 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
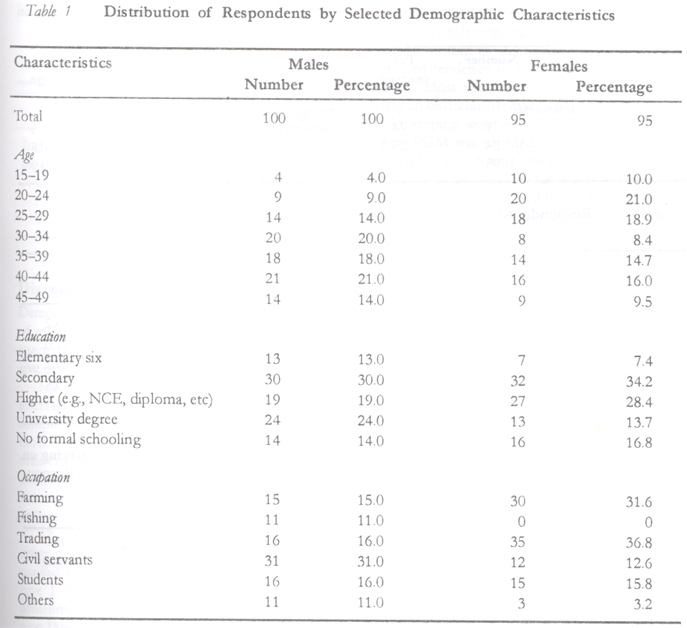
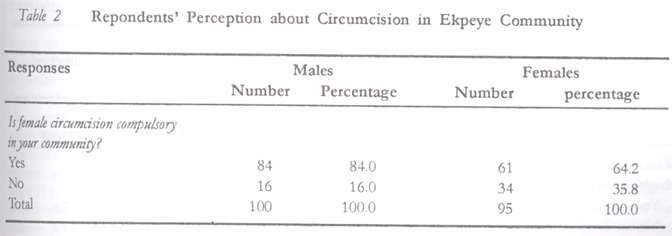
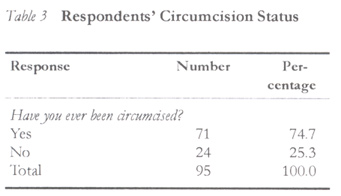
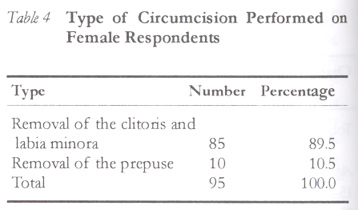
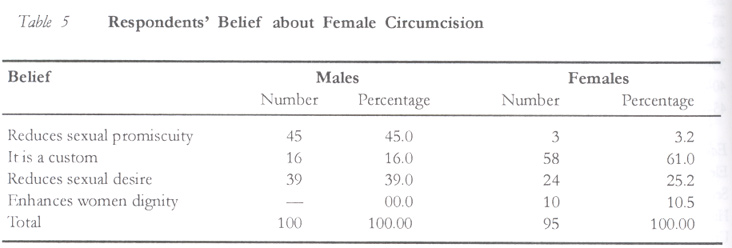
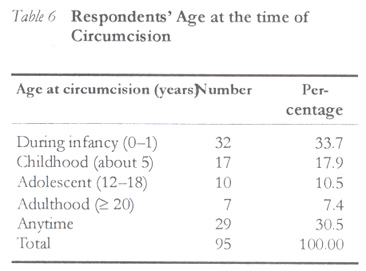
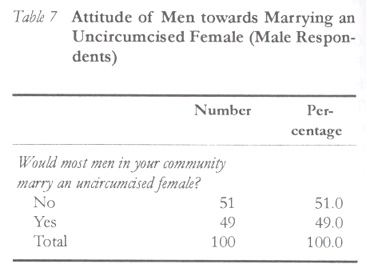
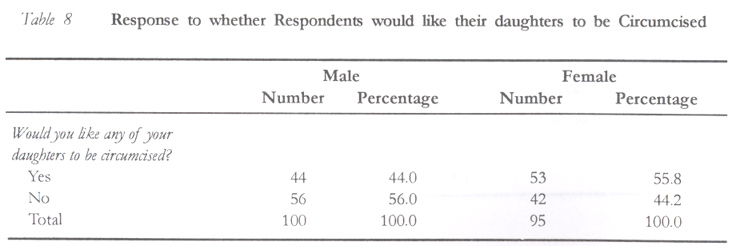
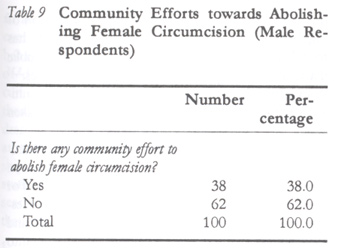
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 44-52 Male and Female Viewpoints on Female Circumcision in Ekpeye, Rivers State, Nigeria LA Briggs Correspondence: Dr L. A. Briggs, Department of Human Kinetics, Health and Safety Education, Rivers State College of Education, Port Harcourt. Code Number: rh02034 ABSTRACT One hundred and ninety five male and female volunteers across the social strata were interviewed using structured questionnaire. Data were analysed using frequency tables. The study revealed that 74.7% of female respondents were circumcised. They believe that the practice would help prevent sexual promiscuity, curb sexual desires and that it is a custom they cannot do without. Most of the men would not marry an uncircumcised female, while a substantial number of the respondents would like to circumcise their daughters. Community effort to eradicate the practice is very minimal. Based on the findings, it is suggested that communities where female genital mutilation (FGM) is practiced as a social norm should be involved in eradication campaigns with support from national and international organisations. (Afr J Reprod Health 2002; 6[3]: 44–52) RÉSUMÉ Les opinions des hommes et des femmes sur l'excision à Ekpeye, Etat de Rivers, Nigéria. Cent quatre-vingt quinze volontaires hommes et femmes, à travers les couches sociales, ont été intérrogés à l'aide d'un questionnaire structuré. Les données ont été analysées à l'aide des tables de fréquence. L'étude a révélé que 74,7% des répondantes ont été excisées. Elle croient que la pratique aiderait à prevenir la promiscuité sexuelle, à réduire les désirs sexuels et qu'il s'agit là d'une coutume indispensable. La plupart des hommes n'épouseraient pas une femme non-excisée, tandis que bon nombre de répondants aimeraient exciser leurs filles. Il y a très peu d'effort de la part de la communauté pour éliminer la pratique. En nous fondant sur les résultats, nous suggérons que les communautés dans lesquelles la mutilation génitale feminine (MGF) se pratique comme une norme sociale, doivent s'engager dans des campagnes d'éradication avec le soutien des organisations nationales et internationales. (Rev Afr Santé Reprod 2002; 6[3]: 44–52) KEY WORDS: Female circumcision, Sexual promiscuity, traditional rites INTRODUCTION The traditional operations that involve cutting away parts of the female external genitalia or other injury to the female genitals, whether for cultural or any other non-therapeutic reason, is called female circumcision (FC).1 The World Health Organization (WHO) and advocates of its eradication now refer to the operation as female genital mutilation (FGM), a term that more accurately describes the consequences of the procedure. In this paper, the terms FC and FGM are used interchangeably depending on the perception of participants but both mean the same. We have, however, adopted the term FGM since this is a scholarly paper. There are apparent harmful physical, psychological and human rights consequences of FGM. It is practiced in one form or the other in 28 African countries, in a few countries on the Arab Peninsula, among minority communities in Asia, and among migrants from these areas who have settled in Europe, Australia and North America.2-4 FGM is also thought to have been practiced at one time or the other in many western countries.3,5,6 Indeed, Baasher7 reported that the ancient ritual of FGM has been practiced in all continents of the world at one time or the other. Arbesman, Kahler and Buck8 estimated that 80 million women worldwide have undergone one type of circumcision or the other, and a variety of health risks resulting from the procedure such as severe bleeding, infection, shock, difficulties with menstruation and urination as well as painful intercourse have been reported. Hosken3, Toubia4 and UNICEF9 estimated that 100–132 million women now living have undergone the procedure and another two million procedures are done each year. According to Calder and Brown10, FGM is still a prevalent custom in some African countries. The practice of FGM has also become an issue for health care providers in the West because of increasing immigration of African families. Because practitioners in western countries may not have access to information necessary to ensure that circumcised women obtain medically and culturally appropriate health care while in western countries, Lightfoot-Klein and Shaw11 have discussed the urinary, gynaecologic and obstetric complications, including a Sudanese physician's protocol recommended to avoid tearing, during the delivery of a neonate. However, there are now organisations in western countries dealing with FGM among recent immigrants. For instance, in London the government-funded Foundation for Women's Health Research and Development and the London Black Women's Health Action Project; and in France, Group Femmes Four L'Abolition des Mutilations Sexuelles (GAMS) and Commission Pour I'Abolition des Mutilations Sexuelles (CAMS) have raised the issue of FGM for national and international discussion. Along with public information and advocacy campaigns, they are active among migrant communities providing information and counselling families.2,12,13 Also, Black and Debelloe14 stated that the UK has incorporated FGM prevention into its child protection laws, and this has been used successfully in the courts to protect some girls from genital mutilation. There is no special law against FGM in France, but CAMS has successfully used existing sections of the penal code on violence against children to persecute circumcisers or parents who have submitted their girls to FGM.13,15 Also, a strong campaign against FGM supported by medical and health personnel is underway in Canada.16 In Nigeria, female circumcision is still widely practiced. Local Inter-African Committee (IAC) affiliates spearhead anti-FGM work and train traditional birth attendants (TBAS) who in turn train their colleagues all over the country. According to Modupe and Lola17, among 453 women and 28 men interviewed in Ibadan, Nigeria, 71.3% of the women had been circumcised and almost half of them (48%) had their last female child circumcised. About 67% of respondents who favoured the practice gave their reasons as maintenance of strong cultural traditions, reduction of sexual promiscuity, prevention of prenatal mortality and reduction of excessive vaginal secretion. Briggs'18 study also confirms the role played by culture in perpetrating FGM in a community where the practice is compulsory. BACKGROUND The objectives of the study are specifically to examine males' and females' attitude towards female circumcision; community belief about female circumcision, whether circumcision is still compulsory and community effort towards its eradication. The Ekpeye ethnic group of Ahoada East Local Government Area of Rivers State is made up of four sub-divisions, namely, Ehida, Ula, Odiemerenyi and Ekpena with an estimated population of over 50,000 inhabitants. They occupy a lowland rainy forest area of Nigeria. The main occupation of this ethnic group are fishing and farming. They also involve in petty trading that makes up the economic life of the people. For generations, it has been a custom among the Ekpeye to circumcise their female folks. In the past, an uncircumcised female was usually ostracised and hides in shame. DATA AND METHODOLOGY One hundred male and one hundred female volunteers were interviewed by means of structured questionnaires with the assistance of a final year student who was also circumcised. The questionnaires were in two parts, each designed for males and females. Apart from the socio-demographic data, questions eliciting respondents' attitude towards circumcision, reasons for circumcision and whether respondents would circumcise their daughters were asked. Isolated questions for males, such as whether they would refuse to marry an uncircumcised female and community effort to abolish female circumcision were also asked. An attempt was made to interview males and females from across the social strata, reflecting age and educational background. All one hundred questionnaires from the males were returned while only ninety five females returned their questionnaires, which were used for data analysis. Data collected were analysed using frequency tables. FINDINGS Table 1 shows the percentage distribution of the sample by selected socio-demographic characteristics. The mean age of male and female respondents was 34.8 and 31.0 years respectively with 59.5% males between 30 and 44 years and 50.5% of females between 15 and 29 years. With regard to education, a greater proportion of the males (43.0%) than females (42.1%) had higher education such as National Certificate of Education, diplomas and university degree. Also, 30.0% and 33.7% of males and females respectively had secondary education, while 13.0% of males and 7.4% of females had elementary education. However, 14.0% of males and 16.8% of females did not attend any formal school. The occupation of respondents differed; 31.0% of males were civil servants while 36.8% of females were traders. A higher proportion of females (31.6%) were farmers compared to 15.0% of males. Sixteen per cent and 15.8% of the respondents were students. Table 2 shows that majority (84.0% of males and 64.2% of females) felt that female circumcision is compulsory in the study environment and Table 3 shows that most of the respondents (74.7%) said that they were circumcised. Table 4 indicates that the type of circumcision commonest among the study participants was the removal of the clitoris and labia minora (89.5%). Table 5 shows respondents' belief about female circumcision. A greater proportion of males (45.0%) said circumcision reduces sexual promiscuity while the female respondents (61.0%) said custom is responsible for the prevalence of the practice in the community. More males (39.0%) than females (25.2%) believed that circumcision reduces sexual desire. Table 6 shows that circumcision was performed on female respondents during infancy (33.6%) and anytime (30.5%), while Table 7 shows that most (51.0%) of the respondents reported that most men in the community would not marry a woman who is not circumcised as against 49.0% who think otherwise. Table 8 shows that 55.8% of female and 44.0% of male respondents would circumcise their daughters. In Table 9, 62.0% of the respondents stated that no community effort has so far been initiated towards abolition of female circumcision, while 38.0% said there has been community effort towards its abolition. Such efforts, they said, were initiated by government and the medical association (31.5%), socio-cultural groups (23.7%) and churches (13.2%). DISCUSSION Demographic analysis indicates that the mean age of males and females were 34.8 and 31.0 years respectively. These are matured age groups likely to give objective responses to the study questions. Majority (84.0% of male and 64.2% of female interviewees) stated that female circumcision is compulsory in the study environment. In recent times women groups have advocated against female circumcision and have tried to reach communities where the practice is common through the mass media. It is noteworthy that 74.7% of the female respondents had been circumcised. The findings also revealed the type of circumcision performed on participants. The WHO categorised FGM into four, types I, II, III and IV. In type I the prepuce (clitoral hood) is removed, sometimes along with part or the entire clitoris. In type II both the clitoris and part or the entire labia minora (inner vaginal lips) are removed. In type III (infibulation) the clitoris is removed, some or all of the labia minora is amputated, and incisions are made on the labia majora (outer lips) to create a raw surface. These raw surfaces are either stitched together and/or kept in contact until they seal as a `hood of skin' covering the urethra and most of the vaginal opening. Type IV involves other operations on the external genitalia, including the introduction of corrosive substances and herbs into the vagina, and similar practices. In this study, it seems type II (removal of the clitoris and labia minora) is mostly practiced. As for the age at which circumcision is performed, analysis shows that it could be done at anytime from infancy. Findings indicate that 84.0% of male and 61.0% of female respondents said female circumcision is a custom in the community because of its perceived tendency to curb sexual desires among women. Most men in the community would not marry an uncircumcised woman. In keeping with the findings of Modupe and Lola,17 FGM was justified by participants because they feel that it forms the basis for socialisation into womanhood and it curbs female sexual desires. This is also supported by the findings of others.3,4,19,20 It seems women are rewarded for the practice in terms of social recognition and status.9,21,22 Undoubtedly, one of the main factors behind the persistence of FGM is its social significance for females. In most regions where it is practiced, a woman achieves recognition mainly through marriage and childbearing and men may refuse to marry a woman who has not been circumcised. Therefore, to be uncircumcised is to have no access to status or a voice in these communities. In this study, 55.8% of females and 44.0% of males would like their daughters to be circumcised. Ntiri's23 study in Somalia reaffirmed the special significance of FGM as a symbol of full womanhood and an instrument for the control of female sexuality. As was observed by the joint report of the World Health Organization and the International Federation of Gynaecology and Obstetrics (FIGO), victims of the practice are often its strongest proponents.24 Another finding in the study also indicates that a greater number of respondents (62.0%) stated that there was no community effort towards abolishing female circumcision in Ekpeye. However, community efforts involving the government, medical practitioners, socio-cultural groups and the churches were reported by 38.0% of the male subjects. Although these efforts have no proof of total eradication, the ground work has been initiated as a strategy for its eradication. The success of the community effort is yet to be ascertained. It is a laudable development that women advocacy groups have placed FGM on the agenda of government as well as regional and international organisations. The WHO25, UNICEF9, UNFPA26, USAID27 and FIGO24, among others, have condemned the practice. The 1994 International Conference on Population and Development (ICPD)28 held in Cairo spotlighted the matter in conference recommendations urging governments to prohibit FGM wherever it exists and to give vigorous support to efforts among non-governmental and community-based organisations and religious institutions to eliminate it. There have been specific laws against FGM in Belgium, Ghana, Sweden and the UK.13,14,29 In France and Canada, the operation is illegal under existing child abuse laws.3,15,16,29 There is some type of regulation against FGM in Burkina Faso, Uganda and possibly other African countries.13 Legal options are under review in Australia and the US3,29,30, and in Eritrea recent civil reforms have banned FGM.2 In Egypt, anti-FGM initiatives led by the Egyptian Task Force Against FGM and the Egyptian Society Against Practices Harmful to Women and Children have programmes in nursing schools, women's associations, health care facilities and the mass media.3,31 Similar activities have also been undertaken in Sudan.2,3 Because FGM is so entrenched in some societies, including Nigeria, legal decrees and policy statements alone are unlikely to abolish it. For example, resolutions against the practice were signed in Egypt in 1959 and a law was passed by the British colonial government in Sudan in 1946, yet it persists.32 However, the 1946 law in the Sudan no longer exists. It seems changes in social norms are necessary for long-lasting results. To this end, some grassroots community education and advocacy groups have taken the lead in ongoing reform efforts. The largest of such groups, the Inter-African Committee on Traditional Practices Affecting the Health of Women and Children (IAC) received the 1995 United Nations Population Award in recognition of its work.26 In Burkina Faso, the government's National Committee Against Excision has used the broadcast media, video, film and other educational materials to teach the public.3 Similarly in Kenya, the largest women's organisation, Maendeleo ya Wanawake Organization (MYWO), is at the forefront of anti-FGM activities. According to Mohammed33, the Population Action International (PAI)34, MYWO, with the assistance from the Programme for Appropriate Technology Health (PATH) and PAI has conducted research on FGM in various areas and is now mounting a public education campaign. Similar anti-FGM activities have taken place in Mali3, Tanzania, Sudan and Somalia.2,3,30 In Nigeria, the National Association of Nigerian Nurses and Midwives (NANNM) has mobilised its members to educate the public through plays, skits and other live performances.3,35 Also, the Family Support Programme (FSP) initiated by the Nigerian military government has taken keen interest in educating women against FGM. The MYWO in Kenya encouraged communities to find healthy alternatives to genital mutilation without giving up its social and ritual aspects. For example, by providing a rite of passage for adolescent girls including the celebration, gift giving and recognition that are key to traditional passage into womanhood, while omitting the actual operation.36 In Sierra Leone, the Kenewas Project worked with opinion leaders of the secret circumcision societies to educate them about the harmful effects of FGM and to encourage them to allow adolescents to go through ceremonies without the harmful operations. The project also encourages young men to pledge that they would not insist on marrying only circumcised women, and young women to pledge that they would not circumcise their daughters.30,35 In order to reduce opposition from practitioners by giving them alternative employment, one project in Ghana trains circumcisers to become traditional birth attendants, while another in Ethiopia trains them in sandal-making and bread-making.12 CONCLUSION This paper has confirmed that FGM is practiced in Nigeria and explains underlying reasons for its prevalence. Grassroots organisations fighting FGM need the support of national and international organisations since the practice is often at the heart of the community's belief, the community first must acknowledge its medical dangers before change can begin. Every human behaviour has a cause and all health conditions have behavioural correlates. It is critical, therefore, that members of the community participate in designing and conducting eradication campaigns.37 Furthermore, it should not be forgotten that in order to design effective reforms, more research is essential in understanding FGM. RECOMMENDATIONS Ekpeye is a traditional ethnic group with a defined culture different from its neighbours. Culture being an accumulation and development of experiences over many generations, has a deep influence on the behaviour of people. This study can form the basis of designing programme to eradicate female circumcision in the study environment. However, there are certain limitations that have to be addressed. For instance, the effect of education on attitudes of respondents and occupational relationship to female circumcision were oversights in the study, which need to be included in further research. Based on the findings, it is recommended that any eradication programme should:
ACKNOWLEDGEMENTS This work would not have been possible without the active cooperation of Miss Imo Patience, a final year student of Rivers State College of Education, I am greatly indebted to her. Miss Patience's interest was motivated by a course in sex education covering female circumcision and its implications. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02034t4.jpg] [rh02034t6.jpg] [rh02034t3.jpg] [rh02034t9.jpg] [rh02034t8.jpg] [rh02034t2.jpg] [rh02034t5.jpg] [rh02034t1.jpg] [rh02034t7.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}