 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 70-81 Gender Differences in Cues that Affect Condom Use among Adolescents in Lomé, Togo Ilene S Speizer 1, Stephanie A Mullen2, Emilien K Vignikin3 and Kodjovi Kouwonou3 1Virginia Commonwealth
University. 2John Snow, Inc. 3Université de
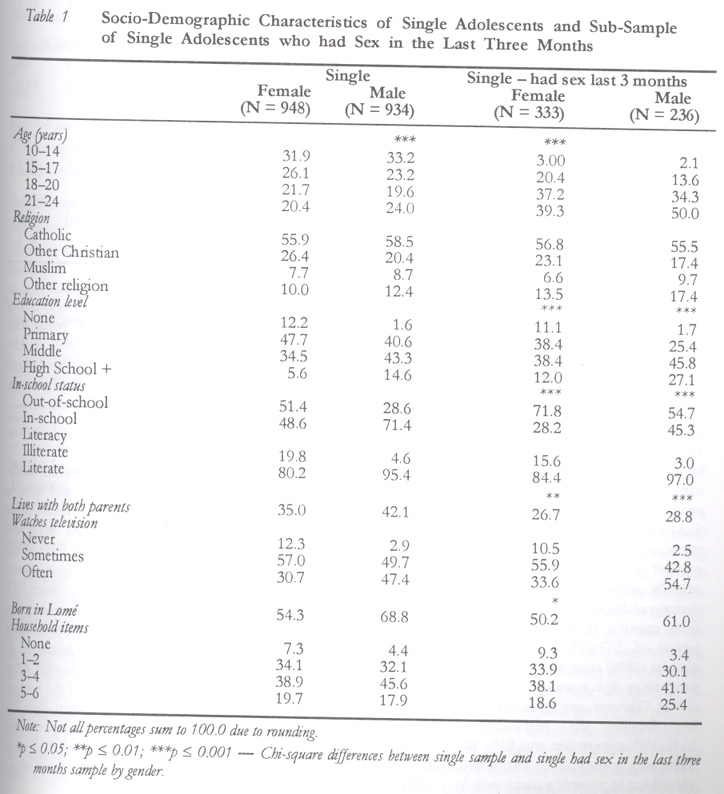
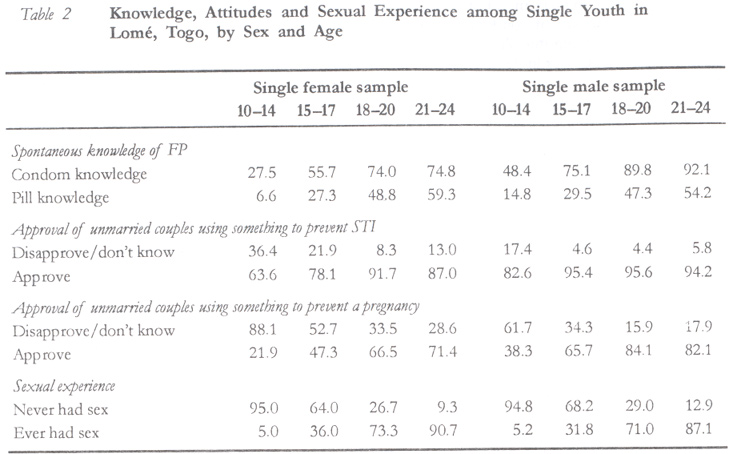
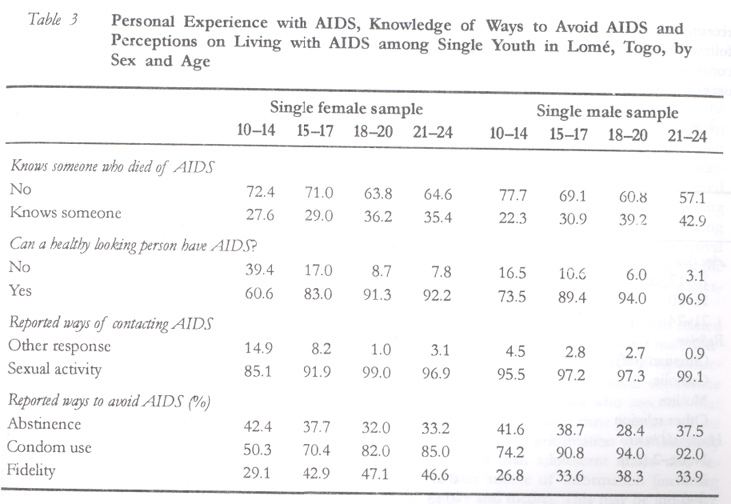
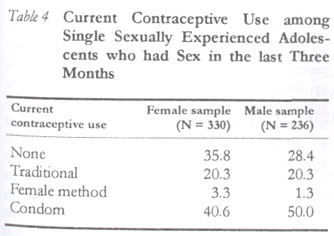
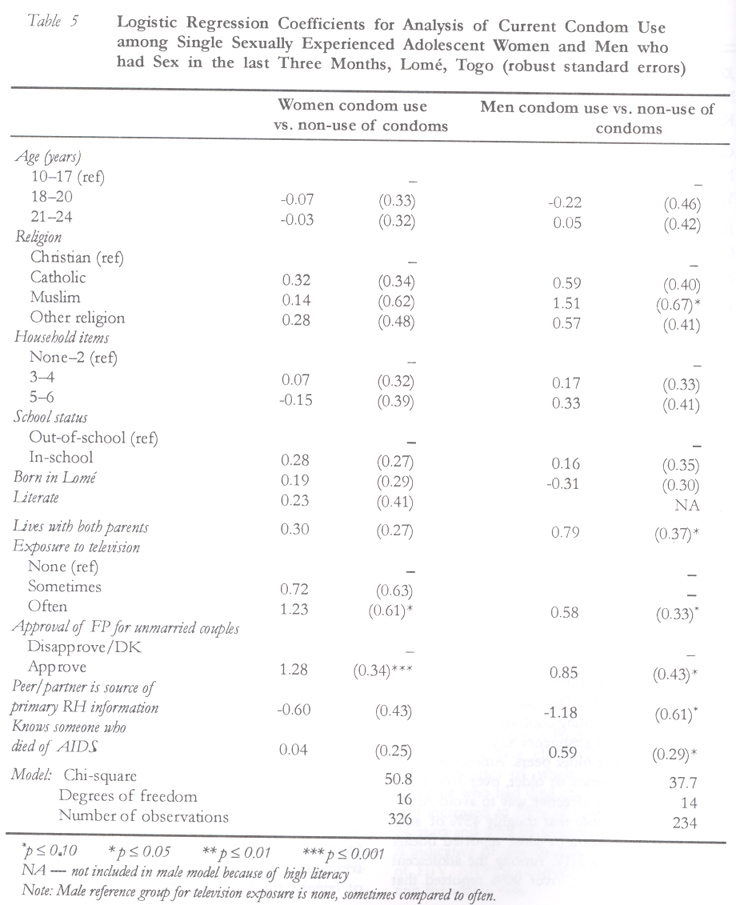
Bénin, Unité de Recherche Démographique (URD). Code Number: rh02037 ABSTRACT A population-based sample study of adolescent women and men from Lomé, Togo, was conducted to examine their responses to personal experiences with AIDS. Information was obtained on youth reproductive health knowledge, attitudes and practices, including attitudes towards HIV/AIDS and personal experience with AIDS. Multivariate results demonstrate that an important factor that distinguishes adolescent male condom users from non-users of condoms is the knowledge of someone who died of AIDS. Conversely, personal experience with AIDS was unrelated to reported condom use among adolescent women. The results illustrate that reproductive health programmes directed towards adolescents need to target men with messages different from women. Sexually active men respond to personal experience with AIDS by adopting condoms whereas women may have less control over condom use and have other strategies such as abstinence and fidelity to protect themselves from AIDS and unintended pregnancies. (Afr J Reprod Health 2002; 6[3]: 70–81) RÉSUMÉ Les différences fondées sur les sexes dans les signals qui affectent l'utilisation des préservatifs chez les adolescents à Lomé, Togo. Nous avons mené une étude échantillonnée des femmes et des hommes à Lomé. Cette étude, basée sur la population, avait pour but d'examiner leurs réponses à des expériences personnelles par rapport au SIDA. Nous avons recuelli des renseignements sur la connaissance de la santé reproductive chez la jeunesse, ses attitudes et ses pratiques y compris ses attitudes envers le VIH/SIDA et ses expériences personnelles à l'égard du SIDA. Les résultats multifactoriels montrent qu'un facteur important qui distingue les usagers-hommes des préservatifs de non-usagers des préservatifs est le fait d'avoir connu quelqu'un qui est mort du SIDA. Inversement, l'expérience personnelle à l'égard du SIDA n'était pas liée à l'emploi des préservatifs chez les adolescentes. Les résultats montrent que les programmes de la santé reproductive qui sont dirigés vers les adolescents, doivent cibler les hommes avec des messages qui sont différents de ceux des femmes. Les hommes qui sont sexuellement actifs répondent à l'expérience personnelle vis-à-vis du SIDA en adoptant des préservatifs alors que les femmes auront peut-être moins d'autorité sur l'emploi des préservatifs et elles ont d'autres stratégies telles l'abstinence et la fidelité pour se protéger contre le SIDA et contre les grossesses non désirées. (Rev Afr Santé Reprod 2002; 6[3]: 70–81) KEY WORDS: Gender differences, condom use, adolescents, Togo INTRODUCTION In sub-Saharan Africa, increasing attention is being paid to the young adult population aged 10–24 years. Interest in this group stems from the large proportion of young adults in Africa and the changing health and social needs of the group that come about as a consequence of urbanisation and modernisation.1 With the rising importance of education, the time between the onset of puberty and marriage is becoming longer, resulting in a higher likelihood that young people will engage in premarital sexual activity, which may or may not be socially sanctioned.2 Adolescents who are sexually active at an early age are at risk of an unintended pregnancy and sexually transmitted infections (STIs). The risk of these outcomes is higher for adolescents than adults because adolescents often fail to use contraception consistently and effectively.3 Furthermore, adolescents change sexual partners often, resulting in increased risk of exposure to sexually transmitted infections including HIV.4 Unprotected premarital sex among adolescents is a social problem for sub-Saharan African societies. Single adolescent women who become pregnant are often forced to drop out of school, reducing their future earning and work potential.1 Those women who do not want to drop out of school or who do not want to have an unintended birth may resort to illegal, unsafe abortions, increasing their risk of disease or death.3,5-7 Furthermore, adolescents who become sterile as a consequence of a STI are likely to have less opportunities for marriage and future family development. Finally, exposure to HIV infection ultimately means death, given that treatment is generally unavailable in sub-Saharan Africa. To protect all adolescents from the social, financial and health consequences of early sexual activity, it is necessary to promote protective sexual behaviours. Studies of adolescents need to consider what motivates some of them to engage in early or unprotected sex and others to abstain or to use contraception, especially condoms, when sexually active.8 Previous research on risk-taking behaviours emphasises a number of psychological and behavioural factors that are associated with behaviour change.9 For example, according to the Health Belief Model, adoption of preventive behaviours is influenced by (1) perceived barriers to performing the behaviour; (2) perceived benefits of performing the behaviour; (3) perceived susceptibility to the outcome; (4) perceived severity of the outcome; and (5) cues to action.10 Applications of these types of models to adolescent reproductive health outcomes have been predominantly undertaken in the US11,12, with recent applications in the developing world (e.g., Ghana13). The present study examines a specific component of the Health Belief Model, cues to action. Cues to action are thought to be necessary to stimulate decision-making processes that lead to adoption of protective behaviours.10 They are thought to act indirectly on behaviours through perceived threats of the outcome.10,12 Previous studies on behaviour change as a response to AIDS risk demonstrate that persons who have personal experience with the AIDS epidemic are more likely to report behaviour change than persons who have no personal experience.9,14,15 In their three-country study, Macintyre, Brown and Sosler14 found that knowing someone with AIDS was a significant determinant of behaviour change among adult men in Uganda and Zambia, and approached significance in the same direction in Kenya. Given the high levels of HIV/AIDS in parts of Africa, this cue to action may become the most important factor that affects adoption of protective behaviours. Likewise, a recent study in Ghana among adolescent males found that an important predictor of consistent condom use is the knowledge of someone who died of AIDS.16 No studies were found that examined the impact of knowing someone with AIDS on condom use among adolescent (or adult) women. Studies of adolescents demonstrate the importance of AIDS knowledge and attitudes on reproductive health outcomes, but these studies do not assess the role of personal experience with HIV/AIDS. For example, previous research has shown that adolescents with appropriate knowledge of pregnancy and STIs/HIV risks and methods to prevent these risks are not necessarily using contraception due to other mediating factors including partner unwillingness to use, poor access to contraceptives, discomfort with service providers and facilities, and negative attitudes towards contraceptive use among peers, family or community.8,17,18 Motivations to use condoms for STIs/HIV and pregnancy prevention also result in barriers to consistent and effective condom use. For example, qualitative research among adolescents in Edéa, Cameroon demonstrates that adolescent males and females use condoms for different reasons.19 Adolescent females use condoms to prevent pregnancies and adolescent males use condoms to prevent sexually transmitted infections, including HIV.19 These perspectives of condom use may be important to the role that personal experience with AIDS plays on adolescent adoption of protective behaviours (i.e., condom use). Given the multitude of factors that influence adolescent behaviours, it is crucial to study cues to action that may affect adolescent motivation to avoid unintended pregnancies and sexually transmitted infections. In this paper, we examine whether adolescents who know someone who died of AIDS are more likely to use condoms than adolescents with no personal experience with AIDS. We assess whether this cue to action has the same effect among male and female adolescents in Lomé, Togo. THE STUDY SITE Togo is a small West African country of about 4.5 million inhabitants bordered by Ghana to the west, Republic of Benin to the east, and Burkina Faso to the north. The country runs about 40 miles from east to west (widest point is 90 miles) and 400 miles from north to south. Togo has a varied geography with a small coastline, a plateau region and a savanna region. This results in two types of climate in Togo — (1) an equatorial climate with two rainy seasons and two dry seasons; and (2) a tropical climate with one rainy season and one long dry season. In Togo, there are over 40 ethnic groups, each having its own language and cultural practices. The official language is French with two official local languages — Kabaye in the north and Ewé in the south. Roughly half of the population of Togo is below 15 years. The 1998 Togo Demographic and Health Survey demonstrates that roughly 20% of adolescents aged 15–19 years have already had at least one child or have ever been pregnant.20 Moreover, more than half of women in Togo aged 20–49 years reported that they had their first sexual experience before the age of 18. Only 8% of 15–19-year-old women who were sexually active in Togo reported modern method use (7% reported condom use and 1% reported other modern method use). Fourteen per cent of 15–19-year-olds reported natural method use, specifically the calendar method.20 Therefore, sexually active young people in Togo are at risk of unintended pregnancies and sexually transmitted diseases. For example, in Togo it has been found that the incidence of HIV/AIDS among the urban population aged 15–49 years has been rising, with adolescents (15–24 years) making up more than 20% of the AIDS patients between 1987 and 1997.21 The site for this study is Lomé, the capital of Togo. Lomé is located on the coast of Togo and is the centre of commercial and international activities. The population of Lomé is about one million. Lomé, like the rest of Togo, has a heterogeneous population with many ethnic groups and languages; the majority of the Lomé population comes from the south (Adja-Ewé). MATERIALS AND METHODS The data for this study were collected as baseline data for an evaluation of the Association Togolaise pour le Bien-Etre Familiale (ATBEF – International Planned Parenthood Federation affiliate) youth centre established in late spring of 1998. The baseline data were collected in November 1998. The study plan was designed based on the recent Togo Demographic and Health Survey (TDHS) that was undertaken between February and March 1998. For the TDHS, a random sample of 62 clusters from the total number of 866 clusters in Lomé was selected. The TDHS identified and listed all households in the 62 clusters and randomly selected households and individuals to interview. For this study, the households from the 62 clusters were revisited and re-listed. A random sample of adolescents was selected for interview from the new household listing with the goal of obtaining a representative sample of 2000 adolescents (1000 male and 1000 female). Adults (aged 30+) in a sample of the households were also interviewed to permit an evaluation of parental perspectives on adolescent reproductive health issues. This study includes only the data from the adolescent sample. Adolescents aged 10–24 years were interviewed by young interviewers using a semi-structured questionnaire. The questionnaire included 319 questions and was structured in five modules, namely, individual demographic characteristics, general sexual knowledge, sources of reproductive health information, sexual practices, and reproductive health needs and desires. A total of 2083 adolescents were interviewed for the study. Over 90% of the eligible sample of adolescent males and females were actually interviewed. A comparison of adolescents (15–24 years) in this sample with adolescents from Lomé in the 1998 Togo Demographic and Health Survey (TDHS) finds few differences between the two groups with the exception that the adolescent men in this sample are less likely to be currently in school than adolescent men in the TDHS. Therefore, the interviewed sample is representative of the adolescent population of Lomé.22 Given that the emphasis of this study is on premarital sexual activity and sexual risk-taking, we use the sample of single adolescents (N = 1882, dropped 201 married adolescents). For the analyses of current condom use, we use only the single, recently sexually experienced adolescents (had sex in the last three months) (N = 569). All analyses are stratified by sex. The emphasis of the multivariate analyses below was to determine whether personal experience with AIDS is associated with condom use. For the multivariate analyses we used only those adolescents who reported having had sex in the last three months. The reason for this select sample is a consequence of the structure of the question on contraceptive use that asked about `current contraceptive use.' Since adolescents tend to have infrequent sex, we preferred to emphasise those adolescents who had had sex recently to reduce the potential for recall problems that would enter when assessing contraceptive use over a longer period of time. Also, given our interest in assessing whether personal experience with AIDS is associated with current behaviours, we prefer to limit our analysis to condom use in the recent period, suggesting that simultaneous or prior experience with AIDS is related to recent behaviours. The outcome variable used for the analysis of condom use was coded zero for non-use of condoms and one for current condom use. In this sample, the majority of modern method use was condom use (92% of modern method users use condoms, 8% use female methods). Therefore, we emphasised condom use for the analyses of whether personal experience with AIDS was associated with reproductive health behaviours. In models that compared modern use (condom and female methods) with non-use of modern methods, we found comparable results because the overwhelming majority of modern use was condom use (results not shown). Moreover, analyses were performed comparing non-use, traditional method use and modern method use. The results using this trichotomous outcome were similar to the results presented for condom use (results not shown). We used logistic regression methods with robust standard errors to control for the clustered design of these data.23 All analyses were stratified by gender. The models of condom use include a number of demographic and reproductive health independent variables. Age (10–17 years, 18–20 years, 21–24 years) was included in the models to control for the fact that younger adolescents may be less knowledgeable about STIs/HIV risks and prevention than older adolescents. Because only a small number of the adolescents aged 10–14 years were sexually active, these young adolescents were grouped with the 15–17-year-olds. We also included religion in the model, given that some religions are more supportive of contraceptive use than others. Household socioeconomic measures in the model included number of household items (refrigerator, television, radio, car, motorcycle, or electricity) and living arrangement (lives with two parents versus lives with one or no parent). Adolescents from households that are better off financially (more household items or two parents) are likely to be better able to afford condoms or more motivated to avoid an STI or unintended pregnancy than adolescents who are of lower socioeconomic status. Also included in the models is whether or not the adolescent was currently in school. Given that among adolescent samples, level of education is often correlated with current age (that is younger adolescents are not old enough to have entered secondary or higher level of school), we chose to include in-school status as a measure of exposure to education and modern influences. For the adolescent female model, we also included a measure of literacy to capture differences in the level of education. For the adolescent male model, 95% of adolescent males were literate, therefore, this variable was dropped from the model. Adolescents in school (or literate) were hypothesised to be more likely to use condoms than adolescents who were out of school (or illiterate) due to their greater knowledge of STI risks and prevention. Other independent variables in the model of condom use included whether or not the adolescent was born in Lomé and exposure to television. Adolescents who were not born in Lomé were hypothesised to be more conservative (less urbanised) than adolescents who were born and raised in Lomé. Moreover, adolescents who watched television were hypothesised to have more modern influences and possibly more information on condoms through the media than adolescents who never watched television. Note that for the male models we grouped television watching as never or sometimes versus often, since only a small percentage of adolescent males never watched television. The remaining variables in the multivariate models were specific to reproductive health knowledge and attitudes. First, we included adolescent attitudes towards unmarried couples using family planning. Adolescents who did not approve family planning use by the unmarried were hypothesised to be less likely to be condom users when they had premarital sex than adolescents who approved. Also available was adolescent approval of unmarried method use to prevent a STI. Due to high approval of STI prevention, this variable was not included in the multivariate models. Primary source of reproductive health information was also included in the model of condom use. A number of sources were possible including family, school, media, peer or partner, and other. We found no differences in the effects for family, school, media and other as compared to peers or partner. The final model compares peers or partner to all other sources. Finally, the last variable of interest to this analysis is whether the adolescent knew someone who died of AIDS. We hypothesised that knowing someone who died of AIDS would serve as a cue to action, leading to greater condom use among those adolescents with personal experience compared to adolescents with no personal experience with AIDS. RESULTS Characteristics of the Sample Table 1 presents the characteristics of single adolescent women and men in the Lomé study population. Columns 1 and 2 present the characteristics for the single sample and columns 3 and 4 present the characteristics for the single, recently sexually active sample. Chi-square tests of differences between the single sample and the single recently sexually active sample by gender are presented in the table. In the Lomé sample of single adolescents, the mean age was 16.8 years. The most common religion is Catholicism, followed by other Christian religions. The sample of single men all had some education with equal proportions having primary and middle school education and 14.6% with high school or greater level of education. Among the women, 12.2% had no education and 47.7% had primary level education, indicating that single adolescent females in Lomé were less educated than their male counterparts. The educational differences between males and females were also apparent in the proportion of the sample currently in school and able to read. A larger percentage of adolescent males were currently in school and literate than adolescent females. Adolescents appeared to have some access to material possessions within their households. The most common household item the adolescents reported having was a radio (91%), followed by electricity (65%) and television (61%). Likewise, the majority of the adolescents watched television sometimes or often, a reflection of easy access to television in the household or neighborhood. Finally, roughly half of the female adolescents were born in Lomé, compared to more than two thirds of adolescent males. This difference may be a consequence of young women coming to Lomé for domestic work, commercial activities, or marriage. The characteristics of the single recently sexually active adolescent women and men are presented in columns 3 and 4 of Table 1. Chi-square tests of differences between the single sample and the single recently sexually active sample show that the single adolescents who had had recent sex were older, more educated (correlated with older age), less likely to be currently in school, and less likely to be living with both parents. Furthermore, among adolescent males, those who had had recent sex were less likely to be born in Lomé. The analyses of the determinants of condom use presented below were only among this older, more educated single sample that had sex in the last three months. Knowledge, Attitudes and Sexual Experience Table 2 presents the knowledge, attitudes and sexual practices among single adolescents in Lomé by gender and age. Table 2 illustrates that the majority of adolescents 15 years or older were knowledgeable about condoms. This is an important first step to getting adolescents to use this method for pregnancy and STI/HIV prevention. Spontaneous knowledge of pills was lower at all ages, indicating that the method controlled by adolescent women to prevent unintended pregnancies is less likely to be adopted in this population. Table 2 also presents single women and men's attitudes towards unmarried couples using a method to avoid an STI and attitudes towards unmarried couples using family planning to prevent a pregnancy. Approval of both types of method use rises with age and is higher at all ages among males as compared to females. Moreover, among males and females approval of STIs/HIV prevention is higher at all ages as compared to approval of pregnancy prevention. High approval of methods to prevent STIs/HIV is important for condom use in this population. In the comparison of approval of methods to prevent STIs/HIV and methods to prevent a pregnancy among the single recently sexually active sample, we saw a similar trend. Among males who were sexually active in the last three months, there was significantly greater approval of STIs/HIV prevention for unmarried couples (98%) compared to approval of pregnancy prevention for unmarried couples (87%, p < 0.001). Likewise, among single recently sexually active females the percentage approving of STIs/HIV prevention was 91% compared to only 71% who approved of unmarried couples using something to prevent a pregnancy (p < 0.001). Finally, Table 2 demonstrates that only 5% of the youngest adolescents (under 15 years) have ever had sex, and the proportion rose to 33% among 15–17-year-olds. Among single women and men over age 18, the majority were sexually experienced. AIDS Knowledge and Attitudes Table 3 provides perspectives on adolescent familiarity with the HIV/AIDS epidemic and ways to avoid HIV/AIDS. Among single youth from Lomé, there was high familiarity with AIDS and ways of contacting HIV/AIDS. Over 98% of the youth were familiar with HIV/AIDS (not shown), and over 90% knew that one can contact HIV from sexual activity. Likewise, the overwhelming majority of the sample knew that a healthy looking person could have HIV/AIDS. Furthermore, almost a quarter of single 10–14-year-olds knew someone who had died of AIDS and the proportion increased to 35% of single women aged 21–24 years and 43% of their male counterparts. This is indicative of personal experience with the risk of HIV/AIDS, a potentially important cue to action for adolescents. Also presented in Table 3 are reported ways to avoid contacting HIV. This table demonstrates a general pattern that young adolescent women were more likely to report abstinence as a way of avoiding AIDS than their older peers. Among the adolescent women 15 years or older, over 70% knew that condoms are an effective way to avoid AIDS. It is interesting to note that roughly 45% of adolescent women 15 years or older reported fidelity as a way of avoiding HIV. Among the adolescent men 15 years or older, over 90% reported that condom use is an effective way to avoid HIV but only a third reported that fidelity is an effective strategy. Women may have more control over their number of sexual partners (fidelity) than whether a condom is used, which results in the above pattern of responses for ways to prevent HIV/AIDS. The Role of Personal Experience with AIDS on Condom Use The emphasis of the following discussion is on the single recently sexually active (within the last three months) adolescents (N = 566). An understanding of factors associated with condom use in this group is useful for designing programmes that promote responsible reproductive health behaviours among all youth. It is important to note that we are talking about the group of adolescents who are older, more educated and less likely to be currently in school compared to all single adolescents (as seen in Table 1). Among this group, the majority were using some form of contraception (64% of females and 72% of males) (see Table 4). The most common method used was condom; used by 41% of females and 50% of males who were single and recently sexually experienced. For the analyses that follow, we assessed current condom use versus condom non-use (non-users, traditional method users and female method users) to assess whether personal experience with AIDS is associated with greater self-protection from HIV among women and men in Lomé. In Table 5 logistic regression coefficients for the analyses of the determinants of condom use are presented for single and recently sexually active females and males. The models include demographic factors, attitudes towards unmarried couples using contraception to prevent a pregnancy, sources of reproductive health information and personal experience with AIDS. In a joint male and female model, no differences were found between single female and single male adolescents on condom use, controlling for the other demographic and attitudinal variables (results not shown). Column 1 of Table 5 presents the results of the logistic regression for single adolescent women who were recently sexually active. The only factors found to differentiate women who used condoms from women who did not use condoms are exposure to television and approval. Single sexually active women who watched television often were more likely to use condoms than single sexually active women who never watched television. Moreover, single women who approved of unmarried couples using a method to prevent pregnancy were more likely to use condoms than single women who disapproved of pregnancy prevention. It is notable that in a separate model where we included approval of unmarried couples using a method to prevent STIs/HIV instead of approval of pregnancy prevention, no differences were found on condom use by approval of STIs/HIV prevention (results not shown). This may be a consequence of high approval of STIs/HIV prevention among women (91%), or may be indicative of women using condoms as a method to prevent pregnancy rather than as a method to prevent STIs/HIV. Finally, in the female model, personal experience with AIDS did not have a significant impact on condom use; personal experience was not an important cue to action among adolescent women. The results of the male model demonstrate that single recently sexually active adolescent males who were Muslims were more likely to use condoms than their Christian peers. This may be explained by the fact that HIV/AIDS education campaigns have emphasised that in the Koran, it is pertinent to protect yourself from disease, and Muslim males were using condoms with disease prevention in mind. We also found that adolescent males who lived with two parents were more likely to use condoms than adolescent males who lived with one or neither parent. Living with two parents may be a proxy for motivation to prevent a birth or for socioeconomic status in that adolescent males who lived with two parents were more likely to be able to afford condoms. Similar to adolescent women, adolescent men who watched television often were more likely to use condoms than adolescent males who never or sometimes watched television. Approval of unmarried family planning use was associated with greater condom use among adolescent males as well. We did not test approval of methods to prevent STIs in the male sample since 98% of single recently sexually active adolescent males approved. The remaining two reproductive health related factors found to differentiate adolescent male condom users from non-users are source of reproductive health information and personal experience with AIDS. Adolescent males who reported that their peers or partners were their primary source of reproductive health information were less likely to use condoms than adolescent males who reported another source of information (including school, family and media). This may be indicative of peers or partners giving inappropriate information on reproductive health risks and prevention, or negative social norms towards condom use among males in Lomé. Finally, we found that adolescent males who had personal experience with AIDS (knew someone who died of AIDS) were more likely to report condom use than adolescent males with no personal experience with AIDS. Personal experience with AIDS is an important cue to action among adolescent males. DISCUSSION The results of this study demonstrate the role of HIV/AIDS in bringing adolescent men into discussions about contraceptive use in Africa. Prior to the AIDS epidemic, most family planning programmes emphasised women, particularly married women. As research increasingly demonstrated rises in premarital sex and adolescent unintended pregnancies24, family planning programmes began to include adolescent women into their target populations. These programmes often continued to ignore adolescent men. By ignoring the adolescent males, these programmes may have limited influence since condom use, the main method used by adolescents in Africa, is controlled by men. Prior to the rise in HIV/AIDS cases, interest in condom use in sub-Saharan Africa was low or non-existent.25 Condoms were generally used with prostitutes if at all. With increasing attention on HIV/AIDS, condoms have taken on a new level of importance. For example, a recent qualitative study among adolescents in Edéa, Cameroon, demonstrates that condoms are used with casual partners or partners that cannot be trusted rather than with frequent or trusted partners.19 Moreover, Calvès finds that adolescent women reported using condoms to avoid unintended pregnancies whereas adolescent men reported using condoms to prevent STIs/HIV.19 By increasing the focus of reproductive health programmes from simply reducing unintended pregnancies to reducing negative reproductive outcomes (unintended pregnancies and sexually transmitted infections), programmes may have better success getting the attention of adolescent men (all men) who ultimately control whether condoms are used. The findings from this study illustrate a number of points that are crucial for improving adolescent reproductive health programmes. For example, this study demonstrates high approval of method use to prevent STIs but lower approval for pregnancy prevention among unmarried adolescents. This suggests that programmes targeting adolescents may have more success if they link STIs/HIV and pregnancy prevention rather than discussing these two issues separately. Moreover, while condoms are reported as the most common method used in this Lomé sample, there still remain roughly 35% of single sexually active women and 28% of single sexually active men who are non-users of any method and thus at risk of both an unintended pregnancy and a sexually transmitted infection. Furthermore, this study demonstrates the importance of personal experience with AIDS on condom use among adolescent males. Roughly a quarter to one third of the single adolescent women and men had personal experience with AIDS. Thus, in Lomé, exposure to AIDS is common. One caveat is that the personal experience measured in this study might be abstract to some adolescents (i.e., know a television personality with AIDS) and more real to other adolescents (i.e., a friend or relative with AIDS). We are unable to distinguish the closeness of this personal experience in the study. Given this caveat, we found that controlling for age, in-school status and other demographic variables, single recently sexually active adolescent males who knew someone who died of AIDS were more likely to use condoms compared to their counterparts who had no personal experience with AIDS. Personal experience with AIDS is an important cue to action among adolescent males. It is notable that this cue to action was not important among adolescent women, possibly related to low condom use self-efficacy among adolescent women. This reason for the lack of effect among adolescent women remains to be explored using further qualitative and quantitative research methods. This study indicates the importance of integrating family planning programmes and STIs/HIV programmes especially for adolescent populations in sub-Saharan Africa. Given the high knowledge and awareness of STIs/HIV, adolescent men are increasingly seeking approaches to reduce their risk of these negative reproductive health outcomes. Programmes that simply promote `family planning' will be unable to capture the attention and participation of adolescent men. Conversely, adolescent women may have more control over the use of a female method (pill or injection) than the use of a condom and, therefore, programmes that simply promote condom use (for dual protection or for STIs/HIV prevention) may be leaving women at risk of an unintended pregnancy if they are unable to insist on condom use. Reproductive health programmes for youth in sub-Saharan Africa need to address adolescents' STIs/HIV and pregnancy prevention situations and needs simultaneously to reduce the overall level of unintended pregnancies and sexually transmitted infections among Africa's future generation of workers and parents. ACKNOWLEDGMENTS This project was supported by the United States Agency for International Development subcontract number P-6002-Tulane-01, Modification 06, Cooperative Agreement #CCP-A-00-96-90002-00. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02037t4.jpg] [rh02037t3.jpg] [rh02037t2.jpg] [rh02037t1.jpg] [rh02037t5.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}