 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 2, August, 2002 pp. 79-86 Indigenous Healing Practices and Self-Medication amongst Pregnant Women in Cape Town, South Africa Naeemah Abrahams, Rachel Jewkes and Zodumo Mvo Gender & Health Research Group,
South African Medical Research Council, P.O. Box 19070, Tygerberg 7505 Cape
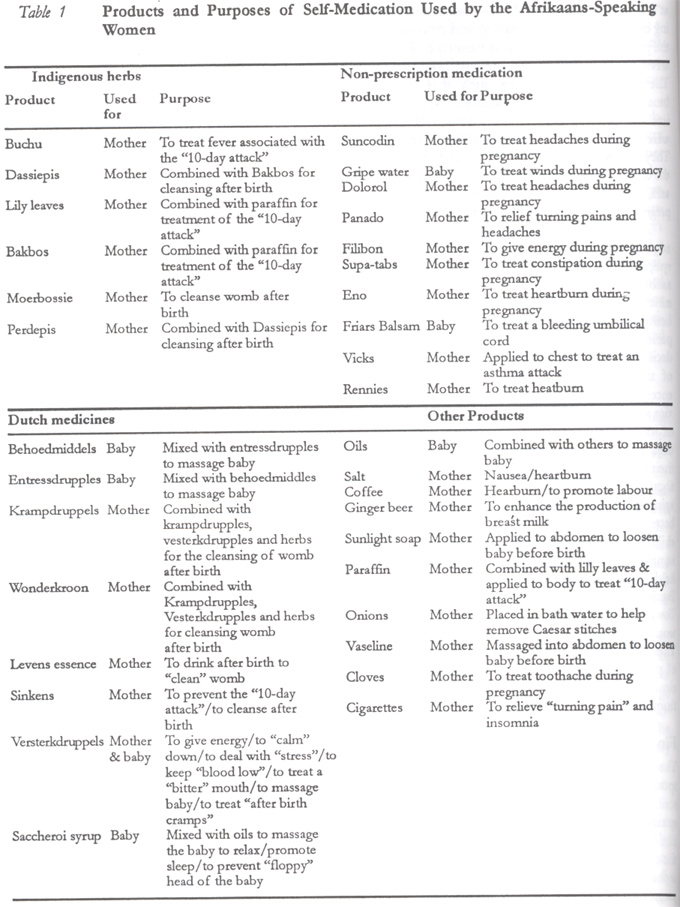
Town, South Africa. Code Number: rh02024 ABSTRACT This study was conducted in and around Cape Town, South Africa, at two primary obstetric facilities and in the antenatal clinics of two secondary hospitals. Findings show that majority of the Xhosa speaking women follow indigenous healing practices for both themselves and their babies because of the need to “strengthen” the womb against sorcery, to prevent childhood illnesses, and to treat symptoms they perceive that biomedical services would not be able to treat. Self-medication with non-prescribed drugs, herbs and Dutch remedies was common practice amongst the Afrikaans speaking women for both themselves and their babies. Herbs and Dutch remedies were mainly used to treat indigenous illness (baarwind) while non-prescribed over-the-counter drugs were used to treat minor ailments associated with pregnancy. There is, therefore, an urgent need to bridge the gap between orthodox and indigenous medical systems through reciprocal learning and by acknowledging each other's roles. (Afr J Reprod Health 2002; 6[2]:79–86) RÉSUMÉ Pratiques de la guérison indigène et l'auto-médication chez les femmes encintes à Cape Town, Afrique du Sud. Cette étude a été menée à Cape Town et les environs auprès de deux établissements obstétriques dans des cliniques de consultation prénatale situées dans deux hôpitaux secondaires. Les résultats ont montré que la majorité des femmes d'origine Xhosa pratiquent la guérison indigène pour elles-mêmes et pour leurs bébés à cause de la nécessité de “renforcer” la matrice contre la sorcellerie, pour prévenir les maladies de l'enfant et pour soigner les symptomes qu'elles aperçoivent et que les services biomédicaux ne peuvent pas guérir. L'auto-médication avec les médicaments non-ordonnés, les remèdes à base des plantes a été largement pratiquée pour soigner les maladies indigènes (baarwind) alors que les médicaments qui n'ont pas été utilisés pour soigner les maux associés à la grossesse. Il y a donc la nécessité urgente de combler le fossé entre les systèmes médicaux traditionnels et indigènes à travers un apprentissage réciproque et à travers une reconnaissance de leurs rôles réciproques. (Rev Afr Santé Reprod 2002; 6[2]:79–86) KEY WORDS: Indigenous healing practices, self-medication, pregnant women, South Africa, Dutch remedies INTRODUCTION Indigenous healing practices are increasingly of scientific interest. Much of the interest to date in medical writing has been the potential for harm caused by traditional practices.1-3 In keeping with calls for an African renaissance, however, there is need for a shift in emphasis towards developing an understanding and recognition for the value of indigenous knowledge. Anthropologists recognise that health-seeking practices of patients in a society like South Africa fall within three overlapping sectors — the biomedical sector (modern Western medicine), the folk sector (traditional healers and faith healers) and the popular sector (self-medication and lay treatment).4 Although practitioners of the formalised folk sector are often regarded as the main repositories of indigenous knowledge, lay `practitioners' of the popular sector also deserve attention. It is here that ill-health is first recognised, health care activities initiated and sets of beliefs about health maintenance are held and acted upon.5 In this paper we explore self-medication and indigenous healing practices as described by pregnant women in Cape Town, South Africa. Data was collected during a study of health seeking practices in pregnancy that was undertaken amongst women attending public health services in Cape Town. Other findings from the study are published elsewhere.6-7 This is the first paper describing practices of Xhosa and Afrikaans speaking women in South Africa; previous published work on indigenous medicine use in pregnancy has exclusively focused on use amongst Zulus living in the Kwazulu-Natal area.1-3, 8-11 STUDY SETTING Since 1994, as part of the transformation aimed at decreasing inequities, the South African National Health System adopted the primary health care approach to improve access of health services to disadvantaged communities. Part of this transition was free antenatal and delivery services for all women who do not have medical insurance. The majority of deliveries in South Africa thus occur in the public health sector in clinics or state hospitals. This study setting was based in the primary care system for obstetric services in Cape Town, Western Cape Province. The system is organised into three tiers with the primary tier comprising of midwife obstetric units (MOUs), which are managed exclusively by midwives; the second tier is a secondary level hospital and is usually the first point of referral/transfer for women who have a history of or develop pregnancy complications, and the third tier is the tertiary hospital. The Cape Town area has a large Afrikaans speaking population, which is made up of mix ancestry (categorised as “coloured” during the apartheid period). During the apartheid era the African population (mainly Xhosa speaking) was prevented from settling and working in this province. They currently only make up one fifth of the province's population. These racial divisions have created a complex set of racially separate residential areas. Health service location and delivery are patterned after these residential areas. There are three major languages in the region: the Blacks speak predominantly Xhosa and English, while the “coloured” and white people speak mostly English and/or Afrikaans. METHODS The research used qualitative methods including individual minimally structured in-depth interviews, group discussions and participant observation. In-depth interviews were conducted with thirty two pregnant women and seven indigenous healers. Group discussions were held with Xhosa speaking women who had recently given birth. The women were recruited at two primary obstetric facilities (each based in a predominantly Afrikaans and Xhosa speaking residential area) and in the antenatal clinics of two secondary hospitals. These were in and around Cape Town. The pregnant women were interviewed repeatedly during their pregnancy by two interviewers, giving a total of 103 interviews. Interviews were conducted in the woman's preferred language (Xhosa, Afrikaans or English) and were audio-taped, translated and transcribed into English. The 17 Xhosa-speaking women attended one primary level facility, while the Afrikaans-speaking women were recruited at a primary (10) and a rural secondary (5) facility. With the exception of two women who delivered unbooked, pregnant women were recruited by researchers at the clinic during their first antenatal visit and most first interviews were done immediately at the clinic. Follow-up interviews took place at the women's homes (the number varied depending on the stage of pregnancy) and continued until the postpartum period. Most women had three interviews of between one and two hours duration. The women were chosen such that they were broadly representative of women using the services. Their ages ranged from 17 to 40 years, all were Afrikaans or Xhosa-speaking, parity (0–7). They included a range of socio-economic status, the duration of time woman had lived in an urban area, complications (or otherwise) and stage in pregnancy at which they booked. The interviews covered the women's knowledge of their bodies, pregnancy and childbirth; symptoms experienced; interpretation of the causation; severity and risks of illness during pregnancy; who is involved in the decision to seek health care; and self-medication and use of non-prescription products. Other issues covered were decisions regarding the timing and pattern of use of antenatal services and place of birth; experiences of the health services particularly health advice and interventions received and their evaluation of its appropriateness and traditional health practices. At each interview women were asked about their health since the last interview and were asked about any treatment taken or help sought in managing their health complaints. In order to gain a better understanding of ideas about pregnancy and childbirth in indigenous healing practices, seven minimally structured in-depth interviews were also held with indigenous healers recruited through the Buzani Kubawo Inyanga's Association in the Cape Town area (4 Xhosa and 1 Zulu; 2 men and 3 women) and in the former Transkei (2 women). These interviews focused on healers' perceptions of pregnancy, the types of problems women experience in pregnancy and for which they seek help from healers, their causes and treatments. FINDINGS The Xhosa and Afrikaans speaking women responded in different ways to symptoms and described different preventive practices. The Xhosa-speaking women mostly went to the antenatal clinic with their health complaints, two attended the community health centre with flu, and only one reported having consulted a private doctor during pregnancy. They described self-medication, mostly with indigenous preparations. The only products that were said to have been bought from a chemist were grandpa powders and panados for pain, and several mentioned having been told by hospital staff to be careful about medication use in pregnancy. In contrast, the Afrikaans speaking women were much more likely to have sought care from the private sector or took medication for symptoms. They responded in different ways to illness depending on their perceptions of the severity and nature of the problem but often spoke of attending the after hours clinic, a pharmacy, a private doctor or followed self-healing practices, which included taking non-prescription medications, indigenous herbs, Cape Dutch remedies and a variety of other non-medicinal products (see Table 1). Receiving medication was an important criterion by which the satisfactoriness of care was judged, even though they too were aware that they should be cautious about taking medication during pregnancy. Not being given medication was perceived to be tantamount to not being given care, and this influenced women's choice of health care provider. Use of Xhosa Medicines and Practices Roughly two-thirds of the Xhosa-speaking women followed indigenous healing practices for themselves, their babies, or reported having done so in previous pregnancies. Others said they knew little about “traditional matters” or did not use traditional medicines because they were church goers (and would pray instead for protection against sorcery). These traditional practices, however, were not used exclusively and many women reported combining traditional healing practices with others such as faith healing. Some women suggested that they felt more protected from sorcery in a township compared to rural areas. Nonetheless, many had been advised about indigenous practices by friends and relatives. The main concerns for which women looked to indigenous practices related to the need for “strengthening” the womb against sorcery, the prevention of the childhood illness, umoya omdaka (dirty wind), and treatment of symptoms that had not been helped by the biomedical services. The indigenous healers interviewed suggested that women might consult at any stage of pregnancy, but one said this is commonly after the sixth month. The indigenous healers explained, and many of the women agreed, that the period of pregnancy is a “delicate” time when women have “lots of problems”, some of which are particularly unpredictable and could lead to the death of the mother or child. Women and their babies were said to be vulnerable to “evil” sent by another person (directed sorcery), particularly a neighbour or a girlfriend of the child's father, who has a “grudge” or is “jealous”, or just to `spells' which a woman might step over in the environment (non-directed sorcery).2 The women described using medicines during and after pregnancy for “strengthening”. Some liquid medicines were taken orally, such as “baboon's urine” (uchamo wemfene) and isicakathi; others were put on a fire “to make smoke where you live” and another form was called intambo. This was described as a material which the healer twists and smears with medicines and gives to a woman to wear around her waist until the baby is born. One respondent said her father made one from part of a cow's tail. The intambo would protect a woman against “jumping over dirty things” (umeqo). One of the healers said he protected mothers “from the outside” by making two small incisions and putting powder into the wound and by giving her something to use when she baths and to sprinkle in the house. Most women bought their medicines from indigenous healers (Afrikaans and Xhosa speaking), or obtained them from concerned relatives. One explained how she would prepare isicakathi herself in the rural area from roots called inkunzane, which she would cook and give to the baby, but she was embarrassed to “take her spade and dig for herbs” in town. Another asserted that “most pregnant women start taking those medicines at four months until delivery” to ensure an easy and safe delivery. Women described practices to protect their babies against umoya omdaka after birth much more often than taking something themselves. The healers explained that umoya omdaka is a childhood illness that can affect children of any age, although it can cause problems for pregnant women as well. Its symptoms include green diarrhoea, restlessness, crying, stopping sucking, fits, grey tongue, constipation and a sunken fontanel. They indicated that all children are vulnerable to it but most said it is not every child that develops it. Umoya was said to have several causes; it may be transmitted to a child in the womb by a mother who has `stepped over' something that has made her womb dirty; it may be spread by impundulu (the lightening bird) through witchcraft; it could be determined by ancestors and indicated by the child being born covered with the membranes or a cord around the neck. Two healers indicated that it could be infectious, transmitted either through impundulu or just by being in a house with a child who has umoya. Since the period of vulnerability for the baby is long, treatment is often said to be continued for two years. Commonly the arrangement is a one-off payment (R50 in the case of the Apostolic), which would entitle the baby to a full course of this. Treatment was described as involving medicines to drink, the use of herbs injected anally (`spading'), creams or ointments that could be rubbed on the body or herbs in a tiny wallet on a string. One woman said she had been given a bottle of Xhosa medicine for herself and the baby, out of which she was to take a teaspoon everyday, a rubbing medicine mixed with vaseline and a wallet for the baby. Whilst another explained that she had been advised in the hospital to go to the Apostolic for umoya protection or to get a wallet rather than give the baby medicines, because “some people do not know how to prepare the correct mixtures and the baby dies”. She said that “as soon as she could” she took him to be rubbed twice a week and got him a wallet. Other things that women reported giving include gripe water and umthombothi (indigenous medicine given to babies). As well as for strengthening, some women reported consulting indigenous healers with symptoms. The women informants said they did so after being dissatisfied with the clinic, but one of the healers said women sometimes come to them first and they might refer them to be checked by a “doctor”. One said she was given medicines because she was having stomach pains and hardness. The clinic had given her an ultrasound (“X-ray”) and iron tablets, but she didn't perceive the pills worked and so returned to report this, only to be told that the baby was “stretching”. Then she went to a healer who gave her medicine, which helped her. Another woman was given medicines for umoya during her eighth month of pregnancy because of waist pains, which the doctor could not cure. She complained that it was expensive but spoke admiringly of the healer when she described the process, saying if you go and say you want medicines for pregnancy and how far you are “he will automatically know which medicine to prepare for you”. The healers indicated that in the last month of pregnancy they would give women medicines (imbelekisone) to ease labour. Some of the healers (male and female) said they used to assist mothers in birth when they lived in rural areas but did not do so in the urban areas because they were not allowed. They described, however, circumstances in which some women gave birth on their premises and strongly implied that healers did occasionally assist in delivery. The healers and one of the women said healers had, and used, medicines which would make women who had had a caesarean section deliver normally next time. One woman said she “would like to use them” but didn't think she should trust them when she was near “doctors and hospitals”. Several of the women indicated considerable overlap between concerns of indigenous health care and biomedicinal service use, notably in a perceived need to know how the baby was “sitting”, in perceptions of the benefit of massage and palpation, in (unmet) desires for something for “protection” from the clinic, and general perceptions that this was a vulnerable time. The woman who delivered at home also suggested that she had not told the tertiary hospital staff that she thought she was in labour as they should “see” this, which is also resonant of the practices of patients when they consult indigenous healers, as they also do not express their concerns verbally. Self-Medication by Afrikaans Speaking Women Given the emphasis that Afrikaans speaking women placed on receiving medication from health services, it is not surprising that self-medication is a common practice of both rural and urban women. They described a variety of ways in which they treated their minor ailments during and after pregnancy as well as prophylactic treatment for health maintenance for their new born babies. The indigenous herbs used by these women are described in Table 1 and were locally available herbs known for the treatment of common reproductive health problems. Herbs and Dutch remedies were predominantly used to treat indigenous illnesses particularly associated with womb `dirtiness' or “baarwind” (winds in the womb), which was perceived to be the cause of the “10-day attack”, a wind from the womb which goes to the head. Womb dirtiness was perceived to be a problem after birth, for which cleansing with herbs is required, “to allow all the old blood and things to come down”, and thus these were used exclusively after birth. Mothers, grannies, aunts and elderly women in the community were mentioned as the most common sources of information about herb use and are frequently consulted. Often the herbs are prepared by the older woman after they have been bought or picked from the garden. One woman described how her granny was “angry” when she discovered that she had been bleeding continuously for nine months after the birth of her previous baby. The granny had treated her with “home remedies”, which “worked immediately” and caused the passing of “massive pieces of blood”. Women were only instructed on their use when they were pregnant for the first time. Several of the women said they were warned by the older women not to prepare the mixtures too early since “leaving it to stand” (Dutch remedies combined with the herbs) can change the contents to a substance that could be used by others in witchcraft against them. The Cape Dutch remedies have a long history of use in the Cape and their popularity stems from their low cost and reputed efficacy for the treatment of minor health problems. Both urban and rural women had similar knowledge and used the Dutch remedies during pregnancies as well as after birth as oral preparations and massaging oils for the babies. The women said they use it to improve their “energy” levels, to treat high blood pressure, relieve tension, stress or induce calm during pregnancy. They said they used them for babies to “help them to sleep”, “to relax” and to “loosen the winds”, and to ensure tone in the neck muscles to prevent a “floppy” neck. The babies had to be massaged using a particular technique and the women were instructed on how to do this by older women such as mothers, grannies and aunts. One woman reported that the “old people believe that the smell will keep the devil away” and that this is the main reason babies are rubbed with the Cape Dutch remedies. The women most often use over-the-counter medication for the treatment of minor ailments. Food substances are also used. For example, some women reported “eating salt” or putting “dry coffee” on the tongue to treat nausea due to reflux, and one woman said they use these because they do not receive “heartburn tablets” from the clinics. More than one woman reported smoking cigarettes to relief symptoms, using “continuous smoking” as a way to help the “turning pain to subside”. The interviews suggest that women, particularly from the farms, perceived that “loosening” the baby is a necessary stage in childbirth, and some reported receiving advice to rub sunlight soap and vaseline onto their stomach to prepare the child for birth. During the narratives of delivery, it was apparent that some were told by nursing staff to walk around when in labour for the same reason. DISCUSSION The interviews indicated considerable overlap between many of the reported Xhosa indigenous healing practices and ideas of biomedicine. Generally, pregnancy in both systems is regarded as a time of vulnerability and unpredictability and both recognise the need for preventative measures to be taken by asymptomatic women. The findings suggest that use of indigenous medications for `protection' of pregnancy and treatment of infants is common. Indigenous healer services and self-medication in most cases were used in a manner that is complementary to, but not a substitute for, use of biomedical services, although several women indicated that in rural areas where access is poor they would be used instead. The only possible exception was the young unbooked woman who took medicine for protection whilst not attending antenatal care. However, it was not clear in the interview whether she consciously regarded it as a substitute. Some of the women consulted with traditional healers when they had symptoms that the clinic could not offer relief for. The women and healers indicated that ingested substances, when taken in small quantities, form only a part of the repertoire of treatments and there was some evidence of success of clinic strategies to encourage women to use non-ingested treatments at least for their babies. None of the Afrikaans speaking women indicated that she perceived the midwife-run primary obstetric care unit or hospital to be her first point of call when experiencing ailments in pregnancy, with the exception of symptoms of vaginal bleeding. This partly stemmed from the experience that most midwives do not show interest in treating women's minor ailments, but also because women are unimpressed by the reluctance of obstetric service providers to dispense medications. These self-medication practices thus provide relief and fill needs that the mainstream medical practice is not able to fill. Other reported factors influencing antenatal attendance in this study have been documented elsewhere and include women's knowledge of the role of antenatal care, booking systems, nurse-patient relationships and economic.6-7 The accounts of self-medication by the women indicate that a considerable range of products are taken during pregnancy and after childbirth. The pluralistic manner in which the Dutch medicine is used in combination with the herbs is explained by De Wet as an `indigenisation process” in her study that explored the use of “doepa”, a Dutch medicine used by mothers in Soweto for their infants.13 Many of the women said pregnant women should be careful about medication use, and it is notable that versterkdruppels is the only Dutch remedy used during pregnancy. This, however, is largely because their use, like that of herbs, is for treating indigenous problems particularly the '10-day attack' and womb dirtiness, which affect women after birth. The study has demonstrated important aspects of antenatal care that must be considered by those who care for pregnant women. It has provided some examples of ways in which health care provision to pregnant women is shared between Western medicine, indigenous healers and the women themselves. Most times the role of traditional health practices is ignored by Western medical practitioners unless the outcome is negative. Similarly, self-medication is also not acknowledged other than to warn women of negative outcomes. Yet in ignoring these forms of health care, medical practitioners restrict their knowledge of the spectrum of treatments used by their patients. Moreover, they lose the opportunity to understand some of their patients' health fears and perceptions of circumstances of risk. In so doing they miss both opportunities for reassurance and engagement with these risks as an approach to more effectively communicating messages relating to the use of biomedical services. In order to ensure that the health system is sensitive to women's needs we must bridge the gap between Western and indigenous/lay medical systems through reciprocal learning and acknowledging each other's roles and importance. ACKNOWLEDGEMENTS This research was funded by the Health Systems Trust. We would like to thank all the respondents who contributed so much of their valuable time to make this research possible. We also thank Nosisi Dingani for assisting in locating women's homes and transcribing tapes, and Wynda Van Eyssen for typing the reports. We would like to thank the tertiary hospital for giving permission to conduct the study. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02024t1.jpg] |
| |||||||||

{kind=link}