 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 93-97 Prevalence of Asymptomatic Genital Infection among Pregnant Women in Benin City, Nigeria John Akerele1, Philip Abhulimen1 and Friday Okonofua2 1Department of Pharmaceutical
Microbiology, University of Benin, Benin City, Nigeria. 2Department
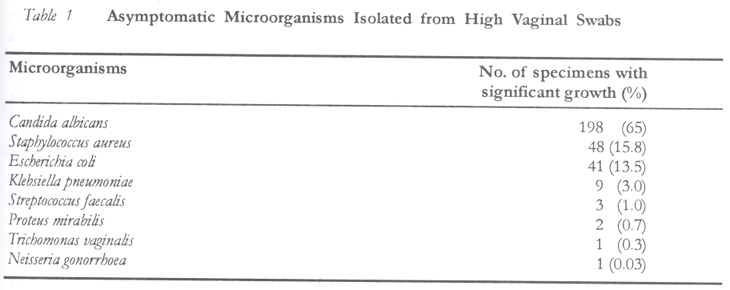
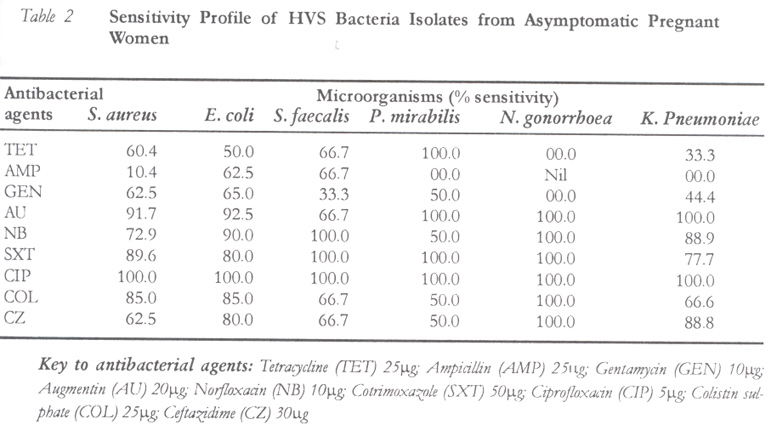
of Obstetrics and Gynaecology, University of Benin, Benin City, Nigeria. Code Number: rh02039 ABSTRACT The prevalence of asymptomatic genital infection among pregnant women and their susceptibility to antibacterial agents was investigated to provide baseline data on common asymptomatic genital microorganisms and identify potentials for development of clinical disease among this cohort of patients. High vaginal swabs were obtained from five hundred consecutive and consenting pregnant women attending the antenatal clinic of the University of Benin Teaching Hospital (UBTH) and the Central Hospital, both in Benin City, Nigeria. A total of three hundred specimens showed significant microbial growth, giving a prevalence rate of 60% for asymptomatic genital infections. Candida albicans (65%), Staphylococcus aureus (51.8%) and Enterobacteriacae (E. coli and Klebsiella species) were predominantly isolated, followed by Trichomonas vaginalis and Neisseria gonorrhoea. Most of the bacterial isolates were susceptible to ciprofloxacin, ceftazidime, cotrimoxazole, norfloxacin and augmentin. All the isolates except Streptococcus faecalis were resistant to ampicillin. These results show a high rate of asymptomatic genital tract infections among pregnant women in Benin City, which have implications for adverse maternal and neonatal outcomes. (Afr J Reprod Health 2002; 6[3]: 93–97) RÉSUMÉ Prévalence de l'infection génitale asymptomatique chez les femmes enceintes à Benin City. Nous avons étudié la prévalence de l'infection génitale asymptomatique chez les femmes enceintes et leur susceptibilité aux agents antibactériens, afin de fournir des données de base sur les micro-organismes génitaux asymptomatiques. Nous avons voulu aussi identifier les capacités pour le développement de la maladie clinique chez les cohortes de patients. Des écouvillons vaginaux de haute densité ont été obtenus de 500 femmes enceintes consécutives et consentantes qui fréquentent la consultation prénatale au Centre Hospitalier Universitaire à Benin City (UBTH) et à l'Hopîtal Central, également à Benin City, au Nigéria. Au total, 300 échantillons ont manifesté une croissance microbienne, indiquant un taux de prévalence de 60% pour les infections genitales asymptomatiques. Candida albicans (65%), Staphylococcus aureus (51,8%) et enterobacteriaceac (les espèces E. coli et Klebsiella) ont été en grande partie isolés, suivis de Trichomonas vaginalis et Neisseria gonorrhoea. La plupart des isolates bactériens étaient susceptibles au ciprofloxacin, au ceftazidime et à l'augmentin. Tous les isolates sauf Streptococcus faecalis étaient résistants à l'amplicillin. Les résultats ont montré un taux élevé des infections de faisceau genital asymptomatique chez les femmes enceintes à Benin City, ce qui a des implications pour les conséquences néo-natales et maternelles défavorables. (Rev Afr Santé Rerod 2002; 6[3]: 93–97) KEY WORDS: Genital infection, pregnant women, antibacterial agents, Nigeria. INTRODUCTION There is evidence to suggest that pregnancy may increase the risks of genital and urinary tract infections.1 Many asymptomatic genital infections have been associated with preterm birth, a common cause of neonatal morbidity and mortality.2 There are genital infections caused by E. coli, Klebsiella, Aerobacter, Proteus, Providencia, Pseudomonas, Facultative anaerobes, Staphylococci and Streptococci have been reported.3 Vaginal discharges caused by Trichomonas vaginalis and Neisseria gonorrhoea are commonly reported genital infections.4 The prevalence of asymptomatic genital tract infection has been widely reported in pregnant women.3-5 Kaitz and Hodder6 reported that the prevalence of asymptomatic genital infections in pregnant black women is appreciably higher than in pregnant white women. Turch et al7 found no significant difference in the prevalence of genital infection among black and white patients of the same socioeconomic group. High prevalence of symptomatic infections has also been reported in women attending public clinics who are financially indigent.8 The report of Rantz9 show that women in the high socioeconomic strata with relatively minor symptoms of genital infections are more likely to seek medical aid. Pregnant women carriers of group B Streptococci are known to have greater risk of early onset of invasive disease.10 Significant association of some lower genital tract organisms and infections with preterm birth or preterm rupture of the membrane has been reported.11 The human host response to genital microorganisms through the elaboration of cytokines and proteolytic enzymes has also been reported.12 Aerobic vaginitis with aerobic microorganisms like group B Streptococci and E. coli has been hypothesised to be mostly responsible for pregnancy complications.13 The objective of this study is to provide baseline data on the common asymptomatic genital microorganisms and the potentials for development of clinical disease in pregnant women from this area of research. MATERIALS AND METHODS Patients and Specimens Collection A total of 500 consecutive and consenting pregnant women attending antenatal clinics at the University of Benin Teaching Hospital (UBTH) and the Central Hospital, both in Benin City, were enrolled in the study. All the women were attending the clinics for the first time in pregnancy. They were non-smoking and had not taken any antibacterial agent for any reason at least two weeks prior to the study. The women were aged 15–35 years (mean = 28 years). There was no history of symptoms of genital tract infections or recent use of any antibiotics. The study was approved by the UBTH ethical review committee. Microscopy High vaginal and endocervical swabs were obtained from each of the women with the assistance of a nurse/midwife. The swabs were streaked onto blood agar, saboraud-dextrose agar, McConkey agar and chocolate agar plates in duplicates. A set of the inoculated plates was incubated aerobically and a second set incubated anaerobically using a properly operated anaerobic jar. The aerobic plates were incubated at 37oC for 18–24 hours and the anaerobic plates for 72 hours. Colonies of bacteria from media plates that showed significant growth (105 Cfu) were identified by appropriate gram stain and biochemical methods following the protocol of Cowan and Steel.14 A broth culture of each of the bacterial isolates was prepared and subjected to antimicrobial susceptibility using the multidisc diffusion method.15 RESULTS A total of 300 specimens showed significant microbial growth, representing prevalence rate of 60% for asymptomatic genital microbial growth. The distribution of isolates among the specimens is as shown in Table 1 while their sensitivities to various antibacterial agents are listed in Table 2. Candida albicans (65%) and Staphylococcus aureus (15.8%) were predominantly isolated, followed by Trichomonas vaginalis and Neisseria gonorrhoea. Combined infection with E. coli and Klebsiella appeared frequently in our study. Staphylococcus aureus and E. coli were sensitive to all the tested antibacterial agents except ampicillin. Staphylococcus faecalis and Neisseria gonorrhoea were sensitive to norfloxacin, co-trimoxazole and ciprofloxacin. Klebsiella pneumoniae was sensitive to only augmentin and ciprofloxacin. DISCUSSION The commonly reported infections associated with pregnancy are urinary tract infections (asymptomatic bacteriuria, cystitis and pyelonephritis), which are frequently encountered as medical complications of pregnancy.16 Although the majority of infections in pregnancy are asymptomatic, the mother is placed at high risk for low birth weight and preterm birth. Pyelonephritis, for instance, could cause significant maternal and fetal morbidity and mortality.16 The organisms commonly isolated in asymptomatic pregnant women are E. coli, Klebsiella pneumoniae and Proteus mirabilis.17 However, our study showed the preponderance of Candida albicans and Staphylococcus aureus, which corroborates the observations of Lewis18, who reported the common occurrence of Candida albicans during pregnancy with the associated white patches of thrush on the vaginal wall. Stanley19 also observed that Candida albicans occurred more frequently in pregnant patients with glycosuria, but our study did not investigate the underlying possible biochemical status of the patients. As a result of lack of facilities in our laboratory, the study design could not detect other clinically important pathogens such as Chlamydia trachomatis, Group B Streptococcus and Gardnerella vaginalis. In an earlier analysis of urine specimens from the same patients, there was a high prevalence of E. coli, Klebsiella species and Staphylococcus species.17 Our results are similar to literature reports, where cultures from symptomatic pregnant women yielded E. coli, Klebsiella species and Proteus mirabilis.20 In the absence of DNA amplication tests, which are employed in similar studies in developed countries, our data show some correlations between organisms found in endocervical swabs and urine of pregnant women in this area of study. Our results show that Staphylococcus isolates were highly sensitive to ciprofloxacin and augmentin, just as E. coli was sensitive to norfloxacin, ciprofloxacin and augmentin. Streptococci faecalis was very sensitive to co-trimoxazole, norfloxacin and ciprofloxacin. Proteus mirabilis and Neisseria gonorrhoea were very sensitive co-trimoxazole, norfloxacin and ciprofloxacin. Co-trimoxazole was very effective against all the bacterial isolates. This observation corroborates the works of Peter et al21 and Delzell and Lefevre3, who reported that most of the isolates encountered asymptomatically in pregnancy were highly sensitive to co-trimoxazole. It is plausible to recommend in the light of these observations that co-trimoxazole regime could be part of the routine drug management of pre-natal genital infections among pregnant women in general. The rationale for this strategy would be the avoidance of selection pressure occasioned by careless administration of broad spectrum antibacterial agents, as it is often and usually the case in this area, without prospective study. We observed in this study that Staphylococcus aureus and E. coli were resistant to ampicillin, a finding that is at variance with earlier observations20, where ampicillin was the most useful first line antimicrobial agent. Our findings support the recommendation of Delzell and Lefevre3, which discourages the use of ampicillin in the treatment of asymptomatic genital infections because of high rates of resistance. The high resistance to ampicillin could possibly be due to the high prevalence of self-medication and misuse of ampicillin, usually without prescription, with the resultant emergence of resistance gene pools, following the selection of resistant bacterial strains. Neisseria gonorrhoea was found to be sensitive to all the antibacterial agents tested in this study. This is a welcome development since Neisseria gonorrhoea infection is a common complication of pregnancy. This study has provided baseline data on symptomatic genital microorganisms, which can cause neonatal mortality and morbidity. Since abundant clinical and laboratory information suggests that subclinical infection is a major cause of preterm birth, new approaches including systematic screening and antibacterial coverage should be developed to prevent prematurity. ACKNOWLEDGEMENT The secretarial assistance of Hope Onoshevwe and the receipt of University of Benin research grant (URPC) for this study are gratefully acknowledged. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02039t2.jpg] [rh02039t1.jpg] |
| |||||||||

{kind=link}
{kind=link}