnic, Ibadan; Lagos State Polytechnic and Ogun State Polytechnic, all of which are located in southwestern Nigeria. The Universities of Ibadan and Lagos are federal institutions and have the whole of the country as the catchments area for admission while Lagos and Ogun State Universities and all the polytechnics are state-owned (this means that majority of the students originate from the states). There were about 40,000 female and 100,000 male students in the institutions. We chose these institutions because they have the largest number of student population in southwestern Nigeria and because of their easy accessibility. The study was limited to the southwest for logistic and financial reasons but we believe that the population is representative of all students in the country's higher institutions and shows an impressive religious mix in the country. The institutions are situated in urban centres but lack specially designated reproductive health clinics on the campuses. Following a focus group discussion involving ten undergraduates from the University of Ibadan, a self-administered structured questionnaire was posted to a random sample of 3,000 students in the six institutions. The sample size was calculated to be 2432, assuming a 25% non-response rate and that 95% of the students are aware of contraception and HIV. The precision was 0.01, Z = 1.96 and p = 0.05. The sample respondents were selected from each institution following a two-stage stratified cluster sampling design. At the first stage, a random sample of clusters (halls of residence in institutions or departments in those where majority lived off campus) was selected with standard probability proportional to size. In the second stage, the blocks of residence or lecture theatres were listed and then systematically selected. An initial pilot study was performed before a final questionnaire was developed. The questionnaire included 30 close and open-ended questions addressing the students' demographic characteristics, knowledge and practice of specific modern contraceptive methods, sexuality and knowledge of fertile periods, pregnancies, abortions and sexually transmitted diseases. The data were coded and entered into a computer using EPI-INFO software (CDC Atlanta, Georgia). Results are included in simple percentages, descriptive measures and Chi square tests. Cross tabulations and correlation analysis were performed to establish relationships among variables. RESULTS Demographic Characteristics The response rate was 79.6%. The demographic characteristics of the students sampled are shown in Table 1. Of the 2,388 respondents, 52.4% were males and 47.6% were females. The gender of the respondents was about evenly distributed but there were more females than males among the polytechnic students. Majority (74.1%) were aged between 16 and 25 years, 22.1% were between 26 and 35 years, while only 3.8% were above 35 years of age. Christians constituted 72.5%, Muslims 20.4%, while 4.5% adhered to traditional religions and 3.0% had no religion. Most of the respondents were single (90.4%) and in the universities (59.8%). Knowledge of Fertile Periods and Prevalence of Sexual Activities Eighty seven per cent of the respondents were sexually experienced while 17.5% have had clandestine abortions before. These were uninfluenced by gender, school location or religious affiliation, but the proportions increased with the age of respondents. The mean age of sexual debut was 16.8 ± 2.6 years. Among the sexually active, 66% had concurrent relationship with more than one sexual partner (Table 1). This was more among the males than females (77% vs 56%). The females were likely to have relationship with older partners (workers, graduates, businessmen or older undergraduates) than their male counterparts who were more likely to have relationships with younger partners (not shown). Few respondents (22.6%) dated their classmates. The females gave reasons such as monetary gains, security of future marriage and maturity and understanding shown by older partners for their choice. On the other hand, the males indicated that younger persons were malleable, inexpensive, require no commitment, less demanding and less difficult to deal with. Eighty two per cent of the unmarried sexually active respondents were more likely to have sexual intercourse at weekends, during holidays or at safe periods. The frequency of sexual intercourse was higher among married respondents, ranging between two and three times a week and also among those living off campus. Among the unmarried respondents, multiple partnerships increased the frequency of sexual intercourse. Sexual activity was less during school examinations. Sexual experience was unrelated to the knowledge of STDs prevention strategies (including HIV and AIDS) because similar number of respondents had a good knowledge of the diseases. About half of the respondents (48.8%) could identify the fertile period — 20.2% cited the first week after menses, 12.4% cited the week before menses, 2.2% cited the menses period, while 16.4% were uncertain. More females (29.7%) correctly identified the fertile period than the males (19.1%). Correct identification of fertile period increases with age and it is positively related to the marital status and level of education. Knowledge and Use of Contraception About 87.5% of respondents approved of contraception, although all of them knew at least one method of contraception. Approval of contraception was highest among the 16–25-year-olds (92.8%) and the university students (90.2%). This approval of contraception was similar in both males and females. Condom (93%) and withdrawal method (66.7%) were the most known contraceptive methods (Table 2). Less than half of the respondents had knowledge of implants, tubal ligation, vasectomy and post-coital pills. Also, less than half of the respondents (38.1%) had ever used or were currently using (34.2%) a contraceptive method. (Current contraceptive users were those who have used a contraceptive method within the last three months). Condom and withdrawal methods were most popular methods ever used or currently used by the respondents. Among the current users, 18.9% had been on contraceptives for less than one year, 21.6% for 1–2 years, 8.6% for 3–4 years, 5.8% for 5–6 years and 4.6% for six or more years. Table 3 shows the associations between current contraceptive use and personal characteristics, including previous clandestine abortions. Diaphragm, implants and bilateral tubal ligation are not shown because very few respondents were currently using them. By current use we mean the use of contraceptives within the last three months in order to account for method switching by some respondents on account of frequent casual sexual experiences or non-use of contraceptives due to sexual abstinence in the month preceding the survey. The method mix distribution in this table does not add up to 100 because some respondents cited more than one method. These methods were mostly those useful only during the act of sexual intercourse or immediately after. They included condom, foam, diaphragm, withdrawal method and post-coital pills. The method mixes among the sexually active respondents differ sharply. For example, condom and post-coital pills were most popular among the 16–25-year-olds, those in the 26–35 years age group relied more on IUD while those over 35 years of age were more likely to use oral contraceptive pills, injectables, foam or diaphragm. These associations were not statistically significant. Religion had no influence on the choice of contraception. Those in the universities were more likely to use a form of contraception than those in the polytechnics. Switching between methods of contraception was common. About 80% of contraceptive users had used more than one method within the year of study. Most switching involved withdrawal method, condom, post-coital pills and oral contraceptive pills. This was most common among the 16–25-year-olds and least among those over 35 years of age. The principal reasons given for switching were fear of side effects, convenience and failure to take the usual contraceptives at the right time or unavailability of the contraceptive method of choice. Sexual partners had limited influence on the choice of methods except the condom. Dual method use was common among users of condom, foam, withdrawal method, post-coital pills and rhythm. These methods were used in various combinations. Dual method use was most common among 16–25-year-olds and single polytechnic students. Reasons for Choice of Contraceptive Method The response to the question on the principal reasons for the choice of contraceptive methods currently in use is shown in Table 4. A respondent to this question could give more than one reason for each method he or she was using. The commonest reason was efficacy. This was closely followed by perceived safety or health reasons. Other reasons included advices from other persons (including health workers) and convenience. The responses show that majority were more interested in efficacy and safety of the contraceptive methods than convenience or prevention of sexually transmitted disease. Reasons for Non-Use of Contraception Percentage distribution of current non-users of contraceptives by reasons for non-use is shown in Table 5. A respondent could give more than one reason. The commonest reasons were the fear of side effects and health concerns. These were closely followed by religious beliefs and infrequent sexual activities. Opposition to family planning either individually or by partner or parent/guardian played a major role (29.3% gave this reason). About 4.8% (only males) indicated that it was the business of their sexual partner to use contraceptives. Six per cent of the respondents were too embarrassed to use contraceptives, while 11.3% gave no reason. Sources of Contraceptives Table 6 shows the percentage distribution of current modern contraceptive users by most recent source of supply according to method (in the last 3 months). The respondents' sources include pharmacy shops (58.3%), hospital/clinics (18.3%), community distribution agents (10.9%), patent medicine stores (11.1%) and drug hawkers (3.0%). Apart from the methods requiring direct contact with the health workers pharmacy shop was the commonest source of modern contraceptives. KNOWLEDGE OF AIDS AND HIV PREVENTING MEASURES All respondents were highly knowledgeable about acquired immune deficiency syndrome (AIDS). They all identified sharing of blades for shaving, circumcision or minor surgery, sharing of injection needles, blood transfusion and indiscriminate sexual intercourse without condoms as modes of HIV transmission. Sixty five per cent believed that HIV could be transmitted through French kissing. With regards to risk reduction strategies, all the respondents identified condoms, sexual abstinence and not having sexual partners who use intravenous drugs as a means of reducing the risk of HIV transmission. However, the use of condom to prevent sexually transmitted diseases (STDs) was inconsistent. Only 26% of condom users did so solely to prevent HIV transmission while 58% used the condom to prevent STDs in general and 73% used it mainly for contraception. Majority (69%) were likely to consent to sexual intercourse without condom during safe periods and with their steady partners. DISCUSSION AND RECOMMENDATIONS This study shows a predominance of condom as a contraceptive method among Nigerian undergraduates. Their choices of contraception were not associated with age, marital status, religion or previous experience with induced abortions. The influence of gender on the choice of contraception was not explored in Table 3 because responses by the respondents were unreliable. Reports in literature have shown that self-reports of sexual activity and possibly contraceptive use by youths are often inconsistent especially among males.30 Similarly, some respondents sighted post-coital pills as current contraceptive method used. It is uncertain whether these few respondents had used the method for emergency protection against pregnancy in situations like sexual assault or failure to use regular contraceptives before sexual intercourse. It will be of importance to educate the students that post-coital pills should be used only in cases of emergency and not allowed to replace regular contraceptives. It is unusual to find out that the less effective contraceptive methods, e.g., rhythm and withdrawal methods were commoner with older respondents. Naturally, one would expect those just becoming sexually active to start with these methods before graduating to the more effective ones as they become more confident and experienced. The overall popularity of these less effective methods amongst current contraceptive users indicates a need for education on efficacy of each available method. This is more so as the commonest reason given for the respondents' choice of contraception was efficacy. In Nigeria, students are admitted into the universities and polytechnics after their senior secondary education and after passing the Joint Admissions and Matriculation Board examinations. Commonly, most students resolve to study in the polytechnic following failed attempts to secure university admission. Undergraduates of both types of institutions fall within the same age bracket. However, the presence of postgraduate students in the universities, who are sometimes older, more matured and experienced than their undergraduate counterparts should influence the behaviours of some of their undergraduate counterparts. These differences did not seem to influence the sexual behaviours and contraceptive choice of the respondents in this study when correction is made for age and marital status. Similarly, both institutions have students living off campus, away from home, and this mode of living is bound to influence their social attitudes. Although most of the respondents lived on campus, it is noteworthy that those living off campus away from home had fewer restrictions and were likely to be more sexually exposed than the on-campus students. Therefore, off campus students will require more contraceptive services than their counterparts living on campus. Fear of side effects and perceived safety of a contraceptive can strongly influence its choice or continuation.31-35 Anxiety about health hazards was a major impediment to contraceptive use in this study and could adversely affect the success of family planning programmes among youths who are ultimately concerned about future pregnancies when required. Thus, there is an urgent need for information on each method with regards to associated advantages and drawbacks. The fact that pharmacy shops and patent medicine stores constitute a major available source of contraceptives suggests that information should be made available in these stations by way of leaflets, advertisement and posters. The managers should be educated and encouraged to discuss freely and sincerely about contraception with youths. Information centres and family health clinics should be made available in higher institutions to encourage users and non-users alike to seek adequate knowledge on family planning and reproductive health issues. Attitude of youths towards sexual intercourse and prevention of HIV transmission is worrying because they are the most likely to spread the disease. It is certain that focus group discussions will provide better insight to this attitude than posted questionnaires. Our findings agree with previous African studies20,21,36 conducted over the last ten years. Unfortunately, it seems the message of AIDS prevention has not reached the youths. Although majority have adequate knowledge of HIV transmission and prevention, only few are taking positive preventive measures. One can confidently argue that once condom is used to prevent pregnancies it provides protection against HIV transmission and other STDs at the same time. However, it is essential that youths become AIDS conscious and take positive steps to prevent its spread in the community. Therefore, enlightenment is required in this regard and the use of condoms should be encouraged, as it is cheap and readily available. One major way of preventing clandestine abortions in Nigeria is the provision of family planning services.37 Despite availability of family planning services in Nigeria since the early sixties acceptance by youths is still very poor.26 This study shows that knowledge of contraceptive methods far outweighs use by undergraduates. Only 34.2% of the respondents were using contraceptives at the time of interview. This is a far cry from 87.2% of them that had good knowledge of contraception. The problem would seem to be with respondents' unwillingness to use contraceptives due to some misconception about contraception or the other. This indicates that a lot of misinformation exists. For example, long-term contraceptive use has been erroneously associated with future genital disorders and sterility in some quarters.26,34,38 In addition, some believe that the use of contraceptives leads to promiscuity. This is because proper information dissemination systems have not been put in place in the institutions. Various organisations and researchers have shown that information about sex and contraception are obtained from many sources including peer groups, parents and older siblings.26,29,31 Wrong information about health and safety of contraceptives is bound to prevent potential users from trying a method. Therefore, in order to effect a change of attitude, access to correct information dissemination is a necessary strategy. Although it is believed that parents, teachers and trained personnel could provide information on contraceptives, their attitude could prevent youths from seeking advice from them. The judgemental attitude of health workers to the demand for contraception by young ones in a Zimbabwean family planning clinic has been reported.39 In the study, some providers reportedly told off young contraceptive seekers. Communication between parents and children on family planning is difficult and may be embarrassing. Youths attending a family planning clinic may face a variety of problems, which include hostility, stigmatisation and rebuff from health workers and older attendants. Therefore, it is essential to establish public and health workers' enlightenment programmes so that the problems of unwanted pregnancies and clandestine abortions can be minimised and the youths given access to services concerning their reproductive and sexual health. The international population conference in Cairo in 1994 emphasised the need for youths to be involved in planning, implementing and evaluating development activities that have direct impact on their daily lives.40 This should be encouraged. Information given should include prevention of unwanted pregnancies and STDs, including HIV/AIDS and sex education. Access to these services should be private and confidential. The role of parents in family health education cannot be over-emphasised. As seen in this study, 9% of non-users based their action on parents' advice. Reports from African studies have suggested that parents should be involved in providing reproductive health education to youths.26,38 Information dissemination through women in the society is important as mothers are often the closest confidants of these youths, especially the females. The misconception by some parents that sexual education for youths encourages early sex should be corrected. A study conducted in the United States of America amongst teenagers showed that the risk of early sexual intercourse is increased when inadequate information on sex-related issues is given to them.41 The study indicates that sufficient information on sexuality, pregnancy and STDs empowers youths with the will to reject early sexual intercourse. Information, education and communication are important means of providing optimum reproductive health services to youths. The results of this study reveal an urgent need to provide special designated centres for youth health services in Nigerian higher institutions where reproductive health matters can be discussed and managed. ACKNOWLEDGEMENT This work would not have been possible without the cooperation and assistance of the respondents, their lecturers and those who helped to administer some of the questionnaires. We are grateful to them all. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02022t6.jpg] [rh02022t5.jpg] [rh02022t2.jpg] [rh02022t3.jpg] [rh02022t1.jpg] [rh02022t4.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}