 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 98-102 Cervical Ripening: How Long can the Foley Catheter Safely Remain in the Cervical Canal? Ekele BA1 and Isah AY1 1Department of Obstetrics
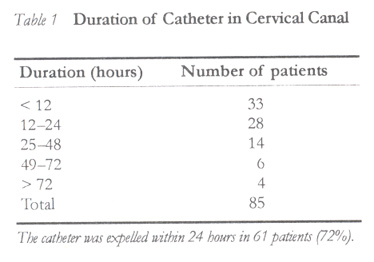
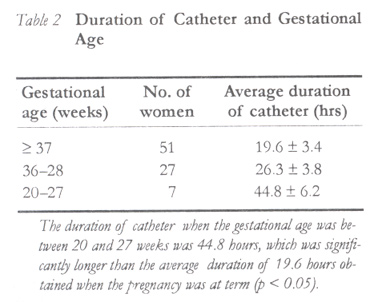
and Gynaecology, Usmanu Danfodiyo University Teaching Hospital, Sokoto, Nigeria. Code Number: rh02040 ABSTRACT This was a prospective study involving 85 patients admitted for induction of labour with unfavourable cervix at Usman Danfodiyo University Teaching Hospital, Sokoto, Nigeria. A size 16–20 Foley catheter was passed transcervically into the extra-amniotic space under aseptic technique and the balloon inflated with 30–50mls sterile water. Each patient was placed on prophylactic antibiotics. The balloon was expelled within 12 hours in 22 (39%) patients. Twenty eight patients expelled the balloon in 12–24 hours, 14 in 25–48 hours, 6 in 49–72 hours and 4 after 72 hours. The average duration of catheter placement when the gestational age was 20–27 weeks was 44.8 hours, which was significantly longer than 19.6 hours obtained for term pregnancies (p << 0.05). Induction of labour was successful in 77 (91%) patients and there was no significant maternal morbidity. The results of our study suggest that the balloon of the Foley catheter can safely remain in the extra-amniotic space longer than 24 hours for cervical ripening if the cervix is unfavourable, provided the membranes are intact and the feto-maternal conditions remain satisfactory. (Afr J Reprod Health 2002; 6[3]: 98–102) RÉSUMÉ La maturation du col: Pour combien du temps peut rester la sonde de Foley en sécurité dans la cavité du col? Il s'agissait d'une étude prospective concernant 85 patientes qui ont été admises au Centre Hospitalier Universitaire Usman Danfodiyo à Sokoto, Nigéria pour le déclenchement du travail avec du col hostile. Une sonde de Foley à la taille 16–20 a été introduit transcervicalement dans l'espace extra-amniotique sous la technique aseptique, le ballon ayant été gonflé de 30–50 mls de l'eau stérile. Chaque patiente prenait des antibiotiques prophylactiques. Le ballon fut expulsé en 12 heures chez 22(39%) des patients. 28 patientes ont explusé le ballon en 12-24 heures, 14 en 25–48 heures, 6 en 49–72 heures et 4 après 72 heures. La durée moyenne pour la mise en place d'une sonde quand l'âge gestationnel était 20–27 semaines était 44,8 heures, ce qui était plus long que 19,6 heures que nous avons obtenu pour les grossesses à terme (p 0,05). Le déclenchement du travail a réussi chez 77 (91%) des patients; il n'y avait pas de morbidité maternelle appréciable. Les résultats de notre étude ont montré que le ballonet de la sonde de Foley peut rester en toute sécurité dans l'espace extra-amniotique plus de 24 heures pour la maturation du col si le col est hostile, pourvu que les membranes soient intactes et que les conditions foeta-maternelles restent satisfaisantes. (Rev Afr Santé Reprod 2002; 6[3]: 98–102) KEY WORDS: Catheter balloon, cervical ripening, insertion-expulsion interval INTRODUCTION A few weeks before the onset of labour, the cervix prepares for labour with anatomic, histologic and biochemical changes. These changes in the uterine cervix and lower segment that normally precede the onset of parturition are termed cervical ripening. There is little doubt that cervical ripening facilitates labour and ultimately influences the prospects of vaginal delivery.1,2 Induction of labour when the cervix is unripe is associated with maternal complications and high rates of induction failure.3 Numerous techniques have been used to ripen the unfavourable cervix to achieve the changes necessary for labour.4,5 The use of Foley catheter to effect cervical ripening was first described by Embrey and Mollison in 1967.6 Thereafter, various balloon catheters have been used to induce cervical ripening.7 However, the simple Foley catheter, which can be passed readily through an undilated cervix before being inflated, has become one of the most popular methods. It has been established that cervical ripening with extra-amniotic catheter balloon possesses the advantages of simplicity, low cost, reversibility, lack of systemic side effects and efficacy that is similar or better than other methods.8,9 What is yet to be determined is how long such a catheter can be safely placed in the cervical canal until the cervix becomes favourable. Equally important is the issue of cervical ripening before 37 completed weeks of gestation. At the Usmanu Danfodiyo University Teaching Hospital, Sokoto, in northern Nigeria, the only option available to us when the cervix is unfavourable is the use of the Foley catheter. Prostaglandins, for instance, are not readily available apart from its prohibitive cost. We had to make the best use of what is available under such circumstances. An earlier study from our department reported the safe use of the catheter for cervical ripening in the presence of fetal demise.8 The objective of this present work was to determine how long the extra-amniotic catheter balloon can remain when used for cervical ripening before its spontaneous expulsion or removal by traction. SUBJECTS AND METHODS We conducted a prospective, cross-sectional study involving patients that were admitted for induction of labour with unfavourable cervix, that is, a Bishop11 score < 4 between January 1999 and June 2001. They were all Negroids. The Bishop score was determined just before cervical ripening. Exclusion criteria included absence of fetal membranes, cervical infection and antepartum hemorrhage. Statistical test where necessary was by student's t test. P value of less than 0.05 was considered statistically significant. The Procedure The vaginal portion of the cervix was exposed with a sterile speculum and cleansed with the antiseptic chloroxynelol (Dettol®). Under direct vision, a size 16–20 Foley catheter with balloon capacity of 30–50mls was inserted through the external cervical os and the balloon inflated above the internal os with 50mls of sterile water. The distal end of the catheter was pulled down such that the balloon fitted against the internal os. This distal end was folded and taped to the inner thigh of the patient to prevent the catheter from dangling in-between the thighs, as she was allowed unrestricted activity. Each patient was placed on prophylactic antibiotic (Ampiclox). The time of insertion of catheter was noted and the time when the catheter fell off spontaneously or by traction was also noted with the new score. Maternal and fetal well being was monitored meticulously. Induction of labour was carried out by artificial rupture of the membranes and/or oxytocin infusion. Obstetric interventions such as instrumental delivery or caesarean section were left to the discretion of the consultant in charge of the patient. RESULTS During the period, 85 patients had extra-amniotic catheter balloon placement for cervical ripening preparatory for induction of labour. Twenty eight of the patients were primigravidae (33%) while the remaining were multiparous. The gestational age was 37 weeks or more in 51 patients, 28–36 weeks in 27 patients and 20–27 weeks in the remaining 7 patients. There were 19, 6 and 3 primigravidae in the three groups respectively. The indication for induction of labour was hypertensive disease in pregnancy in 36 (42%) patients, post-term pregnancy in 29 (34%) patients and intrauterine fetal death (IUFD) in 17 (20%) cases. The average Bishop score before insertion was 2.8 and average score after catheter expulsion was 9.6. The duration of catheter in the cervix is as shown in Table 1. Table 2 shows the relationship between gestational age and the duration of catheter in the cervical canal before expulsion. Spontaneous labour followed balloon expulsion in 34 (40%) patients, and in 51 (60%) patients oxytocin was required for labour induction and/or augmentation of weak contractions. Vaginal delivery was achieved in 77 (91%) of the women while there was recourse to caesarean section either because of failure to progress or fetal distress in 8 (9%) cases. There were 3 cases of postpartum hemorrhage amongst the study group and two febrile maternal conditions that responded to antimalarials. There was no maternal death. DISCUSSION After the catheter balloon is inflated, a variable time period is allowed for spontaneous expulsion, adequate ripening or the establishment of labour depending on the outcome measure used by the authors. Whereas in some studies the balloon was removed after 8 to 15 hours12-14 but re-inserted if cervical score criteria were not met15,16, others waited until the catheter was expelled or removed by pulling.17-19 Some workers would remove the catheter after 72 hours if ripening had not occurred and re-insert it after one week.20 One study reported using another method of cervical ripening if the balloon fails.21 To avoid unnecessary vaginal examinations with its attendant risks, the main outcome measure in this work was the expulsion of the intact balloon either spontaneously or by traction. Expulsion of the catheter with an intact balloon invariably meant a favourable cervix, which was confirmed by a high Bishop score at the post-expulsion assessment. From our results, only 33 (39%) patients expelled the balloon within 12 hours. This increased to 72% within 24 hours, 88% within 48 hours and 95% within 72 hours. In effect, most women would have expelled the balloon (favourable cervix) within 72 hours of insertion. Some workers17 reported expulsion of Foley catheter within 24 hours in over 90% of their cases, and another study claimed it was rare not to expel the balloon within 24 hours.22 The latter study, however, combined the cervical balloon with saline instillation and this could have contributed to the high rate of balloon expulsion within 24 hours. The expulsion of the balloon in only 72% of our patients within 24 hours could also be explained by the fact that as much as 40% of the pregnancies in this series were pre-term compared to 9% in the study by Sherman and colleagues22, while other reported studies were limited to term pregnancies only. In our study, the average duration of catheter stay when the gestational age was 20–27 weeks was 44.8 hours, which was significantly longer than 19.6 hours obtained when pregnancy was 37 weeks or more (p < 0.05). Therefore, gestational age or uterine size appears to be an important factor when the Foley catheter is used to ripen the cervix for induction of labour. It could be argued that in some cases even though the balloon had not been expelled, there could still be changes in the cervical score. However, one needed to perform a digital examination to confirm such changes. In the event that the cervix remained unfavorable after the examination, some workers had resorted to various methods to achieve the ripening15,16,20,21, increasing the theoretical risk of complications. Herein lies the advantage of using the expulsion of the intact balloon as the main outcome measure. Indication for the induction of labour is important in patient management. Depending on the urgency of delivery, some authors have advised that practitioners should always await favourable cervical scores.23 All the four cases in this series that expelled the balloon after 72 hours were of gestational age 20–27 weeks. Incidentally, all the four had intrauterine fetal death (IUFD) as indication for induction of labour and there was, therefore, no urgency for delivery. They eventually had vaginal delivery without any febrile morbidity. The most important concern with leaving the catheter more than 24 hours is that of sepsis. The findings of our study, however, did not support this concern. Other studies also did not find febrile morbidity when catheter was left for more than 24 hours even in the presence of IUFD.10,20 We postulate that this is because the procedure was performed under aseptic conditions. Also in our study, repeat digital pelvic examinations were done only after balloon expulsion in addition to placing the patients on prophylactic broad spectrum antibiotics. Even though there are now reports of catheter being used in the presence of membranes rupture24, all the patients in our series had intact membranes. Some workers17,19 have reported side effects like fluid leakage probably from secretions from the cervical canal that may track down through the “eye” of the catheter. We did not record such leakage. If the distal end of the catheter is folded or a loose knot made, it might obviate or reduce such leakage. Our findings that 91% of the patients had vaginal delivery following cervical ripening and induction of labour is rewarding and significant in a community that is generally averse to surgery. In conclusion, the balloon of the Foley catheter can safely remain in the extra-amniotic space for more than 24 hours if the cervix is not favourable, provided the membranes are intact and there is clinical evidence of satisfactory feto-maternal well being. Most would be expelled within 72 hours. The maximum duration of catheter placement in our series was five days and the gestational age at which the catheter was used for cervical ripening played a significant role. ACKNOWLEDGEMENT We are indebted to Prof. D. P. Ghatak, FRCOG, for his advice, and Mrs. Elizabeth Momo for secretarial work. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02040t1.jpg] [rh02040t2.jpg] |
| |||||||||

{kind=link}
{kind=link}