 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 6, No. 3, December, 2002 pp. 112-116 Leucocyte Counts in Pregnant Nigerian Women with Sickle Cell Trait Awodu OA1, Enosolease ME1, Ubaru AG1 and Famodu AA1 1Department of Heamatology,
School of Medicine, College of Medical Sciences University of Benin, Benin
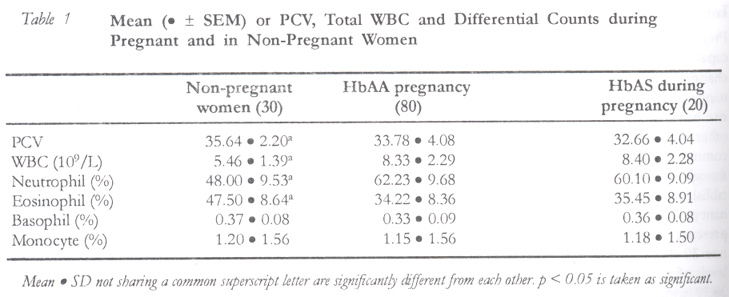
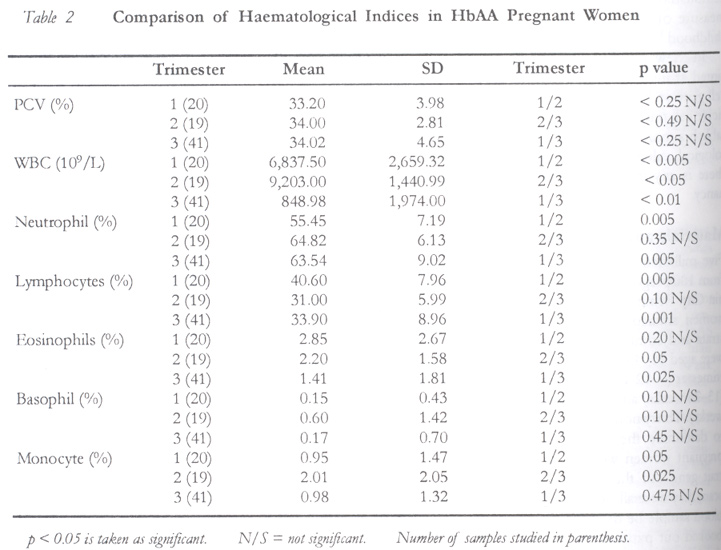
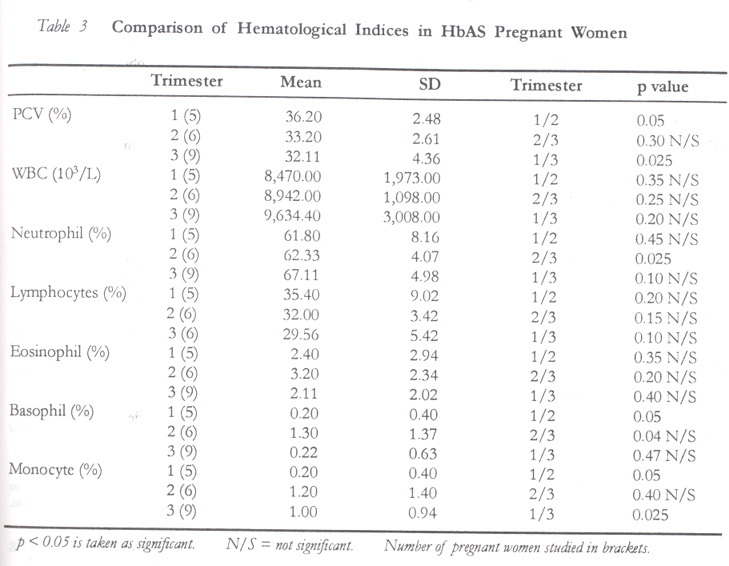
City, Nigeria. ABSTRACT White blood count (WBC) with differential counts and packed cell volume (PCV) were studied in 100 pregnant and 30 non-pregnant control women aged 18–45 years. Eighty of the pregnant women were homozygous HbAA and 20 heterozygous HbAS. The non-pregnant women's PCV, lymphocyte and eosinophils counts were significantly higher (p < 0.005) while their leucocytes neutrophil counts were significantly lower (p < 0.005) compared with HbAA and HbAS pregnant women. However, HbAS pregnant women had higher leucocyte, lymphocyte and eosinophil counts compared with HbAA, but these were not significant. There were no variations in basophil and monocyte counts. HbAA pregnant women had no change in PCV but significant changes occured in leucocyte and neurophil counts with increase in the second trimester with decreasing lymphocyte and eosinophil counts in the second and third trimesters. However, HbAS pregnant women had significant increase in PCV in their first trimester, leucocyte and neutrophil counts in their third trimester but no variation in lymphocyte, eosinophil and basophil and monocyte counts. The increased leucocyte and neutrophil counts in the second trimester in HbAA and third trimester in HbAS may be due to genetic factor and/or oestrogen secretion reaching production peak at different periods of pregnancy. The relative increase in these haematological indices in HbAS women may be a protective mechanism against infection during pregnancy. (Afr J Reprod Health 2002; 6[3]: 112–116) RÉSUMÉ Numérations leucocytaires chez les femmes nigérianes enceintes qui ont des traits drépanocytaires. Nous avons étudié le nombre de globules blancs et le formulaire leucocytaire et l'hématocrite chez 100 femmes enceintes ainsi que chez 30 femmes témoins âgées de 18–45 ans, qui n'étaient pas enceintes. 80 femmes parmi les femmes enceintes étaient des homozygotes de type HbAA et 20 étaient des hétérozygotes, de type HbAs. Le formulaire leucocytaire, la numération lymphocytaire et la numération des éosinophiles étaient appréciablement élevés alors que leur numération leucocytaire des neutrophiles était appréciablement peu élevée (p 0, 005) comparée à HbAA et HbAS chez les femmes enceintes. Toutefois, les femmes enceintes de la catégorie HbAS avaient des numérations leucocytaires, lymphocytaires et des neutrophiles plus élevés par rapport à HbAA, mais ceux-ci n'étaient pas significatifs. Il n'y avait pas de variations quant aux numérations des basophiles et aux numérations monocytaires. Il n'y avait pas de modification dans le formulaire leucocytaire chez les femmes enceintes de type HbAA, mais il y a eu des modifications assez importantes au niveau des numérations leucocytaires et au niveau de taux des polynucléaires neutrophiles au fur et à mesure que le second trimestre augmentait que les numérations leucocytaires et des éosinophiles baissaient au cours de second et du troisième semestres. Néanmoins, il y a eu des hausses importantes chez les femmes enceintes de la catégorie HbAS par rapport au formulaire leucocytaire dans leur premier semestre et dans les numérations leucocytaires et des neutrophiles dans leur troisième semestre. Il n'y avait pas de variation dans les numérations lymphocytaires, dans les éosinophiles et les numérations des basophiles et des monocytes. La hausse des numérations leucocytaires et des neutrophiles dans le second trimestre chez les HbAA, et dans le troisième trimestre chez les HbAS peut être attribuée au facteur génétique et/ou à la sécrétion de l'oestrogène qui atteint le sommet de la production à des étapes différentes de la grossesse. La hausse relative de ces indicateurs hématologiques chez les femmes de la catégorie HbAS peut servir de mécanisme protecteur contre l'infection pendant la grossesse. (Rev Afr Santé Reprod 2001; 5[1]: 112–116) KEY WORDS: Haematological indices, pregnancy, sickle cell INTRODUCTION Pregnancy is one of the physiological conditions capable of causing remarkable and dramatic changes in haematological variables. During pregnancy there is a rise in white blood cells and this rise has been attributed to neutrophilia.1-4 In another report, neutropenia have been found to be common among non-pregnant Africans.5-7 Although several studies have been carried out to establish normal haematological values during pregnancy, few studies have taken cognizance of the presence of sickle cell traits (HbAS), which constitute 30–40% among black Africans.8 The relative levels of percentage haemoglobin S in the HbAS is 38.59 with a range of 32.81–48%.9 It has been demonstrated that sickle cell trait contributes a measure of relative protection against malaria in childhood.8 In view of these observations, the study is aimed at investigating the effect, if any, of sickle cell gene on haematological parameters in pregnant sickle cell traits in black Africans, and to further establish a more reliable and realistic normal haemotological values for pregnant Africans and see if there is any influence of Hbs gene during pregnancy. MATERIALS AND METHODS Five milliliters of venous blood each was drawn from 100 pregnant Nigerian women residing in Benin City. Benin City is a cosmopolitan city and the women studied were representative of all social strata and ethnic groups in Nigeria. The subjects were aged 16–45 years, 25 of them were in the first trimester (0–12 weeks), 25 in the second trimester (13–26 weeks) and 50 in the third trimester (27–41 weeks). Thirty non-pregnant women were also bled to determine the normal values. Twenty of the pregnant women were homozygous for sickle cell trait gene. All the women had single fetuses by scan, they were all fit and well and agreed that their blood sample be used for the study. They were all booked out patients for routine antenatal care at the University of Benin Teaching Hospital and they were on routine folic acid (5mg) daily, fersolate 200mg tds and pyrimethamine (25mg) weekly. Blood samples were taken from the antecubital fossa vein by venepuncture in the morning from the pregnant and non-pregnant women into sequestrene tubes with minimum stasis. Haematological values were determined within standard two hours of collecting the sample. The PCV was estimated using the micro haematocrit method.10 The sickle cell status was also established by standard cellulose acetate electrophoresis as previously described.10 STATISTICAL ANALYSIS Statistical significance of the mean ± SD was tested using student's t-test for paired and unpaired data. For all tests, significance was established to have p < 0.05. RESULTS Table 1 shows the mean SD of PCV, total WBC and differential counts in pregnant women. The non-pregnant women had a higher PCV, lymphocytes and eosinophil count but lower total WBC and neutrophil counts compared with the HbAA and HbAS pregnant women. There were normal differences in basophil and monocyte counts between the groups. The table also shows that pregnant women with genotype AA had slightly higher levels of PCV and neutrophils while the lymphocyte counts were higher in the pregnant women. There were no significant differences in all the haematological parameters measured between pregnant women with genotype AA and AS, although AS pregnant women had higher levels than HbAA. Table 2 shows the comparison of haematological indices in HbAA pregnant women in different trimesters. There were no significant differences in PCV. Total WBC were increased in the second and third trimesters and there were significant differences between trimesters. Neutrophil counts were increased in the second trimester and significant differences were observed between first/second and first/third trimester. Lymphocytes decreased after the first trimester with significant differences between first/second and first/third trimesters. Eosinophil counts decreased during the third trimester with significant differences between first/third trimesters. No variation in basophil counts during pregnancy while monocyte counts varied between trimesters with significant difference between the second/third trimesters. Table 3 shows the comparison of haematological indices in pregnant women with HbAS. PCV decreased from first trimester with significant differences between first and third trimesters total. WBC count increased while lymphocytes decreased throughout pregnancy but no significant differences between the trimesters. Neutrophils showed some variation with significant differences between the second and third trimesters, but no significant change in eosinophil counts during pregnancy. DISCUSSION There is abundant evidence that haematological values vary considerably during pregnancy.1-5 These changes may be due to several factors, which include the placental hormones secreted in pregnancy, increased erythropoetin production5 and increase plasma volume.11 This study shows clearly that in Benin City there is significant fall in PCV during pregnancy (though within normal range) despite iron supplementation throughout the period of pregnancy. It has been reported that iron therapy improves HCT levels in pregnant Nigerian women.12 There was no difference in the PCV of pregnant women with sickle cell trait and those with homozygous HbAA. This finding, therefore, confirms the belief in medical circles that patients with sickle cell traits are not worse off when pregnant. The data obtained in this study, though few in number, further supports our earlier suggestion that poor nutritional status and not the effect of sickle cell trait is responsible for lower PCV in Nigerian pregnant women.13 Leucocytosis due to neutrophilia in pregnancy is known14, and this report shows that it occurs in pregnant Nigerian women irrespective of their genotype. We noticed an increase in total leucocytes particularly neutrophil count in the second trimester in subjects with genotype AA and in the third trimester in subjects with genotype AS. Possible explanation to the differences in the leucocyte counts of the genotype AA and AS may be that while women with genotype AA reached their highest oestrogen secretion peak at about the second trimester, the pregnant women with genotype AS reached their highest oestrogen secretion peak at the third trimester. The increased leucocyte count and neutrophil counts in women with genotype AS may be another protective measure against infection during pregnancy and could as well be due to a genetic factor. Various reasons have been attributed to the increase in leucocyte count in pregnancy, which include elevated oestrogen secretion, raised plasma cortisol and increasing parity.14-16 We found that the lymphocyte count was lower in pregnancy regardless of the genotype, while women with genotype AA had the lowest count in the second trimester with a significant decline between the first and third trimesters. Eosinophil count dropped significantly during pregnancy, which is similar to previous reports5,17,18, while basophil and monocyte counts did not show variation in pregnancy. We conclude that pregnancy is characterised by a significant fall in PCV, lymphocytes and eosinophils, and the significant leucocytosis is due to neutrophilia. On the other hand, these changes may be due to the increase in subclinical infection. However, more work has to be done to assess the level of subclinical infections in this category of women. The influence of good and balanced diet cannot be over-emphasised, as this is capable of improving haematological indices, and the expectant mothers should be encouraged to improve their diet. REFERENCES
Copyright 2002 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh02042t2.jpg] [rh02042t3.jpg] [rh02042t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}