 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 82-92 Reproductive, Sexual and Contraceptive Behaviour of Adolescents in Niger State, Nigeria Adegbenga M Sunmola1, Morenike Dipeolu2, Sunday Babalola2 and Adebayo D Otu1 1Department of Psychology,
University of Ibadan, Ibadan, Nigeria. 2Department of Animal Production
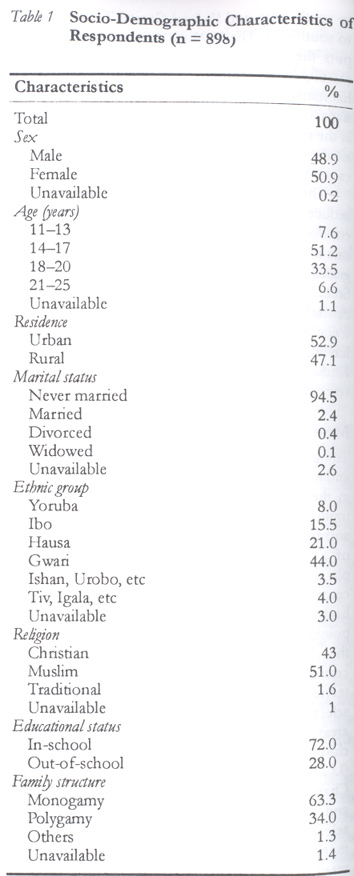
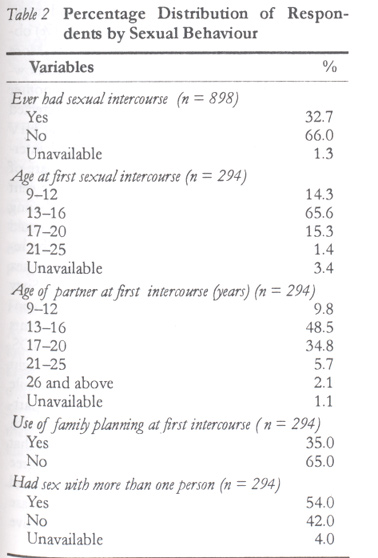
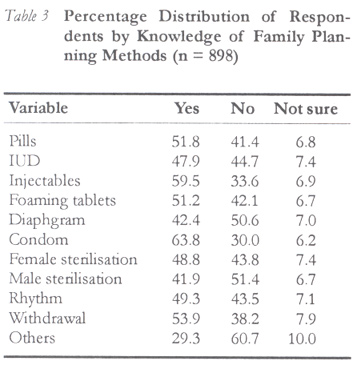
and Health, University of Agriculture, Abeokuta, Nigeria. Code Number: rh02038 ABSTRACT This is a multi-stage random sampling study involving 896 male and female adolescents aged 11–25 years in Niger State of Nigeria. Thirty three per cent of them had already had first sexual experience. Only 3.6% were married. Most of the Gwari and Hausa respondents acknowledged that they married at an earlier age than the Yoruba respondents. One half of those who were sexually experienced had more than one sexual partner. Majority of the respondents were informed about HIV/AIDS and STDs. More Gwari and Hausa respondents felt that HIV infection could be prevented by not having multiple sexual partners than Yoruba and Igbo respondents. A wide disparity between contraceptive knowledge and use was found. Knowledge rate was between 41.9% and 63.8%, while use rate was between 0.7% and 12.5% for the contraceptive methods studied. Condom knowledge and use rate was highest. For prevention of HIV/AIDS, more males than females thought condom was useful. Most Gwari and Hausa respondents did not use any FP method during their first sexual relationships. It is imperative for reproductive health programmes to intensify efforts in improving adolescents' attitude towards sexual risk and motivate them to exhibit behaviours that limit it. (Afr J Reprod Health 2002; 6[3]: 82–92) RÉSUMÉ Le comportement reproductif, sexuel et contraceptif chez les adolescents dans l'Etat de Niger, Nigéria. Il s'agit d'une étude à étape multiple, basée sur un échantillon au hazard, à laquelle ont participé 896 adolescents hommes et femmes âgés de 11–25 ans dans l'Etat de Niger au Nigéria. Parmi eux, 33% avaient déjà eu une première expérience sexuelle. Seuls 3,6% étaient mariés. La plupart des répondants gwari et haoussa ont bien reconnu qu'il s'étaient mariés à un plus jeune âge que les répondants Yoruba. Une moitié de ceux qui étaient sexuellement expériences avaient plus d'un partenaire sexuel. La plupart des répondants s'étaient renseignés sur le VIH/SIDA et sur les MSTs. Il y avait plus de répondants gwari et haoussa qui avaient le sentiment qu'on pouvait éviter l'infection VIH si l'on n'a pas de partenaires sexuels multiples que les répondants igbo et Yoruba. Nous avons remarqué qu'il y avait une grande disparité entre la connaissance du contraceptif et son usage. Le taux de connaissance était entre 41,9% et 63,8% alors que le taux d'emploi était entre 0,7% et 12,5% en ce qui concerne les méthodes contraceptives étudiées. La connaissance des préservatifs et le taux d'emploi étaient les plus élevés. En ce qui concerne la prévention du VIH/SIDA, plus des hommes que des femmes ont cru que le préservatif était utile. La majorité des répondants gwari et haoussa n'employaient pas les méthodes de PF pendant leurs premiers rapports sexuels. Il est obligatoire que les programmes de la santé reproductive intensifient leurs efforts pour l'amélioration de l'attitude des adolescents envers le risque sexuel et pour les motiver à afficher les comportements qui le limitent. (Rev Afr Santé Reprod 2002; 6[3]: 82–92) KEY WORDS: Adolescents, reproductive health, contraception, sexual behaviour, Nigeria INTRODUCTION The transtion from childhood to adolescence is characterised by an increase in personal control, responsibility and independence.1 Adolescents frequently negotiate and adjust to increased demands of a more autonomous lifestyle. In this context, responses to societal sexual norms and expectations can be seen as one of the key tasks of adolescence. Traditional norms in most Nigerian cultures demand premarital sexual abstinence until entry into marital unions. Nevertheless the norms have almost disappeared in all ethnic groups.2 A survey among the Ekiti shows that older women are more likely to be virgins till the time of marriage than younger women.3 The issue of sexual behaviour among adolescents is fast emerging as a public health concern in the country. It is necessary to put into perspective the sexual behaviour of adolescents since it is central to the prevention of transmission of human immunodeficiency virus (HIV) and other sexually transmitted infections (STIs) in the country.a Nine out of every ten male and female out of school adolescents are sexually active.4 A study in Lagos State reported that 40% of secondary school students had already had sexual intercourse.5 Most adolescents have their first sexual intercourse between ages 10 and 16 years. The picture is similar in many urban and rural areas in the country. In Calabar, 54% of female and 52% of male adolescents had sex before age 15.4 Studies in rural and urban Enugu, Kaduna, Lagos, Onitsha and Zaria show that sexual activity among adolescents is high.7 The study further shows that a greater proportion of urban females compared to their male counterparts frequently engage in sexual relationships. In Benin City, 77% of adolscent schoolgirls are sexually active.4 In Ilorin, 62% of in-school adolescents are sexually active, of which 30% of females and 58% of males had sex by the age of 19 years.9 A slightly lower proportion of 55% of adolescents was reported to be sexually active in a survey among in-school adolescents in the southeastern parts of the country.10 a HIV infects adolescents and young adults in the country more than those in the older age groups. Several studies have reported multiple sexual partnerships among adolescents in various parts of the country. Thirty five per cent of female adolescents in Lagos and a higher proportion of males reported that they maintained more than one sexual partner in non-marital relations.11 Similarly in Benin, 35% of adolesent schoolgirls said they had multiple sexual partners8, while in Lagos 75% of sexually active adolescent students indicated that they had more than two partners.5 Among adolescent university students in Ibadan, 48% reported having many sexual partners.12 The 1999 Nigerian Demographic and Health Survey (NDHS)13 also depicts similar findings. The data show that about 57% of Nigerian females aged 15–19 years had had no sexual experience, while close to 16% of those aged 20–24 years had had no such experience. For males, 73% of those aged 15–19 years had had no sexual experience, while 36% of those aged 20–24 years had had no such experience. There are however demographic disparities in relation to sexual activity of respondents aged 15–19 years. About 25% of females were sexually active, while only 10% of males in the same age group were active sexually. More females (50%) and males (52%) in rural areas were active compared to females (44%) and males (47%) in urban areas. In addition, 67–71% of females in the northen parts and 38–44% in southern parts of the country were sexually active. Furthermore, females and males without education were more sexually active than their counterparts with either primary or secondary education. Of those in the 15–19 years age group, only 10.3% of females and 26% of males used the condom during their last intercourse. The brief emprical review in this paper suggests that most adolescents in the country are sexually experienced, with a tendency for multiple partners. Severe risks are however associated with their sexual practice. There are concomitant risks of pregnancy, coital related diseases such as STDs, and HIV infections. About one half of female unmarried adolescents in some parts of Nigeria claimed to have been pregnant.4 In Ilorin, 13% of adolescent male students reported that they had made a partner pregnant, and 69% claimed that the pregnancies were aborted. Of the females in the study, 9% reported that they had been pregnant. Of these, 75% said the pregnancies were aborted.9 Adolescents usually perceive their pregnancies as `unwanted', thus they terminate them through illicit abortion, which is injurious to their health. Those who do not abort their pregnancies become early mothers and often have to interrupt or discontinue their schooling.14 A recent study observed that most adolescents secure abortion from unqualified persons after a long delay, using high risk methods and only seek professional attention when complications occur.15 One of the dangers of the risky sexual behaviour among adolescents is the possibility of becoming HIV infected. A survey shows that 21% of adolescents are at high risk of contracting STIs and HIV as a result of their involvement in casual and unprotected sex.9 Another study further revealed that many female adolescents in southeast Nigeria had a variety of STIs: 11% had trichomoniasis, another 11% had chlamydial infection, 82% had vaginal discharge, while 26% had candidiasis.16 STIs predipose to HIV infection.17 The Need for In-depth Knowledge of Adolescent Sexual Behaviour in Diverse Cultural Groups in Nigeria Studies that have so far been carried out and reported represent interesting and significant contributions in the area of adolescent sexual behaviour. However, they have limited national coverage in their sample populations. A significant proportion of the surveys have focused only on adolescents in the southern parts of the country and not representative of those in the northern parts. This is because most of the researchers in this area of reproductive health are based in the south.18 The 1999 NDHS appears to show an exemption because it is a representative nationwide study with some insights on adolescent sexual practices. Nevertheless, the survey lacks depth in understanding adolescent sexual knowledge, attitudes, preferences and behaviours in relevant contexts. The dearth of information about the sexual practices of adolescents in northern Nigeria is quite worrisome given the twin knowledge that risk reduction efforts are more effective when culturally sensitive19, and that ethnicity is one of the major variables associated with sexual behaviour and risk.20 A preponderance of research studies that do not reflect countrywide characteristics will obviously lack overarching empirical basis with which to compare, evaluate and guide ongoing research across national geographic regions and cultures. This is very important as the 1991 national provisional census figures shows that one in every five persons fall within the 10–19-year age group. The need for cross-cultural comparison of adolescent sexual behaviour is further necessitated by the extreme diversity of the Nigerian population. The country has over 250 ethnic groups, with about 10 notable cultural groups, namely, Hausa-Fulani, Yoruba, Ibo, Kanuri, Tiv, Edo, Nupe, Ibibio and Ijaw, accounting for nearly 80% of the total population.21 Equally compelling is the need to obtain knowledge of national adolescent sexuality patterns and dynamics in order to plan intervention programmes based on specific and general cultural findings. However, some intervention programmes have been developed and implemented countrywide to encourage adolescents' rational decisions on safe sexual and reproductive behaviour despite the relatively low level knowledge of adolescent reproductive and sexual behaviour in some cultural groups. Urgent attention is still required in terms of information that suggests appropriate interventions in certain aspects of adolescent sexuality in Nigeria. Such knowledge would entail awareness of any trends and differentiation available in the country's diverse cultural areas in order to systematise the interventions. In all, availability of reliable and in-depth countrywide adolescent sexual and reproductive information will facilitate design of effective policies, programmes and strategies. Quite important also is the fact that such knowledge will suggest predictors that are or are not culture-specific, and regional priorities and peculiarities may be established to accommodate various needs. Our purpose in this study was to obtain in-depth information about sexual activities, beliefs, perceptions, knowledge and experience of adolescents in Niger State of Nigeria. As previously mentioned, less research has been conducted on samples from diverse cultural backgrounds, especially in Niger State where some of the Gwari and Hausa ethnic group members reside. Niger State lies between latitudes 8o and 10o north and longitudes 4o and 8o east. The state shares a common boundary with Sokoto State to the north-west, Kaduna and Plateau States to the east, Kwara State to south-west, and Federal Capital Territory (FCT) to south-east. The 1991 country provisional census puts the population of Niger State at 2,421,581, (1,169,115 females and 1,252,466 males). The inhabitants of the state are mostly Moslems, Christians, or African traditional religionists. Agriculture is the mainstay of the state's economy, the main agricultural products being guinea corn, maize, millet, cassava, yam, groundnut and rice. The study is essential to understanding how to reduce HIV transmission in the state. A survey conducted in 2000 puts the HIV seroprevalence rate in the country at 5%.22 There are, however, regional disparities in the rates. It is 3.4% for Niger State. It is the lowest among states in the north central zone of the country. The zone's seroprevalence average is 7.6%, with some states like Benue having a rate of 14.9%. The neighbouring states of Kaduna, Plateau and FCT had 6.5%, 6% and 7.9% respectively.23 METHOD To be representative of the range of ethnic groups and levels of development and family planning use in the state, survey data were collected through a multi-stage probability sample of adolescent males and females living in rural and urban areas, as part of a larger study. To estimate an appropriate sample size, it was assumed that 50% of the adolescents had accurate understanding of reproductive health. The sample size within four percentage points of 50% with a 95% confidence interval for the cluster sampling technique was 612. To increase precision, a total of 898 adolescents were interviewed. Twenty eight cluster sites were randomly selected for the survey; 15 in urban and 12 in rural areas. About 32 respondents were included per cluster. Within each cluster, local government areas (LGAs) were randomly selected. The LGAs are Chanchanga, Mariga, Shiroro, Agwara, Gurara and Agaie. Subsequently, wards were randomly selected within the LGAs. The survey team enumerated schools and economic units in the wards. Respondents were afterwards selected from the sampled sites at defined intervals from a random start to obtain the desired sample size. A survey questionnaire was used in the study. The questionnaire included 105 close and open-ended questions on demographic characteristics, sexual behaviour, marriage and reproduction, contraceptive knowledge and use, sexually transmitted diseases including HIV/AIDS, abortion, and family planning. Prior to use in this study, the questionnaire was field-tested on a group of adolescent females and males in one rural and one urban area (these were different areas from those in the study sites). This was to identify any possible gaps and redundancies in the questionnaire, given local conditions and sensitivities of people in the areas as well as to check for language. The questionnaire was subsequently amended appropriately before use. A separate pilot test of the questionnaire provided test-retest reliability. Kappa reliabilities on items ranged from 0.73 to 1.0. Because the questionnaire did not yield a total score, reliability of the summed score could not be assessed. Male and female interviewers were trained during a three-day workshop. A representative population-based survey of adolescents was completed in all the selected LGAs between November 1997 and May 1998. Male interviewers worked with male respondents while female interviewers worked with female respondents. Data from the survey were coded and then entered into a computer using the SPSS 6.1 software. Simple percentages, descriptive measures and correlation analyses were computed to establish relationships among variables. Chi-square tests of independence were conducted. Relationships between relevant demographic and sexual/reproductive variables were assessed. The relationships were reported if they were statistically significant at p < 0.05. RESULTS Characteristics of the Sample There were 439 (48.9%) male respondents and 459 (50.9%) female respondents (Table 1). Some 52.9% were from the urban areas while the remaining 47.1% were from the rural areas. The respondents ranged in age from 11 to 25 years (mean age = 16.8 years, SD = 2.1). Eighty five per cent of them were aged between 14 and 20 years. Although majority of the respondents were Hausa (21%) and Gwari (44%), some of them were from other ethnic groups, particularly Ibo (15.5%) and Yoruba (8%). A slightly higher proportion of them were Muslims (51.0%), while 43% were Christians. Only 2.4% were married while a vast majority of 94.5% were single. Of the single respondents, about 62% lived with both parents while 9% were living with their mothers and 8.8% with their fathers. A larger percentage of all the respondents (63.3%) had fathers with only one wife while 34% had fathers in polygamous relationships. The presence of respondents from polygamous families apparently explains a wide sibling size range of between 0 and 25. Majority of the respondents (74.2%) had sibling size of between one and eight. Most of the respondents' fathers (34.8%) were civil servants while others were either traders (18.3%) or farmers (25.5%). The respondents had at least one form of education. Seventy two per cent were in school (72%) while 28% were out of school at the time of the study. About 98% had either some primary education or completed primary school while about 2% had some secondary education.b b The decision to present the socio-demographic characteristics of in-school and out-of-school respondents together (as in Table 1) was statistical. Except for education, the respondents did not show any statistical difference (p < 0.05) on any of the demographic variables including urban/rural residency Sexual Behaviour Some of the respondents were sexually experienced. Almost one third (32.7%) said they had already had their first sexual experience while 66% said they had never had sexual relations. Of those who had already had their first sexual intercourse, 64% were males and 36% were females. More out-of-school (55%) respondents said they had already had their first sexual intercourse than in-school respondents (45%). Further, slightly more rural (53%) than urban (43%) respondents reported that they had had their first sexual intercourse. Most of those who had already had sexual relationships (86%) claimed that they started when they were between ages 13 and 20 years. During their first sexual intercourse, about 35% said that either they or their partners used a particular family planning (FP) method to avoid pregnancy. The remaining 65% indicated that they did not use any family planning device because they were not aware of any method. Most of the respondents (54.1%) who had already had sexual experience also reported having more than one sexual partner. More of them were males (66%) than females (44%). Slightly more in-school respondents (55%) reported that they had more than one sexual partner than the out-of-school respondents (53%). The frequency of the respondents' sexual intercourse ranged between 0 and 13 times in the past one week before the survey. Majority of them (84.4%) said they had sexual encounters for 1–6 times during the period. Slightly more males (54%) than females (46%) were in this category. Most of the sexually active respondents (58%) said they had sexual intercourse for pleasure. About 22% said they wanted to test their fertility, and 7% said they did it to test their sexual capability. Apparently, the frequent sexual activities of the respondents may be explained by how they spent their free time. Only few respondents reported doing extra reading or serious work during the period. Majority (61%) said they engaged in playing games and sleeping. All the respondents attempted to obtain information about sexual issues. About 23% said they obtained information from friends, another 23.2% said they sought information from physicians, while 18.3% said their parents provided information for them. More males than females (83.3% vs. 16.7%) between ages 14 and 20 years said they had engaged in their first sexual intercourse (c2 = 19.68, df = 10, p < 0.03). However, more females (42.2%) than males (16%) had a higher probability of engaging in their first sexual intercourse at earlier ages of between 11 and 13 years (c2 = 25.51, df = 3, p < 0.00001). Likewise, more out-of-school respondents (55% vs. 45%) reported that they had engaged in their first sexual intercourse than their in-school counterparts (c2 = 22.4, df = 10, p < 0.05). None of urban/rural residency, education and religion had influence on probability of occurrence of first sexual intercourse. Majority of the repondents with primary education (85%) said they had sexual intercourse for pleasure, while 10% of those with secondary education gave the same reason (c2 = 69.4, df = 50, p < 0.03). Marriage and Reproduction Of all the respondents, 95.7% indicated that they were not yet married while 3.6% said they were married. Eighty seven per cent of out-of-school respondents said they were married, while 13% of in-school respondents said they were married. Fifty six per cent of the married lived in the rural areas while 44% lived in the urban areas. Most of those in marital relationships got married between ages 15 and 17 years in the church or mosque or at civil forms of marriage. About one half were in monogamous relationships with equal percentage in polygynous relationships. Of all the married respondents, majority (81%) already had 1–5 children. Almost all (92%) had been married for 1–6 years. Nearly 65% chose their own spouse while others had their parents choose for them. Their spouses were between 20 and 31 years. Both married and unmarried respondents had various expectations of marriage. Most of the respondents (32.6%) believed that the ideal age for females to get married is between ages 14 and 18 years. In contrast, only few respondents (2.1%) thought that males should get married at this age. About one third of all respondents believed that the ideal age for males to get married is between 23 and 26 years, while another one third thought that males should get married at an older age, between 27 and 32 years. Respondents also expressed their fertility preferences. Majority of them (73.7%) said a boy/girl should remain a virgin until marriage, while 22.3% (a percentage slightly lower than those who had already had sexual intercourse) thought otherwise. When married, most respondents (60%) preferred to have between four and six children. Two thirds preferred up to four male children while the remaining preferred 2–3 male children. Generally, about one half of all respondents said God determines how many children a couple should have. Twenty per cent thought that the husband should decide and 4% said the wife should decide. Seventeen per cent felt that both husband and wife should decide together. More Muslim respondents would prefer to have more than five children, compared to Christian respondents (c2 = 19.84, df = 9; p < 0.001). However, female respondents were more likely to refer decisions about number of children appropriate for them to God or Allah than male respondents (c2 = 23.06, df = 5; p < 0.0003). Unlike respondents from other ethnic groups, more Hausa and Gwari respondents believed that God or Allah determines how many children a married couple should have (c2 = 101.484, df = 50; p < 0.001). Also, more Muslims than Christians believed that God decides the number of children a couple should have (c2 = 61.61, df = 9; p < 0.05). More male (62.7%) than female (37.3%) respondents would want a boy or girl to be a virgin before marriage (c2 = 21.28, df = 1, p < 0.001). Likewise, more of those who had not had their first sexual intercourse (83%) believed that someone should remain a virgin till marriage than those (17%) who had already had their first intercourse c2 = 31.4, df = 1, p < 0.001). Further, more Muslims (51.3%) than Christians (46.9%) preferred a boy or girl to remain a virgin till marriage (c2 = 9.05, df = 3; p < 0.028). Majority of Hausa (73%) and Gwari (80%) respondents said they got married when they were between 15 and 19 years, in contrast to Yoruba (10%) respondents (c2 = 21.52, df = 8, p < 0.005). Of those who said they were pregnant at the time of the survey, 80% had completed primary education, while 13% had completed secondary education (c2 = 18.61, df = 5, p < 0.002). Similarly, more of the respondents who were out-of-school were pregnant at the time of the survey than in-school respondents (c2 = 44.7, df = 1, p < 0.0001). More respondents who had completed primary education (89.7%) than those with higher education (35.6%) were likely to report that they had given birth (c2 = 12.269, df = 5; p < 0.0002). Sexually Related Diseases and Induced Abortion Almost all the respondents (91.9%) were aware of HIV/AIDS while all of them had knowledge of various forms of STDs. Majority of them (76.6%) knew about gonorrhoea, 25.7% had heard about syphilis, about 7% knew about herpes, 21.3% had knowledge of pubic lice, and only 3% had knowledge of chlamydia. Majority of the respondents obtained sexually related information on sexual disease prevention and cure from people outside their immediate family — teachers (25.6%), friends (13.3%) and medical personnel (21.9%). Few respondents (8.4%) obtained such information from their parents. More than half of the respondents (58.7%) acknowledged that there were no cures for AIDS; another 36% felt that AIDS could be cured if detected early. Seventy seven per cent were aware that HIV could be transmitted through heterosexual intercourse. Similarly, most respondents were aware of other ways of transmitting HIV. Eighty per cent thought it could be transmitted through sharing needles; 84.4% knew that a pregnant woman could pass it to her unborn child. About half of the respondents said the use of antibiotics before sex could protect one from contracting STDs. Sixty one per cent affirmed that STDs could be contacted from unclean toilet seats. Some respondents had ideas of how to avoid contracting HIV/AIDS. Only 27.2% mentioned condom use, 16% thought that avoiding casual sex could prevent it, while 21% believed that having sex with multiple partners or prostitutes could aid infection with HIV/AIDS. Seventy two per cent were aware that STDs could be cured. Ninety per cent would agree to consult a physician or visit a hospital if they had any of the STDs, 0.6% would report such disease to family members and 3.2% would visit a native doctor. Six per cent of respondents reported that they or their partners had been pregnant and aborted the pregnancy.c Majority of those respondents who had had abortion have done so for 1–3 times. Almost all the abortions took place in the hospital with various consequences. Six out of every 10 reported satisfactory outcome while every other one reported death of a partner, and every other three reported medical complications. c This may however be a conservative percentage in the past one year, since some females would avoid telling their partners about their experience of induced abortion for fear of the partner telling others and the perceived consequent social stigmatisation. Associations were sought between respondents' sexual preventive measures and each of the socio-demographic variables. More female (52.6%) compared to male (47.4%) respondents had heard of HIV/AIDS at the time of interview (c2 = 6.93, df = 1, p < 0.008). More Hausa (53%) and Gwari (55%), compared to either Yoruba (7.3%) or Igbo (11.9%) respondents, felt that HIV infection could be prevented if one does not have multiple sexual relations (c2 = 402.17, df = 150, p < 0.0000). More female (91.3%) than male (8.7%) respondents obtained sexual health information from nurses (c2 = 137.37, df = 13, p < 0.0000). More of Gwari (53%) and Hausa (49%) respondents obtained sexual health information from physicians than Yoruba (14%) and Igbo (20%) respondents (c2 = 165.33, df = 130, p < 0.01). More males than females (88% vs. 14.5%) believed that the condom is useful for HIV/AIDS prevention (c2 = 127.81, df = 15, p < 0.0000). Majority of female (82%), compared to male (6%) respondents would seek care from a native doctor if infected with STDs (c2 = 71.23, df = 30, p < 0.000). However, more males (62%) than females (37%) thought a girl should seek a physician's help for an unwanted pregnancy (c2 = 55.23, df = 11, p < 0.0000). Family Planning At the time of the survey respondents had some knowledge of FP methods. Condom was well known by 63.8% of them. They had knowledge of other methods, namely, pills 51%, injectables 59.5%, foaming tablets 51.2% and withdrawal method 53.9%. Fewer respondents (47.9%) had knowledge of IUD, diaphragm 42.4%, female sterilisation 48.8%, male sterilisation 41.9% and rhythm 49.3%. Only 9.7% reported that they or their partners had ever used pills during sexual relationships, while a slightly higher proportion (10%) said they had used the rhythm method. Condoms were used by 12.5% while nobody ever used the male and female sterilisation methods. At the time of the survey 6.3% were using the condom, while 2.1% reported that they or their partners were using pills. Only 1.2% were using the withdrawal method. Current use for other methods was 0.7–1.1%. One half was not interested in using any FP method in future, they complained that it could reduce sexual pleasure, while 44.5% were interested in using a method in future. Eleven per cent would like to use pills, 15.4% expressed willingness to use condom, while 17.3% would prefer the injectables. More than half of the respondents knew where to obtain information about FP methods. Of these, one third mentioned the doctor as their source of information, another one third said it could be obtained through the media and 6% mentioned the Planned Parenthood Federation of Nigeria (PPFN). There was association between respondents' first source of information about FP and their sex, ethnic group and religion. More males (83.4%) than females (22.4%) had their first source of information about family planning from friends (c2 = 42.62, df = 6, p < 0.0000). Compared to respondents from other ethnic groups, more Hausa respondents said their first source of information was medical personnel (c2 = 85.85, df = 60, p < 0.015). In addition, more Christians (63.2%) than Muslims (32%) reported that they had their first information about FP from books and novels (c2 = 66.41, df = 18, p < 0.0000). More Hausa (44%) and Gwari (45%), compared to either Yoruba (13.5%) or Igbo (19%) respondents did not use any FP method during their first intercourse for lack of knowledge of the methods (c2 = 127.32, df = 63, p < 0.0000). More male (54%) than female respondents used a FP method with their partners to avoid pregnancy (c2S = 4.7, df = 1, p < 0.02). Likewise, more male (54.5%) than female (45%) respondents would like to use a FP method in future sexual encounters (c2 = 9.05, df = 1, p < 0.002). More Hausa (46%) and Gwari (54%) than Yoruba (8.2%) and Igbo (18.8%) respondents would be willing to use a FP method in future (c2 =19.46, df = 3, p < 0.0002). DISCUSSION AND CONCLUSION Based on the results of our survey we could generally say that about one third of adolescents of all socioeconomic status in Niger State have already experienced their first sexual intercourse. Specifically, 32.7% (36% females and 64% males; 55% out-of-school and 45% in-school) of the respondents in the present study had already had their first sexual initiation. On adolescents' educational status, the percentage obtained in the present survey appears slightly lower than reports from most other surveys on first intercourse among adolescents in parts of the country. For instance, some studies showed 40% of adolescent schoolgirls in Lagos5, 62% of in-school students in Ilorin9, and 55% of in-school adolescents in the southeastern part of the country.10 In the present study, more males than females had already had first sexual relationship. This finding is consistent with reports of 40% of female and 50% of male adolescents in rural and urban Enugu, Kaduna, Lagos, Onitsha and Zaria who had already had their first sexual contacts.7 The present finding is also consistent with results that more adolesent males than females in Ilorin had had their first sexual encounters by age 19.9 This study found that about 54% of adolescents who had already had their first sexual experience also reported that they had more than one sexual partner. This finding is slightly higher than reports from some other parts of the country; 48% in Ibadan12, and about 35% of female adolescents in Benin.8 Similarly, our finding shows that 84% (46% females and 54% males) of sexually experienced respondents were sexually active with up to six sexual encounters in the past one week before the survey. This proportion is lower than 77% found among adolescent schoolgirls in Benin8, and about 71% in the general northern female adolescent population.13 The percentage observed in our study is also lower than 62% found among in-school adolescents in Ilorin and 55% among schoolgirls in southeastern Nigeria.9-10 When compared with earlier studies in Lagos, Benin, Ibadan and the southeastern part of the country5,10,12, the respondents in this study had information about HIV/AIDS and at least one STD. Except for gonorrhoea and syphilis, they were not familiar with most other examples and cases of STDs. Significantly more males than females had no knowledge of the term HIV/AIDS. Similarly, a vast majority of respondents lacked knowledge of effective method of HIV/AIDS prevention. Less than 28% of respondents were aware that the infection could be prevented by using the condom, and avoiding multiple sexual partnership and casual sex. Significant findings that differentiate local Gwari and Hausa respondents from other adolescent inhabitants who were indigenes of other ethnic groups were observed in the study. First, most Gwari and Hausa respondents acknowledged that they married at an earlier age than Yoruba respondents. Second, compared to Yoruba and Igbo respondents Gwari and Hausa respondents mostly believed that God determines how many children a couple should have. Third, more Gwari and Hausa respondents felt that HIV infection could be prevented by not having multiple sexual partners than Yoruba and Igbo respondents. Fourth, compared to Yoruba and Igbo respondents, majority of Gwari and Hausa respondents said they obtained sexually related information from physicians. Fifth, most Gwari and Hausa respondents said they did not use any FP method during their first sexual relationships compared to Yoruba and Igbo respondents. However, more of the Gwari and Hausa respondents wish to use a FP in future than respondents from other ethnic groups. Consequently, it is necessary to systematise future interventions on sexual and reproductive health in line with ethnic differences in perceptions and sexual practices of adolescents in Niger State observed in this study. There is need for interventions to consolidate on the Gwari and Hausa belief that involvement in multiple sexual partnership can lead to increased rate of HIV transmission. The interventions should also aim to promote knowledge and use of safe FP methods among the Gwari and Hausa indigenes, since majority of them marry at a younger age, do not frequently use any method at first sexual intercourse, and are ignorant of FP methods. This is consistent with the directive of the UN ICPD that couples and individuals should have access to the widest possible range of safe and effective FP methods.25 Accordingly, stakeholders in the health sector should ensure that FP methods are available at affordable prices to the inhabitants. Evidently, a wide disparity between contraceptive knowledge and use was found for all the respondents. Knowledge rate was between 37% and 63.8% while use rate was between 0.7% and 12.5% for the contraceptive methods studied. This latter finding is in contrast to an earlier finding among adolescents in Kwara State, which observed that condom and other contraceptive use rates were as high as 20.6%.18 The overall induced abortion rate suggests that about 6% of adolescent females in Niger State have abortion each year. Although almost all the abortions took place in hospital settings, only about six out of every ten females in these regions who had had an abortion reported satisfactory outcomes. In addition, about three out of every ten suffered some medical complications resulting in loss of productive days. The remaining one out of every ten died. One prominent observation in the study is that recorded abortion rates were not affected by any background characteristics of respondents including rural-urban differences. The high rate of medical complications and death of females who had abortions in this study, like in previous research report19, is suggestive of a continuing need to improve access to hospital care. There is also a need for improved contraceptive counselling for adolescents so as to increase contraceptive use among the sexually active. Experimental studies outside Africa tend to demonstrate that women in areas with enhanced FP services are more likely to adopt contraceptive use and less likely to have unplanned pregnancies and thus have fewer needs for abortion.26-27 Local health authorities should, therefore, make available effective and free contraceptive services to adolescents. The policy implication of this result is the need for programmes designed to provide adequate knowledge on reproductive and sexual issues to adolescents and help change their attitudes towards reducing their sexual risk behaviours. ACKNOWLEDGMENT This study was funded by the World Bank through collaborative effort of the Population Research Fund Management of the Nigerian Institute of Social and Economic Research (NISER). REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02038t1.jpg] [rh02038t3.jpg] [rh02038t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}