 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
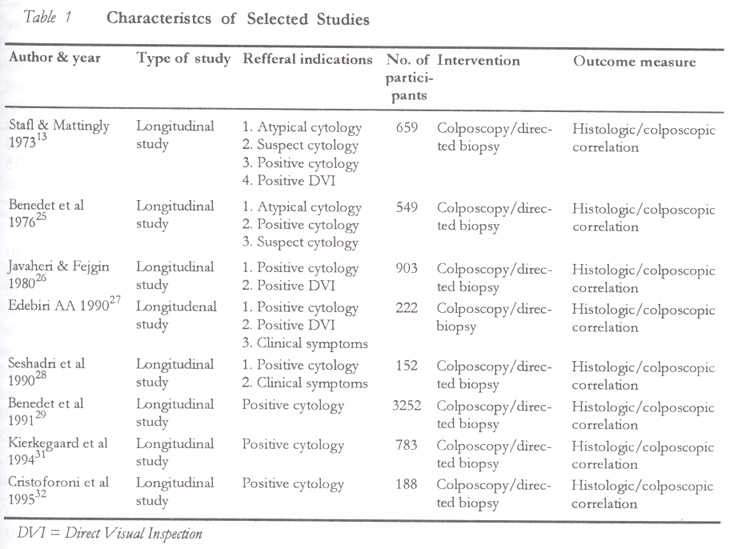
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 59-69 Validity of Colposcopy in the Diagnosis of Early Cervical Neoplasia – A Review Olayinka Babafemi Olaniyan Correspondence: Dr O. B. Olaniyan, Department of Obstetrics & Gynaecology, National Hospital, PMB 425, Abuja, Nigeria. E-mail: yolaniyan@yahoo.com Code Number: rh02036 ABSTRACT This study was conducted to quantify by meta-analysis the validity of colposcopy in the diagnosis of early cervical neoplasia in order to assess the justification of its integral role in this regard. Eight longitudinal studies were selected, which compared correlation of colposcopic impression with colposcopically directed biopsy results. The prevalence of disease in the studies ranged from 40 to 89%. Colposcopic accuracy was 89%, which agreed exactly with histology in 61% of cases. The sensitivity and specificity of colposcopy for the threshold normal versus all cervical abnormalities were 87–99% and 26–87% respectively. For the threshold normal and low grade SIL versus high grade SIL, the values were 30–90% and 67–97%. Likelihood ratios increased with disease severity. Colposcopy performed better in differentiation of high grade from low grade disease than in differentiation of low grade disease from normal cervix. Colposcopy is a valid tool for the diagnosis of early cervical neoplasia. Its integral role in the management of early cervical disease is justified. (Afr J Reprod Health 2002; 6[3]: 59–69) RÉSUMÉ La validité de la colposcopie dans le diagnostic de la néoplasie cervicale précoce: compte rendu. Cette étude avait pour but de quantifier, à l'aide de l'analyse meta, la validité de la colposcopie dans le diagnostic de la néoplasie cervicale précose afin d'évaluer la justification de son rôle intégrant à cet égard. Huit études longitudinales ont été selectionnées pour comparer la corrélation de l'empreinte colposcopique avec les résultats de la biopsie colposcopiquement orientées. La prévalence de la maladie dans les études variait de 40% à 89%. La précision colposcopique était 89%, ce qui s'accorde avec l'histologie dans 61% de cas. La sensibilité et la spécificité de la colposcopie pour le seuil normal par rapport à toutes les anormalités cervicales étaient 87–99% et 26–89% respectivement. En ce qui concerne le seuil normal et le SIL de qualité inférieure par rapport à SIL de haute qualité, les valeurs étaient 30–90% et 67–97%. L'indice de probabilité a augmenté avec la sévérité de la maladie. La performance de la colposcopie était meilleure quant à la différenciation d'une maladie de haut degré d'une maladie de degré inférieur, que dans la différenciation d'une maladie de degré inférieur du cou normal. La colposcopie demeure un outil valable pour le diagnostic de la néoplasie cervicale précoce. Son rôle intégrant dans le traitement de la maladie cervicale précoce est donc justifié. (Rev Afr Santé Reprod 2002; 6[3]: 59–69) KEY WORDS: Colposcopy, cervical intraepithelial neoplasia, cervical cancer, colposcopic accuracy INTRODUCTION Hans Hinselmann1 in 1925 introduced colposcopy as a clinical method of studying the morphological features of various cervical diseases. It is a system that allows magnification, usually 6-40 fold of the cervix, and illumination, with a primary aim of diagnosing cervical cancer in its earliest stage. It is perhaps of interest that the colposcope predates the Papanicolaou (Pap) smear – exfoliative cytology, which was introduced by Papanicolaou and Traut in 1941.2 Hinselmann originally used colposcopy as a screening method for cervical neoplasia, but his complicated nomenclature and controversial opinions on morphogenesis of cervical cancer were responsible for the reluctance of other gynaecologists in accepting colposcopy.3 When Pap smear was introduced as a screening method for cervical cancer in 1941, it was thought to supersede colposcopy entirely. Although Pap smear has become the accepted method of screening for cervical neoplasia all over the world, with significant decrease in cervical cancer incidence and death rates in the areas where mass screening was organised, widespread and prolonged4,5, the major drawback of the Pap smear has been its lack of sensitivity, with reports of false negative rates ranging from as low as 1.5% to as high as 80%.6-9 This is largely attributed to errors of sampling and interpretation.10-12 Eventually, the complementary use of cytology and colposcopy for the identification and evaluation of women at risk of cervical intraepithelial neoplasia and its precursors was thought to secure the highest yield of detection of cervical neoplasia.13,14 The management strategy for women with abnormal cervical smears varies widely. While most authorities agree that patients with significant degrees of cervical intraepithelial neoplasia (CIN) require colposcopic evaluation and biopsy, opinions differ regarding recommendations for the follow-up of the minimally abnormal smears. While it is recommended that women presenting with lower grades of squamous intraepithelial neoplasia be referred for definitive diagnosis by histology of a coloposcopically directed biopsy, a more conservative strategy of cytological surveillance has also been suggested.15 The assessment of women presenting with abnormal cervical cytology and the selection of those who are suitable for local ablative therapy relies on colposcopic assessment of the cervical transformation zone and histological appraisal of a directed punch biopsy. The role of colposcopy is to identify the most atypical site for biopsy in these patients. Fundamental to such a management strategy is the assumption that the colposcopist can identify accurately the area of most severe epithelial abnormality from which to take a punch biopsy.16 Colposcopic assessment is thus a critical stage in the diagnosis of early cervical neoplasia, as the detection of abnormal cervical cytology is dependent on precise visual localisation of micropathological changes and precise biopsy of such tissue for subsequent histopathologic diagnosis. Colposcopy thus plays a crucial role in the diagnosis of early cervical disease, with management decisions often anchored on the colposcopic assessment. However, the ability of the colposcopist to determine accurately the severity of intraepithelial lesions and even to diagnose early invasion has been questioned.17 The objective of this study was to quantify the degree of correlation of colposcopic assessment with the reference or `gold standard' of histologic diagnosis as an indicator of the validity of the colposcopic assessment, and thus assess the justification of its critical role in the diagnosis of early cervical disease. METHODS Literature Search Criteria Both electronic and manual literature searches were done to gather relevant published studies. A Medline search was conducted for articles published between January 1966 and July 2000. The search was limited to articles published in English language only. In addition, references from retrieved articles were followed up manually as a source for further relevant articles. Two hundred and fifty four reports were obtained from the initial search. The abstracts were examined and those studies that clearly did not meet the inclusion criteria were excluded. Fifty two articles were eventually identified as potentially meeting the selection criteria. Full text formats of these articles were retrieved and reviewed in detail. Inclusion criteria for the selection of articles were as follows: (a) Only original articles were selected. This was done to assess the methodology that was employed in the study. Articles that reported work done by other people would not assure that the selection criteria had been met. (b) Colposcopy was done as a diagnostic procedure following referral and not for screening purposes. The reason for this was two-fold, first it ensured that a high prevalence population is studied and secondly it was the `standard' use of colposcopy in the normal clinical setting. (c) Biopsy specimen was generated by directed biopsy. This was necessary to truly assess the ability of the colposcopist to recognise the lesion. (d) A colposcopic impression was clearly recorded before biopsy outcome and there was presentation of adequate data showing in tabular form the colposcopic impression compared with the final histologic diagnosis for the various disease categories. This ensured that data needed for statistical analysis was provided. Exclusion criteria were as follows: (a) Unsatisfactory colposcopy. Such studies were excluded because unsatisfactory colposcopy implies that a definitive colposcopic impression could not be made prior to subsequent biopsy, therefore, there would be no basis for comparison. (b) If colposcopy was used as a follow-up of previous treatment of cervical disease. This was to eliminate a potential source of `work-up' bias. (c) If colposcopy was limited to evaluation of a pre-determined cohort of patients, e.g., HIV positive patients, pregnant patients, or only patients with a particular group of abnormal smears, because such a study would distort the comparative nature of the intended study population. Most of the studies were rejected because they only presented summary results and did not provide raw data to enable statistical analysis.18-21 One large study was excluded because it grouped together CIN grade I–III.22 Another study was rejected because the number of patients assessed was extremely small, with less than 10 subjects in most disease groups.23 A study that included male participants and those with history of previous treatment for cervical disease was also excluded.24 Overall, eight articles met the selection criteria and were subjected to meta-analysis based on their comparative nature. The characteristics of these articles are summarised in Table 1. The outcome measured was the correlation between colposcopic impression and histologic diagnosis as measured by statistical references, with histologic diagnosis as the criterion standard. Terminology, Data Tabulation and Analysis Colposcopic impression refers to the colposcopist's opinion as to the nature of the underlying lesion based on classic colposcopic features. Histologic diagnosis refers to the report of the histologist on the colposcopically directed biopsy specimen. For ease of cross reference, the terminology used for categorisation of grades of abnormality is the Bethesda system33, to which earlier classification systems were converted. Thus, for studies reported using CIN terminology, human papillomavirus (HPV) infection and CIN I were regarded as `low grade squamous intraepithelial lesion' (LSIL) while lesions of CIN II and higher grades were grouped together under the category `high grade squamous intraepithelial lesion' (HSIL). Where biopsy results indicated a `normal' or `atypical' report, it was classified as `disease absent'. All cases of HPV and CIN were classified as `disease present'. Cases of carcinoma in situ, microinvasive carcinoma or frank invasion could not be separately stratified and were grouped together with high grade lesions due to their low numbers. By pairing colposcopic-histologic findings, each coloscopic impression was placed in one of four possible categories, namely, true positive (TP), false positive (FP), true negative (TN) and false negative (FN). The parameters used to assess the validity of colposcopy were as follows:
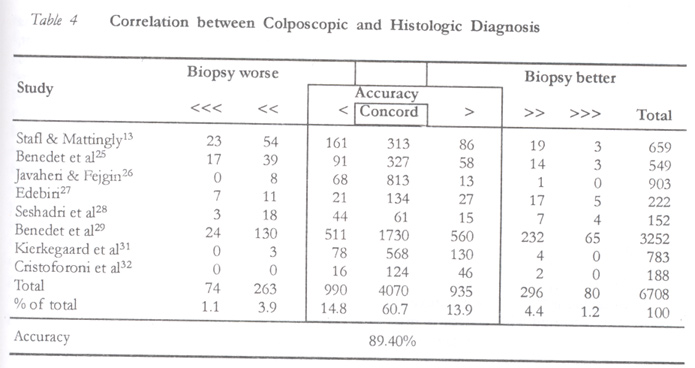
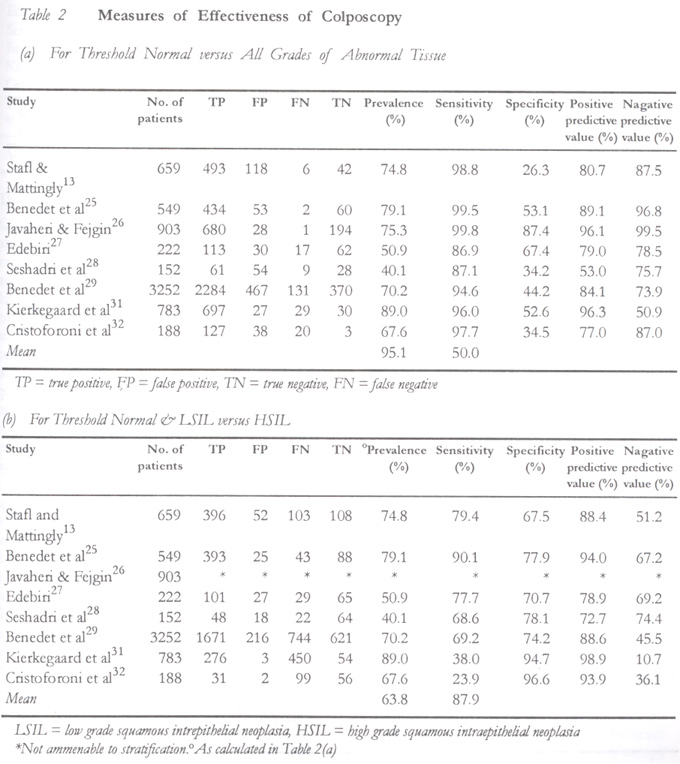
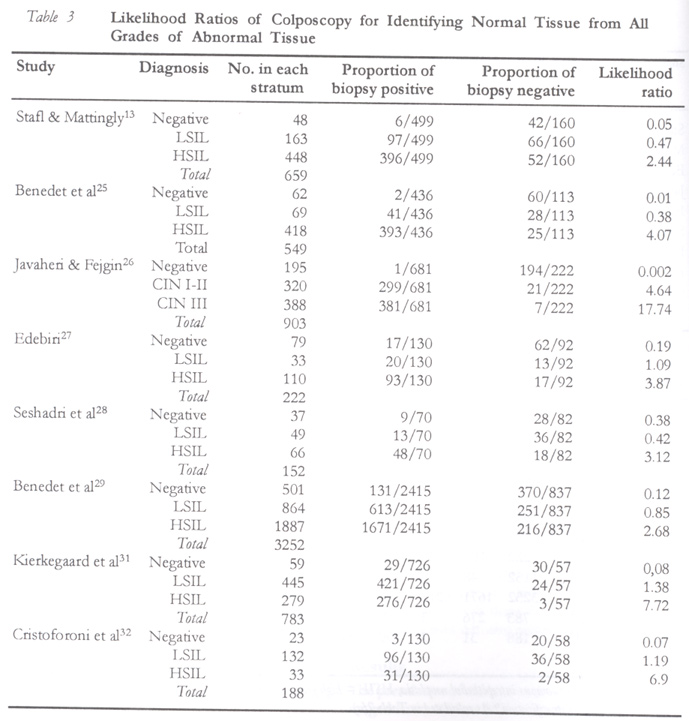
The performance characteristics of colposcopy were calculated using two threshold values (cut off points). First, the ability to differentiate a normal cervix from an abnormal one was examined. Next, a different cut off was chosen to examine the same characteristics for colposcopic ability to recognise a high grade abnormality versus other grades, i.e., regarding only high grade abnormality `disease present' and other grades as `disease absent'. This shift in threshold value was done to examine colposcopic performance over different ranges of abnormality. RESULTS The prevalence of disease in the study populations ranged from 40% to 89%. Meta-analysis of all the studies revealed that the correlation between the colposcopic impression and the directed biopsy diagnosis (colposcopic accuracy) was within one histologic degree in 89% of the cases, and was in exact agreement (concordance) with the histologic diagnosis in 61% of cases (Table 4). It is seen from this table that the tendency at colposcopy to diagnose a lesion as more severe is the same as the tendency to diagnose a lesion as less severe. This tendency, however, is considered quite low at 5%. The sensitivity of colposcopy in differentiating normal from abnormal cervical tissue ranged from 87% to 99% and the specificity ranged from 26% to 87% (Table 2a). The positive predictive value ranged from 53% to 96%, and the negative predictive value from 51% to 99%. By choosing a different cut-off point where only high grade lesions are regarded as abnormal, a fall in sensitivity is observed with a concomitant large increase in specificity. This is depicted in Table 2b. This shift in threshold value also reflected in appreciable increases in the positive predictive values. These results suggest that colposcopy is more efficient in distinguishing high grade from low grade lesions than in distinguishing low grade from normal cervical tissue. The likelihood ratios of obtaining a particular result for a given disease state are presented in Table 3 and a definite trend is preserved throughout all the studies. There is a consistent increase in the values in moving from one stratum to another. The difference is much larger from LSIL to HSIL strata than from normal to LSIL. This is further evidence that colposcopy is more efficient in diagnosing high grade lesions, with the implication that there is a more appreciable difference when distinguishing HSIL from less serious diagnosis than when distinguishing LSIL from normal cervical findings. DISCUSSION Cervical cancer is a serious disease but it is probably the most preventable of all female genital cancers. It is a disease for which screening is suitable and early treatment is beneficial. In the past, cold knife conisation biopsy was the traditional method employed to provide definitive histological diagnosis in patients with abnormal cervical smears. A cone biopsy though accurate and useful carries with it complications that cannot be ignored. It requires hospitalisation and the patient's reproductive capability is often jeopardised. In contrast, colposcopy offers numerous advantages — costly in-patient conisation is avoided and there are no significant complications. The accuracy of colposcopy in the clinical diagnosis of cervical neoplasia in patients with abnormal cytology has been variously documented by several investigators in various clinical settings, in different cohorts of patients and using different outcome measures.36-40 This review illustrates the validity of colposcopy as it is used in the everyday clinical setting. It has tried to eliminate possible sources of bias due to patient selection, intervention methodology and outcome measure bias as much as possible while trying to aggregate a homogenous collection of patients suitable for such analysis. However, language and publication bias proved difficult obstacles to surmount in the circumstances. The validity of colposcopy as an integral part of the management of early cervical neoplasia is confirmed by this review. Test Performance The validity of colposcopy to diagnose early cervical neolplasia is attested to by the very high level of accuracy of this review. A high sensitivity was observed at the expense of the specificity but identifying lesions as cancer is more important than avoiding overcalling of lesions. However, when the threshold of diagnosis was raised, a marked improvement in specificity was observed. The implication of this is that colposcopy performs better in the identification of higher grades of intraepithelial neoplasia than it does in the recognition of low grade lesions. This fact is also attested to by the observed likelihood ratios (Table 3), which show a consistent pattern among all the studies. There was clear demarcation among diagnoses with small but consistent and important shifts occurring between normal cervix, low grade and high grade SIL. This information supports that presented for the distribution of proportional sensitivities and specificities, indicating that clinically there is a larger appreciable difference when distinguishing high grade SIL and cancer from less serious diagnoses than when distinguishing low grade SIL from normal cervix and inflammation. This difference supports the validity of the Bethesda classification.43 The predictive value of colposcopy was also shown to be greater with increasing grades of neoplasia. The results suggest that colposcopic accuracy is quite high (89%), with agreement in 61% of cases. However, there was an equal proportion of false positives as there were false negatives, although false positive results were more likely with low grade lesions (Table 3). A false value of about 5% was generated on either side accuracy. Several reasons have been adduced for the false positive rate of colposcopy. There are some benign lesions of the cervix such as papillomatous lesions in which colposcopic differentiation from a malignant lesion is extremely difficult or sometimes impossible, where a directed biopsy is necessary to establish the correct diagnosis.44 Confusion between mild dysplasia, cervicitis and HPV infection may account for the inaccuracy of the diagnosis of low grade dysplasia by colposcopy. There is also the potential for measurement error by colposcopists because of their knowledge of previous Pap smear result.30 Occasionally, colposcopic lesions may be present without significant changes in tissue histology.44 There are pitfalls that may lead to a false negative colposcopic impression. Underestimation may occur when a high grade lesion may be overlooked because it is placed within a larger area of prominent aceto-white epithelium typical of low grade disease.45 Lesion size has also been correlated with the severity of subsequent pathologic result by others46,47 and it has been suggested that lesion size may result in less accurate biopsies unless one samples the entire large lesion.46-48 Colposcopists may not be entirely responsible for the disagreement between the colposcopic impression and the histologic diagnosis as a certain degree of interobserver variability occurs between pathologists when histologically grading cervical intraepitheleial neoplasia. The apparent colposcopic overestimation of low grade disease may be an excessive representation based on a falsely negative histologic standard.49,50 Implications for Practice The studies included in this analysis involved clinicians who were experienced in the technique of colposcopy. Colposcopy is a visual technique that requires extensive training and experience. The limiting factor in the use of this diagnostic tool is the clinical skill and experience of the operator. As is true with the use of any scientific instrument, the accuracy of the method is directly related to the expertise of its operator. In this regard, to ensure that colposcopy continues to yield a satisfactory level of accuracy, proper training and certification of colposcopists is recommended with appropriate quality control programmes. An appropriate volume of patients must be seen yearly in order to maintain these skills41, therefore, it may be necessary to centralise services within geographical areas to ensure that the highest possible level of care is rendered to patients requiring colposcopic assessment. The false negative rate of colposcopy is of particular concern as under-diagnosis is as important as over-diagnosis. Endocervical curettage has been considered by a number of observers and its use varies from none13,51, to use only when it would contribute to management52,53, and use in all patients54,55. Some workers believe the results are always positive in patients with invasion.54-56 Articles reviewing cases in which patients develop invasive disease after colposcopy56,57 have led to the observation that endocervical curettage was often omitted in those with later invasion, but these articles also reveal that endocervical curettage was done and the result was negative in a substantial number of the patients with later invasive disease. Randomised controlled trials are needed to provide evidence of best practice. Implications for Research A number of new clinical management strategies and technologies are being proposed and tested to address the need to improve screening and detection of squamous intraepithelial neoplasia and cervical cancer. These include HPV testing, cervicography, speculoscopy, the polar probe, and fluorescence spectroscopy. Some of these have been proposed to supplement colposcopy as a diagnostic tool while others have been proposed to replace colposcopy. Arguments have been largely centred around cost effectiveness. These reasons are quite valid but to determine their optimal clinical role, these strategies must be shown to have a performance better or at least at par with the current standard of colposcopy. Efforts must continue to strive to provide the best colposcopy can offer. The possibility of distance learning through `telecolposcopy' appears feasible in this age of digital imaging and computers where images (colpophotographs) may be transferred via the internet in a two-way collaboration between areas of low technical expertise and remote experienced review centres. Such facility has been reported with promising results.23,58 This technique is of particular importance as it may offer opportunities for capacity building in less developed regions of the world with little technical expertise. It may be used for on site training, continuing evaluation, certification and ongoing collaborative support. The technique is particularly attractive because it removes the need for practice eligibility registrations in intended host institutes, visa restrictions, and travel as well as living expenses. The inter-observer variability, which is dependent on skill and expertise of the operator, is a potential limitation of colposcopy. The use of computerised image analysis of the colposcopic appearance is a method worthy of exploring through research in order to deal with this limitation.32 If colposcopy is to have a role in the diagnosis of pre-clinical carcinoma, it is of paramount importance to show that invasive carcinoma is not missed. Anyone using colposcopy must be satisfied that this fundamental criterion is met. The final conclusion is that colposcopy is an indispensable tool in the evaluation of a patient with an abnormal cytology. Colposcopically directed biopsy provides a histopathological diagnosis and colposcopic impression provides information concerning the lesion size and location, which form the basis of additional management. Overview of literature revealed that colposcopy is a diagnostic technique with qualities within acceptable clinical standards. SUMMARY A review of literature revealed that colposcopy is very accurate in the diagnosis of early cervical neoplasia and it has a high sensitivity for detection of lesions. The positive predictive rate is better, as the cervical lesion is more severe. The limitation of colposcopy is its dependence on observer variability and relatively weaker performance in differentiating normal cervix from low grade lesions. Innovations to improve its performance in this regard are needed. Recently, computer assisted analysis of the colposcopic image is being evaluated. It is concluded that colposcopy is an indispensable tool in the management of premalignant cervical disease as long as the limitations of the technique are kept in mind by the operator. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02036t4.jpg] [rh02036t3.jpg] [rh02036t1.jpg] [rh02036t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}