 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 53-58 Intimate Partner Violence among Women of Childbearing Age in a Primary Health Care Centre in Nigeria Amobi L Ilika1, Prosper I Okonkwo1 and Prosper Adogu1 1Department of Community
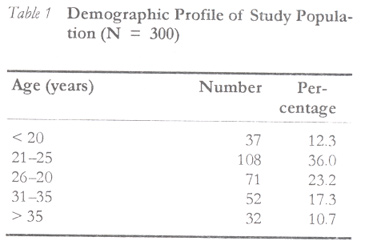
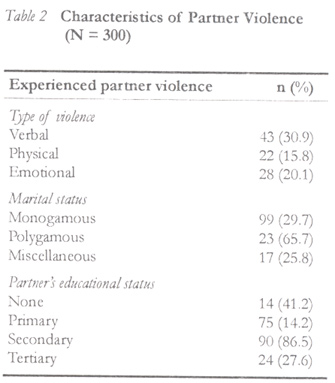
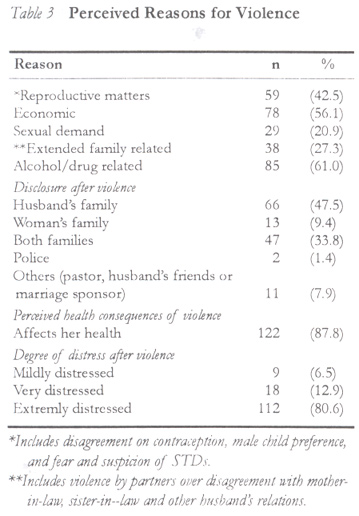
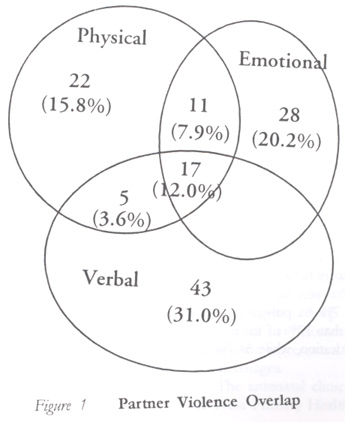
Medicine, Nnamdi Azikiwe University Teaching Hospital, Nnewi. Code Number: rh02035 ABSTRACT This study assessed the prevalence and characteristics of intimate partner violence among women of childbearing age in a primary health centre. With interviewer-administered questionnaire, information on partner violence was elicited from three hundred women of childbearing age selected by systematic sampling in a primary health care (PHC) centre. Over 40% had experienced violence within the last 12 months. Type of marriage and partner's education had effect on violence. Perceived reasons for violence were economic demand (56.1%), reproductive issues (42.5%), alcohol and drugs (61.2%). Forty eight per cent reported to family members. Only 1% reported to the Police. Intimate partner violence is a prevalent public health problem in eastern Nigeria. Health workers and social organisations should recognise the problem and offer necessary support, and women should be empowered to navigate through the problem. (Afr J Reprod Health 2002; 6[3]: 53–58) RÉSUMÉ La violence du partenaire intime chez les femmes en âge d'avoir des enfants dans un centre des services médicaux primaries au Nigéria. Cette étude a etude a évalué la prévalence et les caractéristiques de la violence du partenaire intime chez les femmes en âge d'avoir des enfants, dans un centre des services médicaux primaries. A l'aide d'un questionnaire administé par l'intervieweur, nous avons recueilli des renseignements sur la violence du partenaire de trios cents femmes en âge d'avoir des enfants. Elles ont été selectionnées à travers un échantillon systématique dans un centre des services médicaux primaries (SMP). Plus de 40% avaient vécu la violence ces douze derniers mois. Le type de mariage et le niveau de scolarité du partenaire avaient un effet sur la violence. Les raisons perçues de la violence étaient l'exigence économique (15,1%), les questions de la reproduction (42,5%), l'alcool et la drogue (61,2%). 48% ont signalé aux members de famille. Seul 1% ont signalé à la police. La violence du partenaire intime est un problème de la santé publique prévalent à l'Est du Nigéria. Il faut que les Assistantes Sociales et les organisations sociales reconnaissent le problème et qu'elles offrent le secours nécessaire. Il faut également rendre les femmes capables d'affronter le problème. (Rev Afr Santé Reprod 2002; 6[3]: 53–58) KEY WORDS: Intimate partner violence, women, childbearing INTRODUCTION Violence against women has emerged as a focus of international attention and concern since 1993, when the UN General Assembly passed the declaration on the elimination of violence against women and offered the first official definition of such violence against women.1 Article one of the declaration defines violence against women as “any act of gender-based violence that results in, or is likely to result in, physical, sexual or psychological harm or suffering to women including threats of such acts, coercion or arbitrary deprivations of liberty, whether occurring in public or private life.2 Intimate partner violence is gender based and it is a very serious public health problem that cuts across nations, cultures, religion and class. Around the world, at least one in every three women has been beaten, coerced into sex or otherwise abused in her lifetime. Most often the abuser is a member of her own family. One of the most common forms of violence against women is abuse by their husbands or other intimate male partners.1 The effects of partner violence can be tremendous and devastating to the victim's physical and mental health. Partner violence affects the reproductive life of the woman and increases the risk of unintended pregnancy with associated adverse pregnancy outcomes. In addition to the immediate traumatic effects, it can give rise to other long-term problems including chronic pain, physical disability, drug and alcohol abuse, depression and suicide.1 The problem has been recognised internationally as a serious obstacle to development and peace and a violation of human rights 1. Partner violence affects the psychological welfare of the children who observe it among their parents and also the stability and general health of the family. Unfortunately, however, cultural norms seem to favour gender based violence and victims of intimate partner violence are least likely to report to the police or open up to health care workers to avoid breaking traditional norms or incurring community sanctions. Because intimate partner violence is a sensitive issue, community based household surveys and studies may pose the risk of aggravating further violence against the woman respondent or attack on the investigator from the suspicious violent partner.3,4 A primary health care setting offers a safer and freer environment for the woman to narrate her experiences without fear of her husband and with better assurance of confidentially.1 Intimate partner violence is a global problem and it is widely reported in many parts of the world including China, Parkistan and America.4-6 Though there is a dearth of literature on intimate partner violence in Nigeria, studies by Odujinrin7 and the Federal Ministry of Health/WHO survey8 in Nigeria reveal a high prevalence of wife battery in western Nigeria. Studies by Coker and Ritcher reveal high prevalence of intimate partner violence in Sierra Leone.9 Similar studies in Zimbabwe describe partner violence as a pervasive problem.10 Not much work seems to have been done among the Igbo of south-east Nigeria. This study is, therefore, an exploratory one on gender based violence to assess the prevalence and characteristics of intimate partner violence among women of childbearing age seeking care in a university primary health care centre. METHODOLOGY The study was done at the Nnamdi Azikiwe University Teaching Hospital Primary Health Centre at Neni. Neni is a rural community in Anambra State, the heart of Ibo-speaking states in south-east Nigeria. It is about 15km away from sub-urban Nnewi where the university's teaching hospital is situated. Marriage pattern in the area is mostly monogamous with some polygamous. There are, however, cultural practices such as ihachi nwanyi whereby a daughter is kept unmarried in the paternal home to bear children, or a widow does not remarry after her husband's death but continues to bear children for the dead husband (inolu di). The Ibo also practice wife inheritance, where a male relation inherits his deceased brother's wife and she bears children for him. Women who have no children or have no male child can also marry more wives to bear children for them if they have the means. These practices are considered necessary where there are no male children to keep the family name or where the family is threatened with extinction. Such groups are represented in this study as miscellaneous marriages. The antenatal clinic and infant welfare clinics of Neni Primary Health Centre, the study centre, holds every Tuesday and Wednesday respectively. Over a period of four months – January to April 2001 – three hundred women of childbearing age attending antenatal and infant welfare clinics at the primary health care centre were selected by systematic sampling. All the women of childbearing age who attended antenatal clinic and infant welfare clinic each day were given numbers. This formed the sampling frame from where every third woman was chosen, such that 8–10 persons were recruited during a clinic day until all the 300 women were recruited. The nature of the study was explained to the participants and their consent obtained. They were assured of confidentiality and counselling was provided to violence victims. The women were interviewed by the authors in the local language using pre-tested questionnaires that sought information on violence by intimate partners within the last twelve months. Questions such as episodes of fights, beating and whipping were asked to assess physical violence, while threats and reprimands sufficient to cause emotional disturbance such as lack of sleep or excessive crying were used to assess verbal violence. Emotional violence, as distinct from verbal violence, was assessed with questions related to punitive actions that involved no verbal or physical episode but was sufficient to cause emotional disturbance such as abandonment, refusal of food cooked by the woman, denial or withholding of sex or money for food, and sending her home to his mother or village to humiliate her. These are known cultural behaviours of men within marriage in the studied area and are considered normal instruments of exercising authority and discipline by the man. RESULT The result is presented in Tables 1 , 2, 3 and Figure 1. All the three hundred women of childbearing age were interviewed, giving a 100% response rate. Over 75% of the women were between the ages of 21 and 35 years. Over 60% were in monogamous marriage relationships, 11.7% in polygamous and 22% in miscellaneous. Less than 12% of the women's partners had no formal education, while 34.7% had secondary education. Forty six per cent of the women admitted having experienced partner violence in the last twelve months. Of the women who admitted experiencing violence, 15.1% had the experience once in the last 12 months, while over 70% had it more than once. Of the types of violence, 30% was verbal, 15.8% physical and 20.1% emotional. There was an overlap in the type of violence, as shown in the Venn diagram (Figure 1). There was more violence in polygamous (65.7%) than in monogamous marriages (47.7%). The difference was, however, not statistically significant (c2= 3.16, df = 1, p > 0.05) but there was significant difference between monogamous (49.7%) and miscellaneous marriages (c2 = 11.6, df = 1, p < 0.05). Women whose partners had secondary education experienced more violence (86.5%) than those whose partners had tertiary education (27.6%). The difference was statistically significant (c2 = 3.7, df = 1, p < 0.05). Perceived causes of violence were economic demands (56.1%), reproductive issues (42.5%), and alcohol and drug related issues (61.2%). Abused women most times reported to family members. A statistically significant number of women reported to their husband's family (p <0.05). Forty seven per cent reported to their husband's family, 9.4% to their own family, 37.8% to both families, and 7.9% to their pastor or husband's friends. Only 1% reported to the Police. Eighty seven per cent of abused women admitted that violence affected their health. On a Likert scale of not distressed to extremely distressed, 80.6% felt extremely distressed after an abuse. DICUSSION The study revealed a high prevalence (46.3%) of partner violence among women of childbearing age in the studied area. Thirty per cent experienced verbal abuse, 15.8% experienced physical abuse and 20.1% experienced emotional abuse. In a study in western Nigeria, Odujinrin7 found that up to 81% of women admitted having been abused. Coker and Ritcher observed that 66.7% reported having been abused in a study in Sierra Leone.9 The results in this study are comparable with other studies in Africa and other parts of the world where 10–50% of women reported being abused by male partners.1,5-10 The high percentage in this study is of particular importance because the study segment was pregnant women and lactating mothers attending antenatal and infant welfare clinics in Ibo tribe where it is culturally unacceptable to beat a pregnant or lactating mother. Higher figures would be expected, therefore, when all women are studied. What constitutes verbal violence was found to be subjective, and as some of the women regarded verbal violence as normal and culturally acceptable. We explained verbal violence as verbal encounter with threats or insinuations sufficient to cause the victim emotional disturbance such as lack of sleep or excessive crying. Further qualitative research is suggested to define and characterise verbal violence, as what constitutes verbal violence in one culture may be acceptable in other cultures. Emotional or psychological violence rate was 20.1%. One of the cultural practices peculiar to the Ibos is to send their perceived offending wives living with them in urban areas to the husband's home in the rural village as a punitive measure. The woman could be humiliated further by sending her to her father's compound. This creates some stigmatisation on her part and could cause severe psychological problem; the woman looses self-esteem. This is mostly felt when the woman is economically disadvantaged, unemployed and uneducated. Empowering women through education and employment will help reduce the incidence of such emotional violence. Type of marriage was found to influence partner violence. Violence was found to be higher (66.7%) in polygamous than in monogamous marriages (49.7%). The difference was however not statistically significant. Men in polygamous marriages were more likely to find it difficult to cope with the economic demands and inter-rivalry conflicts often found in polygamous homes. Some of the women actually admitted that they had been beaten because of the other woman. There was statistically significant difference between levels of violence in miscellaneous and polygamous marriages, and in miscellaneous and monogamous marriages. The peculiar nature of miscellaneous marriages may be responsible for this difference. Partner's education was found to have effect on prevalence of violence. There was more violence against women whose partners had secondary education (86.5%) than against those with tertiary education (27.6%). The difference was statistically significant. This observation is comparable to other studies.4 There was, however, less violence against women whose partners had no education (41.2%) than against those with secondary education (86.5%). This observation needs to be investigated further through qualitative studies. Reasons for violence include economic demand (56.1%), reproductive issues (42.5%) alcohol/drug related issues (61.2%). This is comparable with studies elsewhere.4-6,9 One issue of great cultural importance was fertility and male child preference. Women who had no male children had more risks of all types of violence, as the women were said to be responsible for not giving birth to male children. Male children are regarded as very important to keep the family name. Such women are more likely to have a larger number of unintended or unwanted pregnancies, coerced sex and poor spacing of pregnancies with high-risk morbidity and mortality. Some of the women reported that they were abandoned in the hospital with their female babies, a situation that gave them severe emotional distress. Over 60% of the abused women associated alcohol use with the violence. This is consistent with the findings of Coker and colleagues in USA.12 Use of alcohol has been associated with staying out quite late into the night and away from home, and evoking suspicion of infidelity and jealousy which trigger partner disharmony and violence. All the women reported violence to someone. A statistically significant number reported it to only their husband's family while others reported it to their own family members. Only 1% reported to the police. This is in contrast to studies in developed countries where 20–26% of respondents reported to the police.1 This is probably because it is culturally not acceptable to report family matters to the police and the perception or apprehension that the police might not be able to solve their problem. The weakness or inability of social organisations, the police and medical services who are in positions of responsibility to provide support to abused women was extensively discussed by Heise and colleagues.1 The high percentage of those reporting (33.8–47.5%) to family members and to pastors and friends of the husband (7.9%) is in line with the norms among the Igbo extended family system and social organisation where marriage is regarded as an issue that involves the community and not just a personal affair. This attitude should be exploited in planning intervention programmes. Sensitising the community and soliciting community action could be effective public health intervention options to reduce partner violence. The fact that all women in the study would report experience of violence to someone else suggests that the abused woman really would want a reliable person to talk to both for psychological relief and for intervention. This reinforces the argument for health care providers to inquire about domestic violence from clients and provide necessary support. Over 87% of the abused women admitted that violence affected their health. About 80% felt extremely distressed after episodes of partner violence. Studies in Nicaragua13 and Pakistan5 showed that women who had been abused suffered more depression than women who had not been abused. Severe emotional distress, depression, contemplation of suicide and phobia have been identified with victims of intimate partner violence.7 CONCLUSION The study shows that intimate partner violence is a serious public health problem prevalent in eastern Nigeria. The prevalence is, however, comparable to that of other developing countries. There is need for health workers and social organisations to recognise the problem and offer necessary support to the victims and for women empowerment to navigate through the problem. ACKNOWLEDGEMENT Part of this paper was presented at the scientific conference of the Association of Community Physicians of Nigeria held at Enugu in August 2001. I wish to thank Prof. Kale and Prof. Asuzu of the University College Hospital, Ibadan, and Dr Edet of Shell BP for their valuable suggestion. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02035t3.jpg] [rh02035t1.jpg] [rh02035t2.jpg] [rh02035f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}