 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 1, April, 2003 pp. 12-16 Poor Acceptance Rate for Semen Donors to a Private Cryobank in Nigeria Akinrinola OA1, Melie NA1 and Ajayi RA1 1The Assisted Conception
Unit, The Bridge Clinic Limited, P. O. Box 70294, Victoria Island, Lagos, Nigeria.
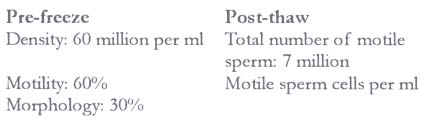
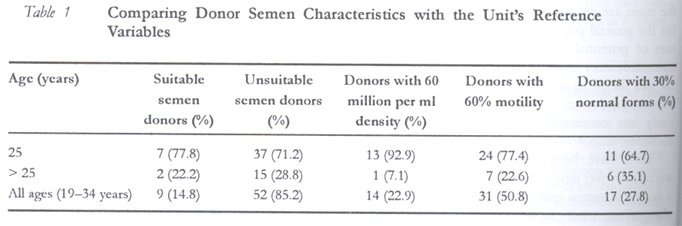
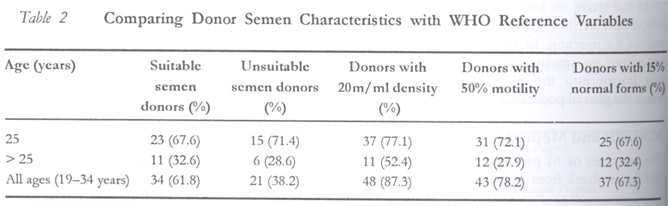
E-mail: bridge@om.metrong.com Website: www.thebridgeclinic.com Code Number: rh03003 ABSTRACT A retrospective analysis of sixty one prospective donors who visited the cryobank in person from August 1999 to December 2001 was done. The study evaluated the acceptance rate of prospective semen donors and semen characteristics in order to assess the fertility potential of the supposedly normal population of young men. The outcome of the various screening processes – history taking, infection screening, blood grouping and Hb genotype assessment, semen analyses (pre-freeze and post-thaw), and post-quarantine (six months after production of last sample) infection – was analysed. Out of the 61 enquiries, 9 (14.8%) donors were recruited, 7 (77.8%) of whom were less than 25 years old. Fourteen (22.9%) donors had sperm concentrations greater than 60 ' 106ml, 31 (50.8%) had motility greater than 60% and 17 (27.8%) had normal forms greater than 30%. Six (9.8%) of the donors were unable to masturbate and thus were disqualified, while only one donor (6.1%) failed to show up for a re-test after the completion of the quarantine period. Twenty one (38.2%) donors had low semen values based on the WHO reference value. We conclude that a high proportion of prospective semen donors may have sub-optimal semen parameters, and that using strict criteria, poor acceptance rates for donors is observed in a semen donation programme. (Afr J Reprod Health 2003; 7[1]: 12–16) RÉSUMÉ Mauvais taux d'acceptation des donneurs de la semence à une cryobanque privée au Nigéria. Une analyse retrospective a été faite de soixante-un donneurs prospectifs qui ont personnellement visité la cryobanque d'août au décembre 2001. L'étude a évalué le taux d'acceptation des donneurs prospectifs de semence ainsi que des caractéristiques de la semence afin d'évaluer le potentiel de fécondité de la soi-disant population des hommes. Les résultats des divers procès du dépistage – interrogations, dépistage de l'injection, évaluation du groupe sanguin et du génotype Hb, analyses de semence (pre-congelé, post-décongelé) et l`infection post-quarantaine (six mois après la production du dernier échantillon) ont été analysés. Soixante-et-un enquêtes, 9 (14,8%) donneurs ont été recrutés dont 7 (77,8%) avaient moins de 25 ans. Quartorze (22,9%) donneurs avaient une concentration de semence supérieure à 60 x 106ml. Trente-et-un (50,8%) avaient une motilité supérieures à 60% et 17 (22,8%) avaient de formes normales supérieures à 30%. Six (9,8%) donneurs ne pouvaient pas masturber et ont été, donc, rendu incapables de participer, alors qu'un donneur (6,1%) ne s'était pas présenté our un re-test à la fin de la période de quarantaine. Vingt-et-un (38,2%) donneurs avaient des indices bas de semence selon les indices de reference d'OMS. Comme conclusion, nous affirmons qu'une proportion élevée des donneurs prospectifs de semence auraient des paramètres sub-optimum de semence et qu'à l'aide de critères stricts, on constate des faibles taux d'acceptation des donneurs dans un programme du don de remence. (Rev Afr Santé Reprod 2003; 7[1]: 12–16) KEY WORDS: Semen donors, cryobank, semen quality INTRODUCTION The use of donor semen is an integral part of most assisted conception programmes. Prior to the advent of intracytoplasmic sperm injection (ICSI) for the management of male factor infertility, demand for donor sperm was relatively high. However, ICSI has since revolutionised the treatment of male factor infertility and made it possible for men with even the most severe semen abnormalities to have genetically related offsprings — a more acceptable outcome. This is thought to have led to a decline in the number of requests for donor sperm in some countries.1 Although ICSI remains the best solution for male factor infertility, there is still a role for donor sperm. Some men may request the use of donor sperm following poor prognosis for surgical sperm collection (SSC), and others may do so after an unsuccessful SSC procedure. In addition, there may be cost considerations regarding ICSI. Sources of donors vary between countries but appear to be predominantly student populations,2 older or married men making up the rest. Donor recruitment criteria also differ, but in the main are set higher than the reference values for the general population. In addition, due to issues of potential infections especially human immunodeficiency virus (HIV), it has become unethical and illegal to use unquarantined semen from unscreened donors. This may account for the relatively low recruitment rates observed in some countries/units.3,4 There have been debates over semen quality among men over time. While some studies have shown a decline in semen quality,5-7 others showed an unchanged or even increased sperm count over time.8,9 In our study, we looked at the acceptance/rejection rates of donor applicants and analysed the reasons for rejection. In addition, particular focus was placed on semen characteristics in order to gain insight into the possible semen situation within the general population. MATERIALS AND METHODS The outcomes of 61 prospective donors who visited the cryobank from August 1999 to December 2001 were examined. Donors were recruited mainly from higher institutions of learning in the locality. After making enquiries, donors were selected based on their ability to produce semen samples whose parameters are above laboratory specified minimal limits. The age limits were 18–40 years. They were all given token pecuniary compensation.10 The amount of money given depended upon the stage of the recruitment process. However, once accepted, the donor was initially given a thousand and five hundred naira. This was later reviewed to two thousand naira per ejaculate within the study period. Payments were made in two instalments – half at each ejaculation – and the combined balance post-quarantine upon negative infection screening results. Clinical Assessment All donors were interviewed and thoroughly examined by a clinician prior to acceptance. The assessment covered basic personal data, current general health, past medical and surgical history, family history (including a detailed general history), occupational and social history, medical and illicit drug use, reproductive and sexual history.11,12 Screening for Fertility The semen samples were produced strictly by masturbation. Assessment of semen quality was based on the evaluation of several parameters including semen volume, sperm motility and sperm morphology in particular. Routine semen analysis was performed by at least two trained technicians (internal control) using phase contrast microscopy on wet preparation to determine percentage motility and normal forms manually. Sperm concentration was determined using improved Neubauer counting chamber after diluting the original sample 1:20 in distilled water. The result was compared to the reference variables of our cryobank. Only prospective semen donors, though with borderline assessment, were given a second chance to analyse their semen samples. Suitable semen samples were vapour frozen under sterile conditions and stored in liquid nitrogen at -196oC for post-thaw assessment the following day. Minimum Requirement (Table) Screening Test for Infection Successful donors at this stage were tested for infectious diseases, which included HIV 1 & 2 antibody, hepatitis B surface antigen, syphilis (RPR), ABO and Rh blood grouping as well as Hb genotype (only AA was accepted). Quarantining After a satisfactory screening exercise, all successful donors were recruited in our cryobank. The semen samples were quarantined for six months, prior to a re-test for infectious diseases such as HIV 1 & 2 antibody, hepatitis B surface antigen and syphilis (RPR) before the samples were released for use. RESULTS Table 1 shows the performance of donors based on the unit's pre-freeze variables (density 60 million per ml; motility 60% and morphology 30%). Nine (14.8%) donors were accepted, seven (77.8%) of which were less than 25 years old. Fourteen donors (22.9%) had sperm concentrations greater than 60 million per ml, 31 (50.8%) had sperm motility greater than 60% and 17 (27.8%) donors had sperm morphology greater than 30%. Table 2 shows the performance of donors based on the reference value of a normal semen assessment16 (density 20 million per ml; motility 50% and morphology 15%). Thirty four (61.8%) of the donors fell within the normal reference value, out of which twenty one (67.6%) were less than 25 years old. Twenty one (38.2%) donors fell below the normal reference value with 15 (71.4%) of them less than 25 years old. On the whole, six (9.8%) donors were unable to masturbate and were disqualified. Only one (1.6%) donor failed to show up for a re-test six months after the completion of the quarantine period. DISCUSSION For a successful semen donation programme, certain criteria are employed in donor recruitment. This would ensure as much as possible the supply of infection free, genetically wholesome and potent semen. The screening strategies involved would therefore result in exclusion of some prospective donors. The vast majority of semen donors in our cryobank are from higher institutions of learning. Payments were made to all applicants as compensation or for inconveniences but the amount paid was not high enough to be a main factor in donor recruitment.13 A United Kingdom sperm bank tried a total altruistic mode of recruitment. Only 38.8% of their needs were met and it resulted in a reduced pregnancy rate, as less rigid and strict criteria were used.12 Report from a study showed that most of the semen donor applicants were usually unsuitable after completing the screening exercise.4 Reasons for rejection as a result of semen assessment result has also been analysed in another study.14 In our study, however, the vast majority of prospective donors (88.6%) were disqualified based on the results of their semen assessment as compared to the pre-freeze variables of our unit. High proportions of both suitable (77.8%) and unsuitable (71.2%) semen donors were less than 25 years old. This is probably due to the fact that the vast majority of prospective semen donors in this study were undergraduates. Poor recruitment rates for donor applicants have been observed in some countries. Using strict criteria, only 5% were accepted in United Kingdom as compared to France where 61% were accepted. However, in France, one third of these donors were liable to have some genetic diseases, which could probably be due to the fact that less rigorous method was adopted for recruiting donors.3 Lower mean or reduced sperm parameters have been reported among men aged between 20 and 40 years.15,6 In 1992, 61 separate studies examined sperm count in men from many western countries including the United States. This meta-analysis study reported an annual decline in sperm concentration of 0.93 million per ml and an overall decrease in mean sperm count from 113 million per ml to 66 million per ml.5 Other studies did not, however, find a significant difference in sperm concentration.8,9 Results from our study showed that in an attempt to assess the overall fertility potential of the population of semen donor applicants, 38.2% had their semen parameters below the reference variables of a normal semen assessment, suggesting fertility problem among this supposedly `normal' population of young healthy men. This also indicates that there is probably no correlation between age and male factor infertility. The lower limit of 15% for morphologically normal spermatozoa was based on suggestion that fertilisation rates in assisted reproductive programmes are reduced below this level.16 In order to increase the overall pregnancy rates, it was suggested that donor recruitment should be based on strict sperm morphology with emphasis on rejecting donors that do not produce pregnancies within 12 cycles. 17 In conclusion, larger multi-centre studies may be required to ascertain the trend within this group of young men. A proportion of the prospective semen donors may have sub-optimal semen parameters (using WHO reference values). Increasing the minimum requirements further, in addition to more infection screening tests, could lead to poor donor acceptance rates in a semen donation programme. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03003t2.jpg] [rh03003t1.jpg] [rh03003t.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}