 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 1, April, 2003 pp. 27-31 Prevalence of Du Phenotype amongst Rhesus Negative Females in Port Harcourt, Nigeria CA Nwauche1, OA Ejele1 and AOU Okpani2 1Departments of Haematology
and 2Obsterics and Gynaecology, University of Port Harcourt Teaching
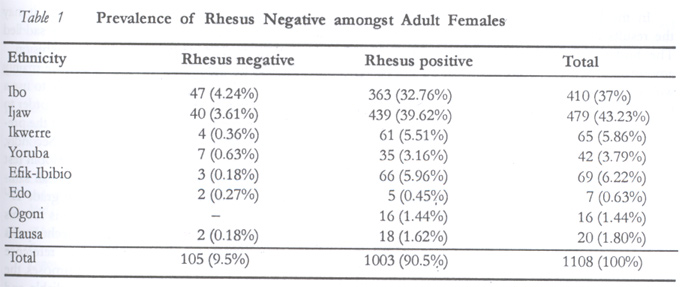
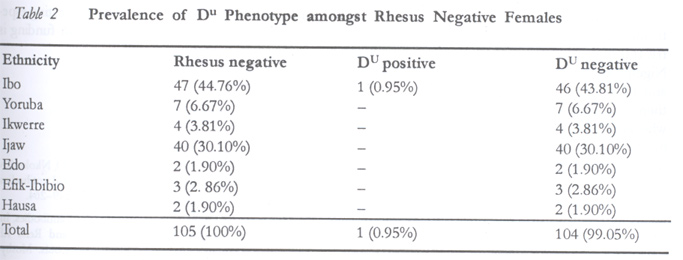
Hospital, Port Harcourt, Nigeria. Code Number: rh03005 ABSTRACT The prevalence of Du phenotype was investigated among rhesus negative women of childbearing age (15–45 years) in Port Harcourt, Nigeria, over a period of 17 months. A total of 1,108 women were randomly sampled, out of which 1,003 (90.5%) were rhesus positive and 105 (9.5%) rhesus negative. Only one (0.95%) of the Rh-negative women was Du positive while 104 (99.05%) were Du negative (true rhesus negatives). The results show that the incidence of Du phenotype in Nigeria may not be uniform — it is high among the Yorubas (7.5%) and rare among the Ijaws and Efik-Ibibios of the south-east. The results also suggest that Du testing may not be indicated in all individuals initially typed as rhesus negative while being strongly indicated only in areas of high prevalence. More studies are required in other parts of Nigeria to provide data that may facilitate the adoption of a comprehensive nationwide policy on appropriate management of rhesus negative women in the country. This will include the Du testing of all rhesus negative mothers in areas of high Du phenotype prevalence before the prophylactic administration of anti-human immunoglobulin (Rhogam). (Afr J Reprod Health 2003; 7[1]: 27–31) RÉSUMÉ Prévalence du phénotype Du chez les femmes à Rhésus négatif à Port Harcourt. La prévalence du phénotype Du a été étudiée chez les femmes à rhésus négatif qui étaient en âge d'avoir des enfants (15–45 ans) à Port Harcourt, au Nigéria, au cours d'une période de 17 mois. Au total l'étude a échantilloné 110 8 femmes au total ont été échantillonées au hasard. Le test du rhésus chez 1003 (90,5%) était positif, et négatif chez 105 (9,5%). Le test du phénotype Du était positif chez une seule femme (0,95%) parmi les femmes dans le groupe à rhésus négatif, alors que le test était négatif chez 104 (99,05%) (les vrais rhésus négatifs). Les résultats ont montré que l'incidence du phénotype Du au Nigéria peut ne pas être uniforme - elle est élevée chez les Yorubas (7,5%) et rare chez les Ijaws et les Efik-Ibibios du sud-ouest. Les résultats suggèrent également que le test du phénotype Du peut ne pas être indiqué chez tous les individus qui ont été initialement classés comme rhésus négatifs alors qu'il est bien indiqué dans les régions de haute prévalence. Il faut entreprendre davantage des études dans d'autres régions du Nigéria pour fournir des données qui pourraient rendre facile l'adoption d'une politique nationale compréhensive sur le bon traitement de rhésus négatif dans le pays. Ceci comprendra le test du Du de toutes les mères dont le test était négatif dans les régions de haute prévalence du phénotype Du avant l'administration prophylactique de l'immunoglobuline antihumaine. (Rev Afr Santé Reprod 2003; 7[1]: 27–31) KEY WORDS: Port Harcourt, rhesus negative, DU phenotype, childbearing age, women INTRODUCTION The pathogenesis and clinical sequelae of rhesus isoimmunization are well known. Proper management of the rhesus isoimmunized gravida is essential to prevent fetal mortality and morbidity. More crucial, probably, is the premarital and prenatal identification of rhesus negative women.1-3 In blood transfusion practice, Du individuals (who are actually rhesus positive) are commonly mistyped as rhesus negative through the use of polyclonal antibodies with grave consequences.4-6 These include transfusion reactions for both male and female recipients and rhesus isoimmunization. Recently the use of monoclonal antisera in many developed countries (Europe and America) has significantly reduced these undesirable phenomena to manageable proportions. In Nigeria, reports from works done in this field are apparently scarce. The classic studies of Worlledge et al in the mid 1960s7 to mid 1970s1 were concentrated mainly on the western part of the country. Subsequent studies are in agreement with their results and all place the incidence of rhesus negative population here as between one and six per cent. This indicates lower levels of rhesus negative individuals in Nigeria when compared with levels of about 17% in Caucasian populations. Conversely, the Du phenotype from published reports is higher in blacks than Caucasians (7.5% of all rhesus negative donors among the Yoruba of south-western Nigeria as against 0.6% in the United Kingdom). Studies on the Yoruba population also established that Du phenotype individuals constitute 0.4% of the general population. There is paucity of reports on rhesus negative phenomena, especially Du phenotype from the northern and delta regions of Nigeria. The Niger Delta area, where this study was done, is where most of Nigeria's crude oil operations take place. The University of Port Harcourt Teaching Hospital is the tertiary referral unit for about seven million people including expatriates, based on projections of the 1991 census figures. Blood transfusion rates average 50 units per day and by the use of polyclonal antibody rhesus typing, about 1–6% is typed rhesus negative. However, rhesus isoimmunization is rarely seen in our practice among apparently high risk rhesus negative highly parous gravidae who have never had anti-D serum at previous deliveries, suggesting lower levels of rhesus negative genotype than actually quoted. This indicates a need to determine Du phenotype to reduce the need for anti-D serum administration to gravidae typed rhesus negative by the polyclonal antibody method. We carried out the study to ascertain the incidence of Du phenotype among women typed rhesus negative by the polyclonal method. MATERIALS AND METHOD Sampling A total of 1108 adult females in Port Harcourt within the childbearing age group of 15–45 years were randomly sampled. The samples were collected over a 17-month period from the three major blood banks in Port Harcourt Local Government (PHALGA), i.e., University of Port Harcourt Teaching Hospital, Braithewaite Memorial Hospital and Orogbum Comprehensive Health Centre. Sixty seven (63.81%) of the rhesus negatives were pregnant while 38 (36.19%) were not. Method of Du Testing Samples of 3ml blood were collected from each subject by venepuncture into 10ml sterile containers and the red cells separated from the serum. Two-stage Du testing8 was then carried out, which consisted of initial rhesus grouping of all samples by the standard tile technique and indirect anti-globulin testing of samples found to be Rh-negative. Negative and positive controls were also set up at both stages of Du testing. RESULTS A total of 1108 adult females within the 15–45-year age group were randomly screened. One thousand and three (90.5%) samples were Rh-positive while 105 (9.5%) were Rh-negative. Furthermore, only one (0.95%) sample amongst the Rh-negative samples tested as DU positive and was of the Ibo ethnic group, while 104 (99.05%) were DU negative. The prevalence of Rh-negative adult females in Port Harcourt was 9.5%. Table 1 shows the prevalence of Rh-negative in the various ethnic groups screened. The two main contributors to this figure were the Ijaws, with a total of 479 (43.23%) samples of which 439 (39.62%) were Rh-positive and 40 (3.61%) Rh-negative. The second highest contributors were the Ibos with 47 (4.34%) Rh-negative and 363 (32.76%) Rh-positive samples, making a total of 410 (37%). Table 2 shows the prevalence of DU phenotype amongst the Rh-negative samples. Only one (0.95%) sample was found to be DU phenotype and was of the Ibo ethnic group, making 2.13% of all the Ibo Rh-negatives. DISCUSSION In 1966, Worlledge et al reported the incidence of rhesus negativity in Nigeria, which was found to be between 1.69 and 5.5%.10 Their finding confirmed the trend of the relatively low incidence of rhesus negativity in the country (and even in the African population) earlier highlighted by investigators such as Chalmers et al.1 Other reports in the recent past by Worlledge et al (0–6.6%),1 Udeozo (4.6%),9 Odaibo et al (2.2–5.9%),11 Odunaiya (5.2%)12 and Onwukeme (2.9–6.6%)13 have validated the finding. Similar data have also been cited in reference to people of African origin in the diaspora by Arneaud and Young, which recorded 2.5% rhesus negative among blacks in Trinidad.14 Leck also noted 7% rhesus negative among West Indian blacks living in Britain.15 The low incidence of rhesus negativity found contrasts markedly with the high figures obtained elsewhere, for example, in the UK and Basques where it is about 17% and 20–40% respectively. It is also noteworthy that there is a complete absence of rhesus negative in American Indians.16 In the light of the foregoing subsisting data, the results obtained in this study are noteworthy. The finding of 9.5% prevalence of Rh-negative among adult females in Port Harcourt is in keeping with earlier reports of low prevalence of Rh-negative in Nigeria. Again, the DU status in the study was found to be 0.95%, which was predominant in the Ibo ethnic group, a total of 2.13% of all the Ibo Rh-negative samples. This finding is at variance with that of Worlledge et al, which reported the highest figure of 7.5% among the Yorubas in a study involving 13 ethnic groups in Nigeria.17 It is also noteworthy that no DU was described among the Ijaws in both the Worlledge study and ours, but they accounted for the second highest contribution (38.10%) of Rh-negative in the study. Thus, this survey suggests that there is no uniformity in the distribution of DU across the country. It is high among the Yorubas of south-western Nigeria and completely absent among the Ijaws and Efik-Ibibios of south-eastern Nigeria. Again, there was no record of DU among the Ikwerres who are Ibo-speaking, while the mainstream Ibos produced the only DU recorded in this study. This further depicts the heterogeneity in the prevalence of DU even among somewhat homogenous entities, as seen between the Ikwerres and Ibos. The relatively low prevalence obtained in this study is noteworthy, being similar to findings in the UK where it is 0.6%. The implications of these findings in relation to the management of rhesus negativity in the study environment are significant. Firstly, the results seem to suggest that management of Rh-negatives in Nigeria is probably best carried out on a staggered module in view of the differential distribution of DU phenotype in the country. Thus, it may be beneficial to re-appraise the current practice of administrating anti-human immunoglobulin (Rhogam) to all rhesus negative females without prior DU testing across the country such that the practice may be acceptable in some areas of Nigeria like the Ijaws or Efik-Ibibios while prior DU testing would be suitable in western Nigeria. Secondly, in view of the scarcity of rhesus negative blood for transfusion in areas of high DU prevalence, it may be desirable to carry out DU testing on all prospective samples in order to ascertain the true rhesus negative blood in this environment. However, due to the high cost of the proposed scheme to the national health service, it may not be feasible in Nigeria that is currently saddled with other crucial problems of blood transfusion. Finally, the limitations of this study are mainly two-fold. Admittedly, it would be advisable to use a larger sample size in subsequent studies in order to corroborate the findings of this survey, as the present study is rather preliminary in scope. Secondly, the test method employed (indirect anti-globin test technique IAGT) is known not to detect all samples of DU – up to 25% of very low grade DU samples may be missed by IAGT and it is for this reason that the adsorption and elution technique is advocated as the gold standard or reference method. However, for all intents and purposes, the IAGT is cheap, simple and relatively reliable and still stands as a very useful tool in DU testing especially in this environment where health funding is poor and deteriorating steadily. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03005t1.jpg] [rh03005t2.jpg] |
| |||||||||

{kind=link}
{kind=link}