 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 103–111 Perceptions of and Attitudes towards Male Infertility in Northern Botswana: Some Implications for Family Planning and AIDS Prevention Policies Rebecca L Upton1 1 University of Michigan,
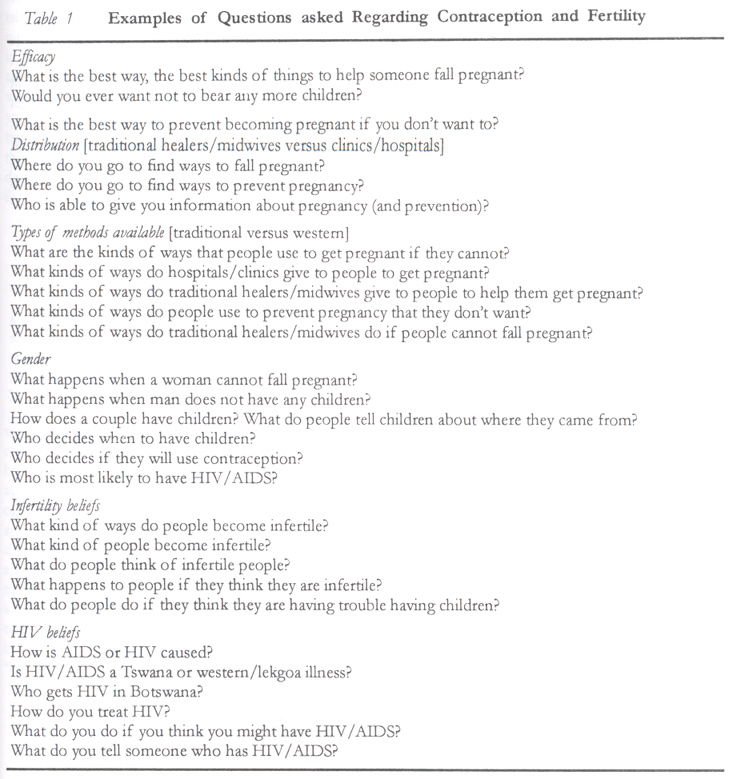
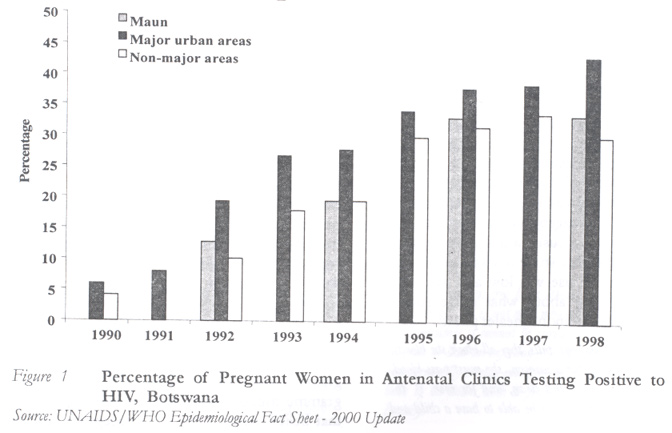
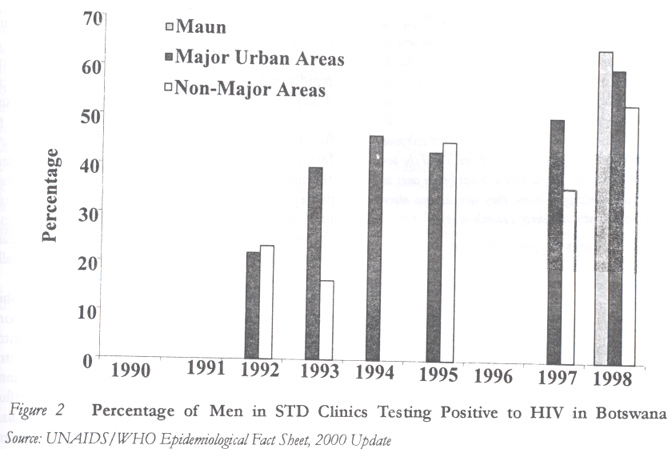
Ann Arbor. Code Number: rh02041 ABSTRACT This paper discusses the perceptions of male infertility in northern Botswana and their implications for efficacious family planning and AIDS prevention programmes in the country. HIV rates are rapidly increasing in northern Botswana and it is estimated that nearly 30% of the population are infected. A significant factor in these increases is the perception that infertility is caused by the use of contraceptives. Male infertility in particular is understood as a result of female contraceptive use and is highly stigmatised. In an area with such high HIV rates, these perceptions directly contribute to the lack of efficacious family planning and HIV prevention programmes in the country. (Afr J Reprod Health 2002; 6[3]: 103–111) RÉSUMÉ Perceptions et attitudes envers la stérilité masculine au nord du Botswana: quelques implications pour la planification familiale et pour les politiques de la prévention du SIDA. Cet article étudie les perceptions de la stérilité masculine au nord du Botswana et leurs implications pour une planification familiale efficace et pour les programmes de la prévention du SIDA dans le pays. Les taux du VIH augument rapidement au nord du Botswana et on estime que près de 30% de la population sont infectées. A l'égard de ces augmentations, un facteur très important demeure la perception qui consiste à croire que la stérilité est causée par l'emploi des contraceptifs. La stérilité masculine en particutier est perçue comme une conséquence de l'emploi des contraceptifs par les femmes et ceci est bien stigmatisé. Dans une région où il y a des taux élevés du VIH, ces perceptions contribuent directement au manque d'une planification familiale efficace et des programmes de la prévention du VIH dans le pays. (Rev Afr Santé Reprod 2002; 6[3]: 103–111) KEY WORDS: Gender, infertility, Southern Africa INTRODUCTION Many demographic studies in southern Africa focus on levels and trends in fertility among married women or all women in childbearing cohorts (15–49 years).1 The behaviours of individuals who are unmarried, and more importantly infertile, are rarely considered in such studies despite increasing attention to concomitant issues of sexually transmitted diseases and HIV/AIDS in this region.2 This study examines an even more shrouded aspect of infertility in the southern African context, the attitudes towards, perceptions of, and responses to male infertility. Tswana culture has long emphasised the value of childbearing for the successful attainment of personhood and identity for both men and women.3 Population and official government policies have focused on the high rate of unmarried fertility with little recognition of the cultural factors that influence that necessity. While Botswana has one of the world's lowest population densities, it is nevertheless high compared to the fragile resource base. Most BaTswana are concentrated in the east of the country and the rate of population growth is approximately 3.5%. Botswana, in addition to the growth rate, has a total fertility rate that, although decreasing, remains high at 4.3 births per woman. A recent review of the Maternal and Child Health Programme stated that the country had one of the highest levels of contraceptive use in sub-Saharan Africa, about 32% in 1991, but the increasing rates of HIV raise questions about this level. Resources to address these increasing rates and programmes geared towards HIV prevention have become more prevalent. The number of persons infected with HIV was estimated to be about 92,000 in 1993 (out of a population of 1.3 million), or one in seven of the sexually active population. Between 1993 and 1995 the HIV seroprevalence rate among antenatal women rose from 22.5% to 32.5% and these figures are of course based on those women who do actually attend clinics (only an estimated 25% of women).4,5 More recent newspaper headlines that were repeated in the field site village orally proclaimed a ratio of one in three of the sexually active population. Upon hearing this information responses varied. For many, AIDS is considered a lekgoa (white person) disease and not one that is considered to affect BaTswana. Thus, despite the ever-increasing incidence and prevalence of HIV/AIDS in Botswana6, few Tswana in the northern district believed that it was a significant illness or, more importantly, one that affected or was carried by men. RESEARCH SETTTING, DATA AND METHODOLOGY The Maun Community This paper is based on data gathered during 15 months of field work in Botswana during 1996 and 1997, with follow-up study conducted in 1998 and 2001. The field work was concentrated in a village in the north west district of Ngamiland, primarily in and around the village of Maun. Maun is situated on the Thamalakane River, in-between the Delta region to the north and the Kgalagadi Desert to the south. Maun is the present district administrative headquarters for Ngamiland, the historic home of the BaTawana people. While Ngamiland today has an ethnically diverse population, the term BaTawana is also used to refer collectively to all inhabitants of Ngamiland. Most villagers maintain flocks of goats and cattle but crops remain largely dependent upon the seasonal floods and rain. Economically, the local community has depended on the income from male migrant labour although changes in this system have begun to affect the lives of both men and women. Fewer men send remittances and women are forced to seek alternative means of support, even leaving the community to seek employment or education in the south. Some villagers have begun to seek employment in the rapidly growing tourism industry in Ngamiland although this too is largely seasonal employment, and overall the community was economically depressed at the time of this research. Data and Methodology The findings presented in this article are drawn from a larger project on the impact of infertility on the social life and status of women in Botswana. A survey of 307 individuals (including clinicians, traditional healers and midwives) was conducted in several wards (kin-based neighbourhoods) with more in-depth interviews and life course history and reproductive histories gathered for approximately 45 women within that sample. These more in-depth studies comprised the majority of field work, as intensive ethnographic knowledge was gleaned from daily participant observation over the research period. For this paper, research and interviews with men in the community on the topic of infertility and health were utilised. Both SeTswana and English are official languages in the country and interviews were often conducted with the assistance of several local interpreters in order to capture the complex and sensitive aspects of language and meaning surrounding fertility, family and health issues. In addition to these interviews, the author lived in the community, participated in everyday life and village activities and observed daily interactions. She recorded the observations daily and discussed when and why individuals spoke about issues with respect to family and fertility repeatedly in order to gain a more holistic perspective of such demographic issues. Questions concerning use of contraception, traditional methods of contraception and fertility enhancements were asked of each individual who was formally or informally interviewed and provided the basis for focus group discussions. Sample questions drawn from this questionnaire are included in Table 1. Answers and discussions based on these questions formed the basis for further research into the question as to what happens when individuals find they cannot reproduce. In turn, research questions connected to infertility often centered on the increasing rates of STD and how these two health related phenomena were affected by contraceptive methods. FINDINGS The population in Maun has high levels of knowledge about fertility control and contraception. Many individuals, for example, spoke about the ubiquitous HIV/AIDS prevention billboards throughout the country admonishing one to “follow the ABCs of HIV prevention: Abstain, Be Faithful and Condomise”, in addition to the constant advertisements and health warnings on the radio about HIV infection. The AIDS and STD prevention office of the Ministry of Health has launched a particularly large campaign directed towards youth in order to prevent unwanted pregnancy that also stresses the need for HIV and STD prevention. Despite this knowledge, however, the incidence and prevalence rates of sexually transmitted diseases in the region are continuing to increase (Figures 1 and 2), and in the Maun region in particular. In addition, physiological and cultural connections between STDs and fertility remain largely unconsidered. These connections become evident in the data as expressed through ethnographic research and are presented in conjunction with the profile of rates of STDs in Maun in contrast to other parts of the country. Characteristics of the Survey Population — Migration The Maun community has long been impacted by emigration by men to the southern parts of the country and the southern African region.7,8 For many women, this migration has been of advantage in developing culturally appropriate means of mediating fertility status. For example, Iris, a 23-year-old woman in Maun, describes her pregnancy:
Iris' explanation was one that I heard on several occasions where apparent infertility, and particularly male infertility, was explained as a result of female blood. It may be that Iris was able to get pregnant through sexual intercourse with another man but she explained it as an unusually long pregnancy in order to afford Kutlo fertile status. This strategy is culturally compatible with constructions of gender where women are believed to be the primary contributors to infertility. As Rra Kwena put it:
If a man feels that he may have been “bitten” by a woman, where she might have an illness of the blood (primarily due to the transgression of some taboos) it is not uncommon that he will sleep with a young woman or girl in the effort to rid himself of this illness. As many individuals travel frequently throughout the country, these actions often have consequences that affect the increasing HIV rate. One 45-year-old man told me repeatedly that he was afraid that he had been “bitten” since he was chronically ill. He drives trucks through the country to Zimbabwe and South Africa and within Botswana as well. He argued that it is only through intercourse with a younger woman (or girl) that a man could be,
This man's strategy, referred to by many as the “virgin cleansing myth”, echoes the earlier belief that it is indeed older Tswana women who are thought to be both infertile and carry HIV. In addition, it points to the necessity for policymakers on family planning and AIDS prevention to look carefully at the cultural construction of contraceptives themselves. Characteristics of Family Planning and Contraception At one point during the research period, I gave a talk on how HIV was affecting the Maun community and Botswana in general. Many Tswana were in the audience and at one point one man stood up and asked, “Why do you (health officials, clinical workers, etc) keep telling us to use condoms when you know they make us sick?” Upon further investigation, it was clear that many male members of the audience were particularly vehement in their declaration that condoms are indeed making them ill. A 37-year-old man told me:
Many Tswana individuals, both men and women, actively resist the use of western contraceptives. As I travelled round the country, billboards, literature and radio announcements talk about the importance of “condomising” to protect oneself and to prevent unplanned pregnancy among young people.10 Given the high rate of media exposure and general knowledge in the country about western contraception, one would expect that a higher rate of use would accompany this knowledge. Yet in this study it was clear that continual contraceptive use was low and was directly linked to ideologies about what made someone “healthy”. As one traditional healer put it:
Injections such as Depo Provera are also thought to be harmful to one's health in this way and were routinely described as being detrimental to one's ability to be a “healthy” individual in the society. Even non-western contraceptives and beliefs about the abilities of certain foods or beverages to affect fertility were pervasive. Hot, caffeinated tea, for instance, is seen to be particularly efficacious in limiting one's fertility and has the potential to cause infertility in women who have not yet giving birth to children. Many traditional healers11 and midwives talked about how they would not tell someone to seek for contraception, that they were suspicious of the western clinical hospital and the effects that their medications could have on the overall “health” of the community, above and beyond the individual. Certain Tswana members of the community who were employed at the clinics and hospitals actively worked against the clinical policy in persuading individuals not to accept contraception. A 22-year-old mother of four thus said:
These data echo others who have found in the southern African region13 that what individuals are concerned with is problems of infertility not the prevention of fertility itself, thus causing dissonance between cultural perceptions, attitudes, acceptance and use of fertility controls. With these data, it is clear that further investigation into how fertility is understood as an essential aspect to personhood and general (in addition to reproductive) health should be central to any efficacious HIV/AIDS prevention or family planning programme. For example, if an HIV prevention programme focuses solely on condom use it is clear that beliefs about barrier contraceptives will continue to be unsuccessful. While it is difficult to suggest alternatives to current policies and education, research into new methods of prevention such as vaginal microbicides or other non-barrier methods seems to bear some attention. Characteristics of HIV/AIDS The power of blood and the links between contraception and health are evident in discussions of HIV/AIDS in Botswana. Awareness is high (there is a National AIDS Control Programme, NACP, established in 1989 with an AIDS prevention policy) due to the fact that people discuss AIDS, and enormous billboards are erected on major thruways/truck routes in the country. Yet many of the people interviewed argued that it is simply a `radio disease', an illness that one hears about on the radio but has never actually encountered first hand. In addition, many older men who were involved in this research claimed that it is in fact older Tswana women who carry the disease. HIV/AIDS and the illnesses associated with the use of contraception are often assumed to be a result of women. When men spoke about being “bitten”, for example, and of having weakened blood as a result of contraceptive use or even HIV from women, cures centered on the necessity to have sexual intercourse with young girls, what is often referred to as the “virgin cleansing myth”. Here, even if a woman attempts to protect herself against illness and unwanted pregnancies, the gender inequalities at the sociocultural level prevail as ironically, the very `cure' for men leads to infection for women. Again, Rra Kwena discussed how,
In this case, data suggest that blood, and in particular female blood, is believed to be directly responsible for male reproductive health. Culturally and theoretically, male infertility appears to be a direct result of possible symptoms of female illness such as HIV infection. Yet as Figures 1 and 2 suggest, practically and physiologically, male infertility can be seen as both a product of sexually transmitted disease as concomitant with lowered use of contraception and condoms in particular. Characteristics of Male Infertility The power of blood and contraception in this research is directly linked to female reproductive health and ultimately the fear and stigma associated with infertility. Little or no mention was made of male infertility directly apart from the perception that any illness experienced by men is a direct result of female reproductive illness. One man alleged vehemently:
Gossip and community knowledge about infertility and the inability of couples to reproduce abounds.14 While much is directed at women, many male respondents voiced concern that women would then redirect that status towards other women and even to male partners. As one man suggested:
While the data in Charts 1 and 2 are limited in that they only capture individuals who present at antenatal or STD clinics, they do suggest the rapidly increasing rates of HIV infection in the country. At present, as this ethnographic research has begun to demonstrate, much more attention to the connections between perceptions of HIV/AIDS and infertility (particularly as related to male infertility) are necessary. Male infertility remained a particularly sensitive topic in this research as many men were hesitant and even initially reluctant to discuss the topic. While some of that reluctance stems from the interview situation, it was clear upon further ethnographic investigation that male infertility remains a much understudied and undiscussed phenomena in both academic literature as well as in everyday life in Botswana.
As these findings suggest, men are literally and figuratively moving on. If they feel ill, they are able to appropriate other cultural narratives about illness and reframe both their diagnosis and treatment as causally linked to female reproductive health. Ironically, however, migration and multiple partnership allow women to draw upon similar narratives in order to reframe their own status as fertile individuals. While perhaps not a statistically significant variable, infertility, particularly male infertility, is a salient and significant social variable linked to rising STD rates in the country. DISCUSSION The social and economic history of northern Botswana is particularly salient to the contemporary understanding of male infertility and the connections with increasing rates of sexually transmitted diseases. The normative pattern of migration is intricately connected to ideologies of health and culturally supported ideas of gender and childbearing. Migration, cultural logics about the significance of reproduction, gender, power, cultural perception of family planning and HIV all contribute to contemporary attitudes and perceptions of male infertility in northern Botswana. The use of contraception by individuals, both male and female, is understood to be a significant factor in the cause of infertility. Despite the high level knowledge of both traditional and western methods of contraception, only few individuals in this study readily acknowledged that western contraception is at all efficacious in preventing infertility. While certainly the intent (from a western clinical perspective) is to prevent pregnancy and in addition prevent the spread of STDs (with condoms) and even prevent infertility, beliefs about the significance of fertility and reproduction prior to marriage remain particularly strong and directly intervene with these contraceptive programmes. Statistics suggest that STDs and HIV are rising rapidly in Maun and Botswana as a whole. Yet few, if any, studies on male infertility in this region exist at all. This study demonstrates how difficult it is to first locate male individuals who do experience infertility and, secondly, how gendered understandings of health and fertility influence those perceptions. Evidence that male infertility and cultural understandings of blood, contraception and “health” are linked should be explored more fully in future research in order to provide more culturally sensitive and, above all, efficacious programmes. While this study was grounded in ethnographic research in northern Botswana, it can be more broadly applicable and generalised to the country itself. As individuals migrate within the country frequently, this study provides great insight into Tswana beliefs and attitudes towards fertility influencing factors and male infertility in particular. This study demonstrates how perceptions of infertility can be mediated through individual strategies, both male and female, and yet underscores the importance of gender for reproductive health accessibility in Botswana. The study highlights the value of ethnographic and qualitative research for policy and family planning/HIV prevention programmes as it provides more in-depth knowledge on factors that influence male reproductive health and concerns. Men have not been culturally construed as infertile and this observation has potentially far reaching effects for AIDS prevention. Infertility and AIDS are often described as female illnesses; they are remedied through intercourse with multiple sexual partners, are considered to be caused in many ways by contraception, and are described generally as a “disagreement of blood”. Exploring these understandings and examining traditionally non-demographically significant variables and gender inequalities embedded within cultural perceptions of health and illness, we can begin to suggest potentially more efficacious family planning and HIV/AIDS prevention policies. ACKNOWLEDGEMENTS The author is indebted to the entire Maun community, particularly to the various clinicians, health officials, traditional healers and midwives who have provided invaluable insights. The government of Botswana and the Demography Unit at the University of Botswana have all been particularly supportive. Special thanks are due to the J. William Fulbright and Andrew Mellon Foundations for financial support of this research and to Nathanael T. Lauster, Autumn J. Kelly, Dr Thomas Fricke and Dr Marcia Inhorn for assistance, advice and suggestions. The author is also indebted to the anonymous reviewers for their valuable comments and suggestions on an earlier version. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02041f2.jpg] [rh02041f1.jpg] [rh02041t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}