 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 38-43 Caesarean Myomectomy E Yao Kwawukume Correspondence: Dr E.Y. Kwawukume, Department of Obstetrics and Gynaecology, Korle Bu Teaching Hospital, Accra, Ghana. Code Number: rh02033 ABSTRACT This study was conducted at Korle Bu Teaching Hospital and Family Health Hospital, Accra, Ghana, between April 2000 and January 2001 to compare the efficacy and safety of myomectomy done at caesarean section with the application of a tourniquet with caesarean section without myomectomy. Twenty four patients were recruited into the study. Average haemoglobin of patients both pre and post-operatively was 11.73g/dl and 9.90g/dl for patients who had caesarean section with myomectomy and 12.07g/dl and 10.34g/dl in the other group in which caesarean section without myomectomy was performed. The average duration of operation was longer in patients who had caesarean section and myomectomy (62.08 mins) than those who had caesarean section alone (50.83 mins). The drop in average haemoglobin for patients who had caesarean section and myomectomy was 1.83 while those who had caesarean section alone was 1.73. This was not significant. The fibroid nodules removed ranged from one solitary nodule to six nodules with an average diameter of 6cm. Eighty five per cent of the fibroids were intramural and in the body of the uterus. Uterine involution was normal and there were no significant complications during the puerperium. We conclude that there is no significant difference in intra-operative and post-operative morbidity and blood loss in performing caesarean section alone and caesarean section with myomectomy when a tourniquet is applied. (Afr J Reprod Heath 2002; 6[3]: 38–43) RÉSUMÉ La myomectomie césarienne. Cette étude a été menée au Centre Hospitalier Universitaire de Korle Bu et à Family Health Hospital à Accra au Ghana entre les mois d'avril 2000 et janvier 2001. Elle avait comme but de comparer l'efficacité et la sécurité de la myomectomie faite pendant la césarienne à l'aide d'un tourniquet avec une césarienne sans la myomectomie. Vingt-quatre patients ont été recrutées pour effectuer l'étude. L'hémoglobine moyenne des patients, que cela soit pré ou post-opératoire, était 11,73 g/dl et 9,90g/dl pour les patients qui ont eu une césarienne avec la myomectomie et 12,07g/dl et 10,34g/dl dans l'autre groupe qui a eu la césarienne sans la myomectomie. La durée moyenne de la césarienne était plus longue chez les patients qui ont eu la césarienne avec la myomectomie (62,08mins) que chez les patients qui n'ont eu que la césarienne (50,08 mins). La baisse moyenne de l'hémoglobine chez les patients qui ont eu la césarienne avec la myomectomie était 1,83 alors que chez celles qui n'ont eu que la césarienne, la baisse moyenne était 1,75. Ceci n'était pas significatif. Les nodules fibreuses enlevées variaient d'une nodule solitaire à six nodules avec un diamètre moyen de 6cm. 85% des fibromes étaient intra murals et étaient au centre de l'utérin. L'involution utérine était normale et il n'y avait pas de complications importantes pendant le puerpérium. Nous affirmons, en conclusion, qu'il n'y a pas de différence significative dans la morbidité intra-opérative et post opérative; il n'y avait pas non plus de différence significative entre la déperdition sanguine pendant la césarienne sans la myomectomie et la césarienne avec la myomectomie quand on appliqué le tourniquet. (Rev Afr Santé Reprod 2002; 6[3]: 38–43) KEY WORDS: Caesarean myomectomy, tourniquet INTRODUCTION Myomectomy during caesarean section was relatively unknown in obstetric literature until the last decade. Oftentimes during caesarean sections obstetricians are confronted with large fibroids. Pedunculated fibroids could easily be removed and haemostasis secured without endangering the life of the mother. If the fibroids were located in the lower segment many obstetricians would readily perform a classical caesarean section and deliver the baby. But some obstetricians face the problem of taking emergency decision to remove or incise through them to deliver the fetus or leave them behind for interval myomectomy. In the non-pregnant state majority of fibroids are asymptomatic and confined to the pelvis and might not need any therapy. The major indications for aggressive management are abnormal uterine bleeding, rapid growth, growth after menopause, infertility, recurrent pregnancy loss, pain or pressure symptoms, menorrhagia, urinary tract symptoms or obstruction, iron deficiency anaemia secondary to chronic blood loss, and suspicion of sarcomatous change.1 During pregnancy, fibroids may also be asymptomatic but may undergo severe degeneration with pain, recurrent pregnancy loss, pressure symptoms or obstruction. The current teaching is to deliver the baby and perform interval myomectomy probably before the next pregnancy. This article presents the technique of minimal blood loss at caesarean section with elective myomectomy and compares it with caesarean section without myomectomy. PATIENTS AND METHODS The study was a prospective clinical trial of myomectomy done at caesarean section and compared with caesarean section without myomectomy at Korle Bu Teaching Hospital and Family Health Hospital, Accra, Ghana, between April 2000 and January 2001. Twelve patients with uterine fibroids who had caesarean section for various indications were selected. Any patient who also had caesarean section immediately after a patient with uterine fibroid who had caesarean section was also selected to serve as control. In all, 24 patients were recruited into the study. Parameters considered were age of patient, parity, pre and post-haemoglobin levels, duration of operation, blood loss, duration of application of tourniquet and number of weeks before the next menses. Intra-operative blood loss was measured using a graduated cylindrical flask connected by a rubber tube into the operating field. Blood from the operating field, paracolic gutters, anterior to the uterus and Pouch of Douglas was sucked into the graduated cylinder using a vacuum pump. Blood from the soaked packs was squeezed into a kidney disk and sucked into the graduated cylinder. Total blood loss was then measured from the cylinder and recorded. All the patients were antenatal attendants at the hospitals and had ultrasonography during pregnancy. Diagnosis of fibroids was made on physical examination and confirmed by ultrasonography. All the patients had daily iron tablets and weekly daraprim during their antenatal period. They also had prophylactic antibiotic, augmentin 1.2g, during induction of anaesthesia. This was repeated after 12 hours. Exclusion Criteria
Surgical Technique used for Caesarean Section and Myomectomy
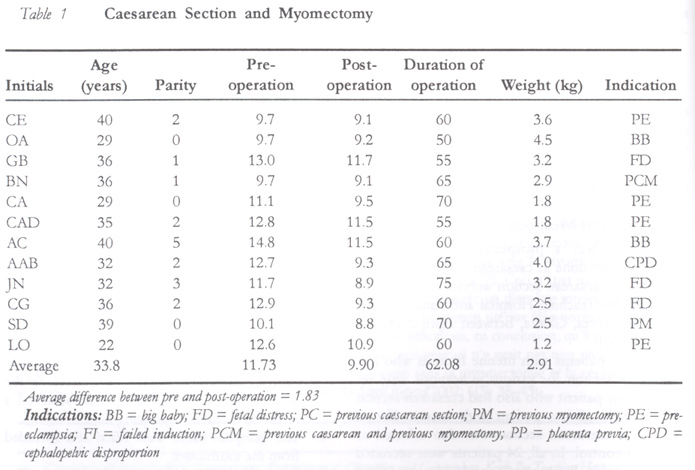
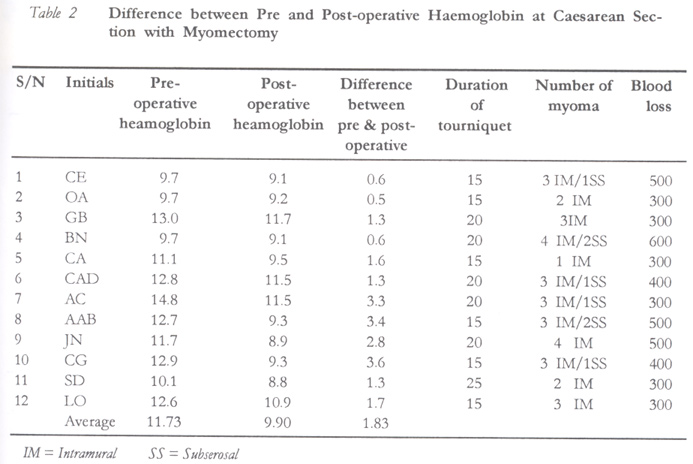
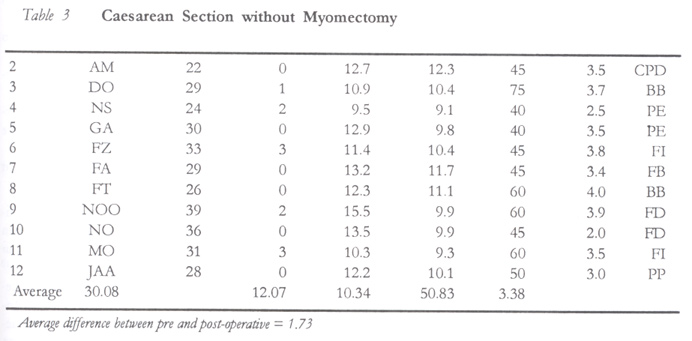
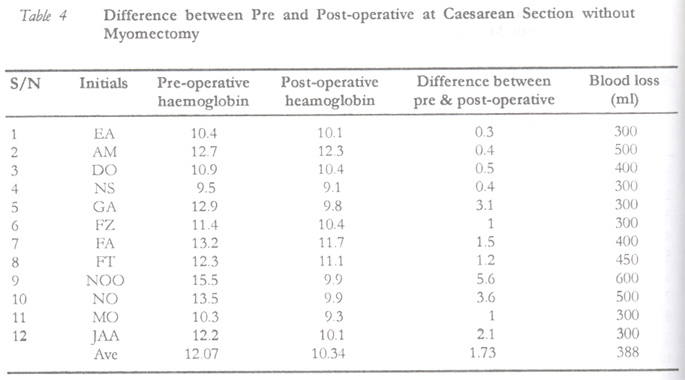
RESULTS The characteristics of the patients including age, parity, pre and post-haemoglobin levels, birth weight, Apgar score, blood loss, duration of application of tourniquet and duration of operation are shown in Tables 1, 2, 3, 4. Table 1 shows patients who had caesarean section with myomectomy. Table 3 shows patients who had caesarean section without myomectomy. The average age of patients who had myomectomy and caesarean section was 34.5 years, higher than those patients who had caesarean section alone (30.2 years). This might be because fibroids are associated with older age.2 The average haemoglobin of the patients both pre and post-operatively was 11.73g/dl and 9.90g/dl for those patients who had caesarean section with myomectomy and 12.07g/dl and 10.34g/dl in the control group. The average duration of operation was longer in those who had caesarean section and myomectomy (62.08 mins) than in the control group (50.83 mins), but was not significant. The fibroids removed ranged from one to six nodules. They were mainly intramural and in the body of the uterus as shown in Table 2. The fibroid nodules put together weighed about 500g in a patient in whom the largest number of fibroids was removed. Uterine involution using symphysio-fundal height was normal and there were no significant complications during the puerperium. All patients were discharged on the fifth day after caesarean section. The duration of return of menses ranged from two to twelve months. This might be attributed to breastfeeding practices in the hospital. Pre-operative haemoglobin levels were measured within one week of the operation and post-operative haemoglobin estimation was done on the third day after operation. DISCUSSION Caesarean section has become one of the commonest hospital-based operative procedures in Ghana. The rate has increased from 10% in 1970 to 20% in 1999.3-5 Certainly there has been a change in obstetric practice and various reasons might be adduced such as liberalisation of indications for “fetal distress”, a lower tolerance for taking risks, breech presentations and various reasons for elective repeat caesarean sections. Fibroids vary in size and shape, from seedlings to large uterine tumours that may not only fill the pelvis but also extend to the upper abdomen. These tumours may be solitary or multiple.6-8 Fibroids are benign uterine tumours that are composed of smooth muscle and connective tissue elements. They are the commonest pelvic tumours in the female especially in African women. The exact incidence is unknown, but traditionally it is estimated as 20% of women above 35 years. At post-mortem the incidence of fibroids is much higher, reaching about 50% of women.9 Myomectomy at caesarean section has many advantages such as:
As seen from this study, there was no statistically significant difference in blood loss between patients who had myomectomy during caesarean section and the control group. In a similar study10 myomectomy as a separate operation during caesarean section increased haemorrhage by 10%. Another study11 reported severe haemorrhage at caesarean section in ten patients, three of whom needed hysterectomy. Hsieh et al12 also recorded 112ml blood loss during the operation. The minimal blood loss in our study compared to the greater loss in other studies might be due to the application of the tourniquet, which occluded the uterine arteries and vessels in the infundibulo-pelvic ligament thus effectively reducing blood loss. There was no intra-operative or post-operative blood transfusion and no patient had caesarean hysterectomy because of the application of the tourniquet. The blood lost during surgery might not necessarily reflect on the procedure of myomectomy during caesarean section since surgical procedures during the caesarean sections themselves might result in greater amount of blood loss. In addition, liquor volume might be added to the estimated blood loss since the method of estimation of blood loss could not strictly exclude liquor volume. The average age of those who had caesarean section and myomectomy was 34.5 years, similar to that in another study (33.4 years),11 and were higher than the control group (30.2 years), probably because fibroids become common with increase in age.2 The birth weights of patients who had caesarean section and myomectomy were lower than the control group and might be attributed to the presence of fibroids, but they were normal for Ghanaian neonates.13 In the present study myomectomy added 11.25 mins to the operation time. This is similar to the report of other researchers,12 who reported 11 minutes being added to the time taken to complete myomectomy and caesarean section. Attempt should not be made to remove small fibroids and unnecessarily prolong operation time. Fibroids could be removed in the lower segment to help in closing up the uterine incision. In addition, fibroids in the fundus and body of the uterus could also be removed without any significant loss of blood if the above technique is applied properly. Myomectomy was not performed on one patient who had a previous myomectomy and two previous caesarean sections because of extensive adhesions. It is advised that if extensive adhesions are encountered during caesarean section, adhesiolysis should not be performed to gain access to the fundus of the uterus. Interval myomectomy should rather be performed. Adhesions encountered while entering the abdomen should be removed as usual to gain access to the lower segment. It is recommended that more research should be carried out by doctors on myomectomy at caesarean section with the application of the tourniquet in order to have further insight on how to improve the technique. This is essential in Africa where fibroid is common. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02033t4.jpg] [rh02033t2.jpg] [rh02033t1.jpg] [rh02033t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}