 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 71-78 Where is the Condom? Contraceptive Practice in a Rural District of South Africa Jennifer Smit1,2, Lynn McFedyen1,3, Abigail Harrison1,4 and Khangelani Zuma5 1Africa Centre for Population
Studies and Reproductive Health, South Africa. 2Reproductive Health
Research Unit, Department of Obstetrics and Gynaecology, University of the
Witwatersrand, South Africa. 3Modelling and Simulation Group, Clinical
Sciences, Pfizer Global Research and Development, United Kingdom. 4HIV
Prevention and Vaccine Research, South African Medical Research Council.5 Biostatistics
Unit, South African Medical Research Council; and Statistics Department, University
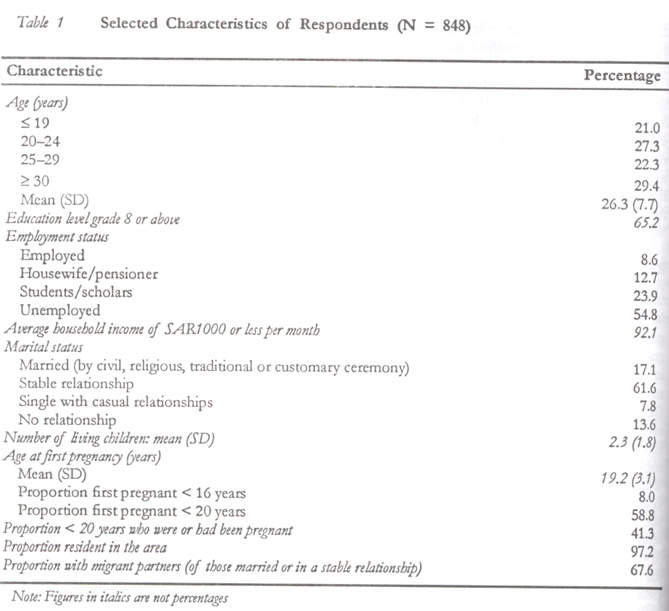
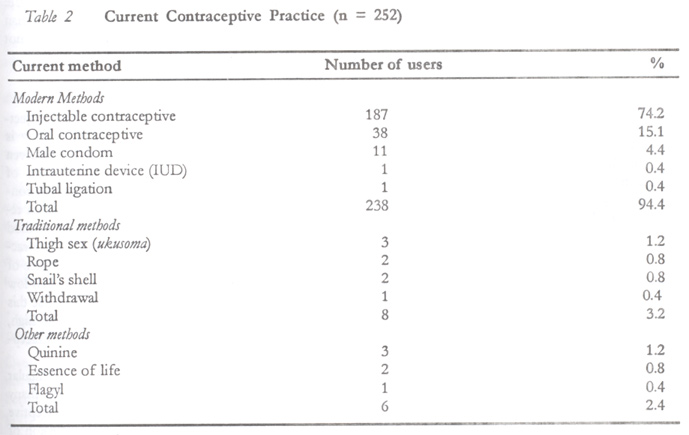
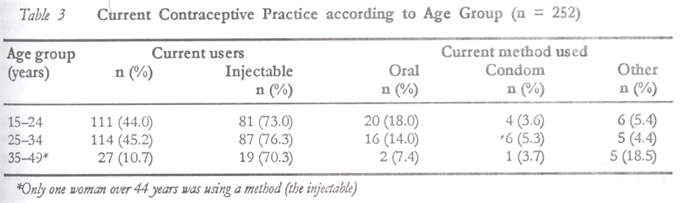
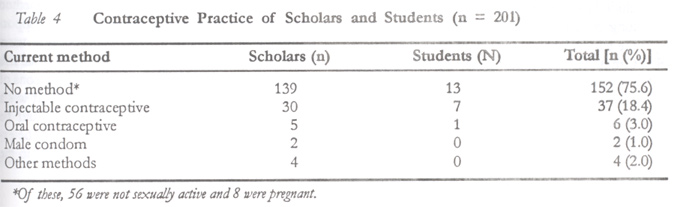
of Waikato, New Zealand. Code Number: rh02023 ABSTRACT Interviews were conducted with 848 African women aged 15–49 years in a rural area of South Africa to determine the extent to which condoms are used, reasons for contraceptive method choice and unmet contraceptive need. Injectable contraceptives were being used by 22.1% of respondents, who considered them to be convenient, safe, effective, and/or a method that could be used secretly. The decision to use this method was often made on the recommendation of a health worker. Eleven women said they were using the male condom, seven of whom were using it because it provides protection against pregnancy and sexually transmitted infections. Many (70.3%) women were not using any form of contraception. Counselling about contraceptive options should take into account the need for dual protection, and strategies for increasing condom use should be promoted. (Afr J Reprod Health 2002; 6[2]: 71–78) RÉSUMÉ Où est le préservatif? l'usage du contraceptif dans un district rural de l'Afrique du Sud. Nous avons eu des entretiens avec 848 femmes africaines âgées de 15–49 ans dans une région rurale de l'Afrique du Sud pour déterminer l'ampleur de l'usage des préservatifs, la raison pour le choix de la méthode contraceptive et le besoin de contraceptif qui n'a pas été satisfait. 22,1% des répondantes utilisaient des contraceptifs injectables qu'elles considéraient comme étant convenables, saufs, efficaces et/ou comme une méthode qu'on pouvait utiliser en cachette. C'était sur la recommendation d'une assistante sociale que la décision d'employer cette méthode a été souvent prise. Onze femmes ont déclaré qu'elles utilisaient le préservatif pour hommes; 7 d'entre elles l'utilisaient parce qu'il sert de protection contre la grossesse et les infections sexuellement transmissibles. Beaucoup de femmes (70,3%) n'utilisaient point de contraception. It faut que les conseils sur les options contraceptives tiennent compte de la nécessité pour la double protection; il faut également promouvoir les stratégies pour l'augmentation de l'usage du préservatif. (Rev Afr Santé Reprod 2002; 6[2]:71–78) KEY WORDS: Contraception, condoms, dual protection, South Africa INTRODUCTION Use of barrier methods of contraception in South Africa is reported to be very low. The 1998 South Africa Demographic and Health Survey (SADHS)1 found current male condom use to be 1.9% amongst all women interviewed in the age range 15 to 49 years, and 2.3% amongst women sexually active in the four weeks prior to being interviewed. Male condom use was reported to be only 0.6% amongst all non-urban women interviewed.1 The SADHS report did not include information about female condom use. A national introductory strategy of the female condom to some South African public sector health facilities commenced in 1998.2 However, the female condom is not yet available at all facilities. On the other hand, the progestagen-only injectable hormonal contraceptives are widely used by South African women.1,3-8 According to the SADHS,1 injectable contraceptives were currently used by 27.3% of all women aged 15–49 years and by 30.1% of women sexually active in the four weeks prior to being interviewed. The injectable contraceptive is particularly popular amongst younger users and women living in rural areas.1 While studies undertaken in South Africa have examined contraceptive prevalence, contraceptive method mix, and reasons for method switching or discontinuation,1-10 an extensive literature search revealed no published studies that describe reasons for method choice amongst South African users. With the exception of one qualitative study amongst 40 adolescents in the Northern Province of South Africa,11 published studies that explore reasons for non-use of contraception amongst potential South African users were not found. In this one study, the main barriers to contraceptive use among adolescents were the experience or fear of side effects and harassment by clinic nurses, who regard them to be too young to be sexually active.11 With one in four women attending antenatal clinics found to be infected with HIV in 2000,12 one would expect to see a move away from injectables as the main method of contraception to the use of condoms, which provides dual protection against sexually transmitted infections (STIs) including HIV and unwanted pregnancy. HIV prevalence as high as 37.4% was reported among 20–24-year-old pregnant women in a study undertaken in rural KwaZulu-Natal.13 Teenage pregnancy rates are also high, with 35.1% of teenage girls reported to have been pregnant by age 19,1 and the need for effective contraceptive methods remains. However, the low use of barrier contraceptive methods is disquieting and the development of an understanding of what guides decisions about contraceptive use is urgently required. Against this background, this paper describes contraceptive use patterns and the extent to which condoms are used in a rural area of KwaZulu-Natal in South Africa. Reasons for contraceptive method choice and unmet contraceptive needs are analysed. Based on this analysis, and taking into account the need for dual protection against unwanted pregnancy and HIV infection, appropriate contraceptive options are proposed and strategies for increasing condom use identified. METHODS Setting and Sample Contraceptive patterns of use were determined by means of a community-based cross-sectional survey undertaken in a rural sub-district comprising 13 wards (isigodi) in northern KwaZulu-Natal, South Africa. Commencing from a randomly selected starting point, every second household in each isigodi was chosen until 40% of the estimated 2088 households in each isigodi had been visited. Verbal and written explanations of the study were given to each woman selected, and 848 women aged 15–49 years were interviewed. Prior to commencing the survey, workshops and meetings were held to introduce the study to local traditional leaders, community health workers and health service providers. Approval to conduct the study was granted by the Ethics Committee of the University of Durban-Westville. Data Collection and Analysis Data were collected by means of an extensive structured interview, which included questions on demographic characteristics, reasons for selection of contraceptive methods, problems and side effects experienced with current and previous contraceptive methods, and reasons for not using contraception. Since the focus of the study was on contraceptive use and method choice, questions about HIV/AIDS were not included. The study did not explicitly explore concurrent use of more than one method (dual method use) or consistency of condom use. Interviews were conducted in Zulu between September and December 1998. They were conducted during the day from Monday to Friday, but where a selected woman was not at home a repeat visit was made in the evening or on Saturday. Data were coded, double entered and analysed using Epi-Info Version 6.43 (Centre for Disease Control, Atlanta) and the Statistical Analysis System (SAS) Version 6.12. RESULTS Description of the Study Population In total, 848 African women, whose home language was Zulu, were interviewed. Selected demographic characteristics of respondents are shown in Table 1. Their mean age was 26.3 years (SD 7.7) and almost two thirds had an education level of Grade 8 or above. Only 8.6% were employed (formally or informally) and 23.9% were students or scholars. Most of the women (61.6%) were in a stable relationship, but few were married (17.1%). Whilst nearly all respondents (97.2%) were resident in the area, many of their partners (67.6%) were not, and 74.1% of these migrant partners did not return home for a month or longer. In a few cases (n = 14) partners returned only once a year, usually for the Christmas holidays. Many respondents (58.8%) were first pregnant in their teens and 41.3% of those under 20 years at the time of the survey were or had been pregnant at least once. Current Contraceptive Practice Less than one third (29.7%) of all women (N = 848) reported use of a contraceptive method at the time of the survey. Only 1.3% of respondents reported the male condom as their current method and none was using the female condom. As expected, the most commonly used methods were the long-acting progestagen-only injectable contraceptives, depot medroxyprogesterone acetate and norethisterone oenanthate, used by 22.1% of all the women. Current use of natural family planning methods such as the calendar or rhythm method or the basal body temperature method was not reported. Of those using a method (n = 252), 94.4% were using a modern method (injectable or oral hormonal contraceptive, male condom, intrauterine contraceptive device, tubal ligation), 3.2% a traditional method and 2.4% other methods not registered with the Medicines Control Council for contraceptive use (Table 2). In contrast to the widespread use of the injectable method (74.2% of women practising contraception), the condom was used by only 4.4% of current users. In the age range 15–24 years, 73.0% of those using a method (n = 111) were using the injectable, whilst only four women (3.6%) were using the condom (Table 3). Amongst students and scholars, 18.4% were using the injectable and only 1.0% used the condom (Table 4). Reasons for Method Choice In response to an open-ended question about reasons for choosing the injectable method, the most common reason given by 35.0% of respondents was that it was convenient. The method was considered to be convenient since it only has to be used every two or three months, or because one does not have to remember to take it everyday as with the oral contraceptive. Nearly one quarter of the injectable users (23.0%) chose this method because it is effective, often making statements such as “its always in my blood” or “it stays in the blood a long time”. The third most common reason given for using the injectable is that it was recommended by the clinic health personnel (19.7%). Some respondents (4.9%) simply stated that the method “suited them”, and others expressed a dislike for oral contraceptives because of side effects experienced (4.4%). A few respondents chose the method because it could be used without their partner's knowledge (2.7%). Similar responses were given when injectable users were prompted to respond to each of a list of 10 possible reasons for choosing the injectable method. Almost all (96.3%) the 187 injectable users indicated that they chose this method for convenience, as they only had to return to the clinic every two or three months. Others said it was effective (47.6%), it was recommended at the clinic (37.4%), few problems or side effects were experienced (27.3%), it caused amenorrhoea (23.0%), it was recommended by friends or relatives (21.5%), and it was a method that could be hidden from partners (20.9%). Although not reported in response to the open-ended question, 52.9% agreed that they chose the injectable method because they felt that it was a safe way to prevent pregnancy. A quarter (25.8%) of the women were using a method other than the injectable, and the most common reason for method choice given by 43.3% in response to an open-ended question was related to injectable side effects. Although almost half of the women giving this response had used the injectable method before, only 55.6% of these previous injectable users gave this as their reason for current method choice. A few were using a method on the recommendation of their partner (n = 4), relatives or friends (n = 1), or the health provider (n = 2). Six of the women giving this response were using the oral contraceptive and one was using the withdrawal method. Of note is that seven women were using the condom and three were using thigh sex, because these methods were considered to provide protection against both pregnancy and sexually transmitted diseases. The remaining condom users indicated that they did not like the side effects of oral contraceptives or that their partner was often away and a regular method was not needed. Reasons for not Using a Method Of the 848 women interviewed 70.3% were not using a contraceptive method. Reasons for not using a method are broadly grouped as follows:b
In all, less than two thirds (61.2%) of those not using a method were not sexually active, were pregnant or wanting to get pregnant, or had had a hysterectomy. This suggests an unmet need for more appropriate contraceptive methods or services than those available amongst nearly 40% of women not practising contraception. DISCUSSION The pattern of low condom use and high injectable contraceptive use reported in this study is consistent with findings from the SADHS.1 Given the high prevalence of HIV in rural areas of KwaZulu-Natal, the low use of condoms for contraception requires attention. Only 11 women reported the male condom as their current method and none was using the female condom. The practice of thigh sex, which may offer some degree of protection against HIV and pregnancy, is also low with only three women reporting that they use this method. Since teenage pregnancy rate is also high, the need for effective but appropriate contraceptive methods is clearly evident. Understanding why women choose a particular contraceptive method and recognising that many women do not need or wish to use a contraceptive method and why, are essential to the provision of effective advice about HIV preventive measures. Findings from this study assist in the development of pragmatic guidelines for counselling women about appropriate contraceptive options. Understanding Method Choice Health workers play an important role in women's decisions to use injectable contraceptives. In this study, many injectable users indicated that they chose the method because it was recommended at the clinic. Only two women using other contraceptive methods gave this as a reason for method choice. This suggests that there are missed opportunities for counselling potential condom users about barrier method use to minimise the dual risk of pregnancy and HIV infection. Other reasons of note for choice of the injectable were that it was a convenient and effective method that could be used secretly. The low use of condoms may be explained by their failure to meet these criteria to the extent that the injectable does. The need by some for secrecy particularly precludes the use of the condom, which requires the cooperation of the partner. Where contraceptive efficacy is the criterion for method choice, women at risk of HIV infection should be counselled to use condoms in addition to their hormonal method. An important observation from this study is that at least 10 respondents had embraced the concept of dual protection – the simultaneous prevention of pregnancy and STIs – indicating that they were using the male condom or thigh sex because it provided protection against pregnancy and STIs.c This finding is encouraging as it may indicate that educational messages aimed at dual protection against unwanted pregnancy and HIV/STIs are reaching even remote rural areas of the country, or that women are recognising the need for dual protection. Understanding why Women are not Currently Practising Contraception Over two thirds of the women interviewed were not using a contraceptive method. Many had never been sexually active or were sexually inactive at the time, and these women were not at risk of unwanted pregnancy or infection. However, nearly 40% of non-users were estimated to be at risk of an unplanned pregnancy and even more, including those who were pregnant or wanting to conceive, were at risk of contracting HIV. Many of the women had migrant partners who were absent for long periods of time and a reason put forward for not practising contraception was infrequent sexual intercourse. These women's contraceptive needs are intermittent and often unpredictable. Provided that the partner is willing the condom (male or female) would be an appropriate contraceptive option for them, particularly as a dual protection method, since several studies have shown that migrants are at greater risk of being infected with HIV and other STIs.14 The much promoted message “use condoms to prevent HIV” is clearly inappropriate and unhelpful for women trying to conceive. These women, who are at risk of being infected, should be counselled about risk reduction strategies such as having unprotected sexual intercourse only at the fertile period of the cycle. The “use a condom” message, which generally refers to male condoms, is also inappropriate for women whose partners refuse to use male condoms. For these women who want to prevent pregnancy the injectable remains a rational choice. The female condom was not widely available in South Africa at the time of this survey, however, the national female condom introductory strategy launched just prior to the survey is being expanded to more public sector health facilities.15 This will make this female controlled method more widely available. However, it should be noted that two female condom acceptability studies undertaken in South Africa have reported a mixed reaction to the acceptability of the female condom.2,16 Behavioural interventions designed to develop negotiation and decision-making skills for women and to promote gender equality and respect by men for women's reproductive rights are urgently needed. The promotion of mutual monogamy and other low risk sexual behaviours is also important. Where women attempt to negotiate condom use and fail, awareness of emergency contraception to prevent pregnancy is important. Women who do not need contraceptive protection; for example, those who are pregnant, should be encouraged to use protective measures against HIV infection should they be at risk. Breastfeeding women may derive a level of protection against pregnancy, but this is not an effective contraceptive method and it does not provide protection against HIV/STIs. If the mother is HIV positive breastfeeding also carries the increased risk of transmission of HIV to the child. Individualised counselling on the appropriateness of breastfeeding is thus extremely important. RECOMMENDATIONS Dual protection against unwanted pregnancy and HIV/STIs is an appropriate strategy for many women in the context of South Africa's HIV epidemic, and should be integrated into counselling about contraceptive options. Strategies to increase use of male and female condoms should be promoted. First, for women wishing to delay or prevent pregnancy, counselling and decision-making about appropriate contraceptive methods should take into account the dual risk of pregnancy and infection with HIV/STIs. Second, appropriate counselling about reducing the risk of HIV/STIs for women wanting to conceive or those not wishing or needing to practise contraception is also required. Third, health workers clearly play an important role in decision-making about contraception and may be happier to promote condom use over the injectable method if they are reassured about efficacy. Promoting the use of emergency contraceptive pills as a back-up for condom use may result in increased likelihood of condom promotion. Fourth, more attention should be paid to promoting female condom, which provides dual protection and is under the control of women. Microbicides, which protect against HIV/STIs and pregnancy are being developed and may in the future be an important option for women. The search for microbicides that are not spermicidal is also underway. These research efforts should be vigorously supported. Finally, effective sexuality education programmes are urgently required especially for young women who are particularly vulnerable to unplanned pregnancies and HIV/STIs. ACKNOWLEDGEMENTS This research was supported by a grant from the Wellcome Trust (Grant Number 050543/Z/97/C). We are grateful for the assistance of our fieldworkers and data capturers and to the women who willingly participated in the study. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02023t3.jpg] [rh02023t1.jpg] [rh02023t4.jpg] [rh02023t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}