 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 1, April, 2003 pp. 32-36 Use of Maternity Waiting Home in Rural Zambia Luc van Lonkhuijzen1, Margreet Stegeman2, Rebecca Nyirongo3 and Jos van Roosmalen1 1 Department of Obstetrics,
Leiden University Medical Centre, the Netherlands. 2Department of
Obstetrics, University Hospital, Groningen, the Netherlands. 3Nyanje
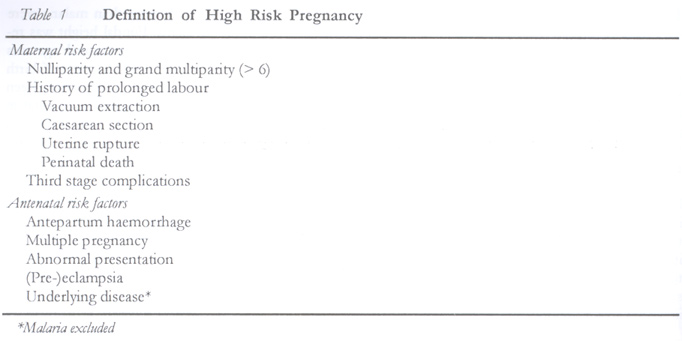
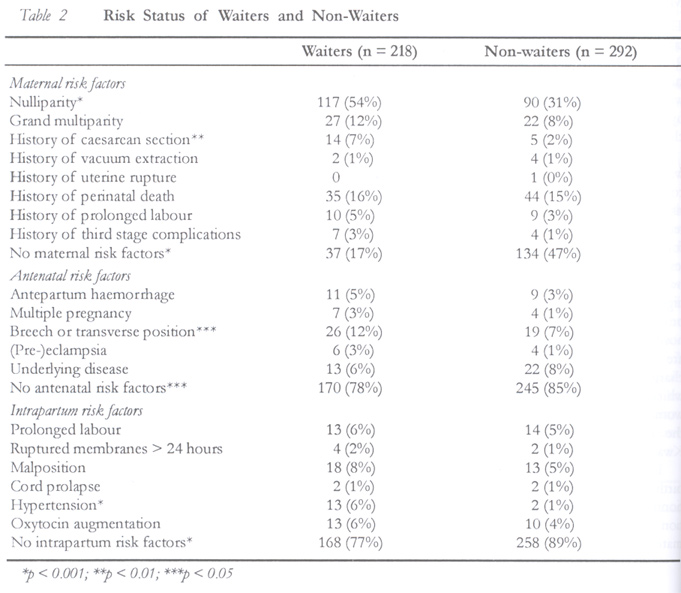
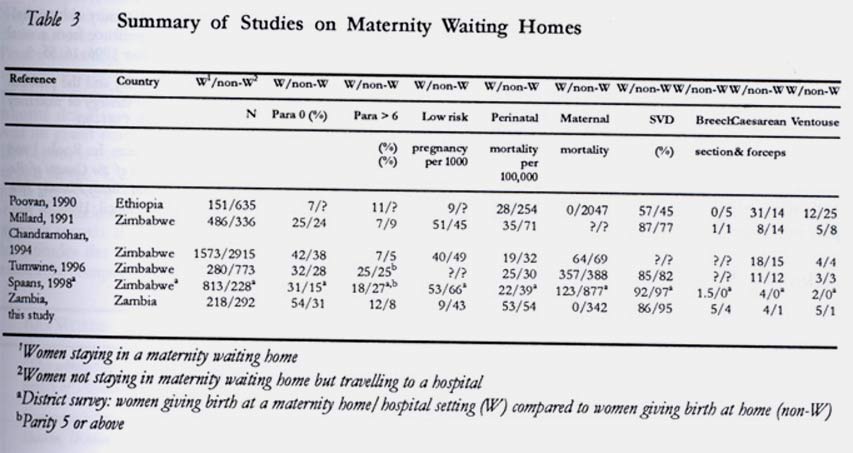
RCZ Hospital, Zambia. Code Number: rh03006 ABSTRACT This study was conducted to assess the results from the use of a maternity waiting home, a health facility to which women with high risk pregnancies are referred during the last weeks of pregnancy in rural Zambia. It compared the risk status and pregnancy outcome in women staying as waiters with those women who give birth in hospital after direct admission (non-waiters). Forty seven per-cent of the non-waiters (n = 292) had no maternal risk factors and 85% had no antenatal risk factors as compared to 17% and 78% among the waiters (n = 218). Eighty six per cent of waiters had spontaneous vaginal vertex delivery as compared to 95% of non-waiters. Although the differences in risk status were statistically significant, no differences were found in birth weight and maternal and perinatal mortality. The similar obstetric outcome among waiters with more high risk pregnancies and non-waiters could be interpreted as a possible outcome of the maternity waiting home. When dependent on a proper functioning referral system, such waiting homes can reduce perinatal mortality. (Afr J Reprod Health 2003; 7[1]: 32–36) RÉSUMÉ L'utilisation de la maison de maternité en Zambie rurale. Cette étude a été menée pour évaluer les résultats obtenus à travers l'utilisation de la maison de maternité, un établissement de santé vers lequel sont orientées les femmes de grossesse à haut risque pendant les dernières semaines de grossesse en Zambie rurale. L'étude a comparé la situation de risque et la conséquence de la grossesse chez les femmes qui sont restées dans la maison à celle des femmes qui accouchent à l'hôpital suite à une admission directe. Quarante-sept pour cent de ces dernières (n = 292) n'avaient pas de facteurs de risque maternel et 85% n'avaient pas de risque prénatal comparé à 17% et 78% chez les femmes qui sont restées dans la maison de maternité (n = 218). Quatre-vingt-six pour cent de ce groupe ont eu un accouchement vertex spontané par voie vaginale comparé à 95% de celles qui ont accouché à l'hôpital. Bien que les différences par rapport à la situation de risque soient statistiquement significatives, il n'y avait pas de différences en ce qui concerne le poids de naissance et la mortalité maternelle et périnatale. Les résultats obstétriques pareils chez les femmes à grossesse à haut risque qui restent dans la maison de maternité et chez les femmes qui ne sont pas restées peuvent être interpretés comme étant des résultats possibles de la maison de maternité. De telles maisons de maternité sont capables de réduire la mortalité quand on s'appuie sur un bon fonctionnemment du système d'orientation des patientes vers les spécialistes. (Rev Afr Santé Reprod 2003; 7[1]: 32–36) KEY WORDS: Maternity waiting home, high risk pregnancy, perinatal mortality, maternal mortality INTRODUCTION The World Health Organization (WHO) considers maternity waiting homes (MWH) as an essential element of maternity care.1 It has been suggested that in rural areas, where women live far from a health facility and transport is poor and often impossible when complications of labour occur, maternity waiting homes can play an important role in reducing maternal and perinatal mortality.2-4 When access to care is difficult, women with high risk pregnancies should be admitted to a waiting home at 36 weeks of pregnancy. In such facilities they can await the onset of labour in the vicinity of a hospital. Few studies have been published to assess the role of maternity waiting homes. This study was, therefore, conducted to evaluate its use in a rural area in Zambia. MATERIALS AND METHODS The study was conducted in Nyanje RCZ Hospital between May and November 1994. Nyanje RCZ Hospital is a 120-bed hospital situated in a rural area in the Eastern Province of Zambia with approximately 60,000 people. Monthly visits by hospital staff are paid to 10 outreach MCH clinics. Distance to the nearest hospital is 80km. Next to the maternity ward is the maternity waiting home made of a small building that can accommodate 10 to 15 women. Women with high risk pregnancies (Table 1) are advised to be admitted to this home. Risk assessment is usually performed by midwives at the monthly outreach clinics. Few women come to stay as waiters on their own initiative, and in general only women with high risk pregnancies are admitted. The hospital provides food for the waiters. The women visit the hospital's antenatal clinic once a week where they are also given health education. The waiters are charged an admission fee of 1,000 Kwacha (US$3), which includes the cost of hospital birth. Also women deliver in hospital after direct admission to the labour ward and they are charged 2,000 Kwacha (US$6). Data were compiled of all women who gave birth in hospital during the study period. A questionnaire was filled in by the midwives. Information was collected on socioeconomic status and maternal risk factors from history and the present pregnancy. Only other diseases than malaria were considered as a risk factor. Fundal height was recorded, but information on gestational age was either lacking or unreliable. The outcome of birth up to discharge was also recorded. Data have been compared for women who gave birth after a stay in the MWH (waiter) and those who gave birth after direct admission to hospital (non-waiter). The differences between waiters and non-waiters were assessed using chi-square and student's unpaired t-test. RESULTS During the study period, 581 women gave birth in hospital. Owing to procedural imperfections, data from 61 women were lacking, thus only 520 were used for analysis. Twenty women gave birth to twins. In the non-waiter group nine women were excluded because of an emergency admission for diarrhoeal disease (n = 2), antepartum haemorrhage (n = 3) or obstructed labour (n = 4). It was not certain whether one woman stayed as a waiter or not. The study group thus consisted of 218 waiters and 292 non-waiters. The average ages of the waiters and non-waiters were 23 and 23.5 years respectively. Waiters produced more maize than non-waiters (p < 0.05). Waiters had the tendency to be more educated, but the difference was not statistically significant (p = 0.08). Distance from the place of residence to hospital was 22km (range 2–80) for waiters and 13km (range 0–66) for non-waiters (p < 0.001). Waiters were more often nulliparous (p < 0.001). They also had history of previous caesarean section more frequently (p < 0.01). Only 17% of the waiters had no maternal risk factors as compared to 47% of non-waiters (Table 2) (p < 0.001). Breech or transverse presentation occurred more frequently in the waiter group (p <0.05). Many women suffered from underlying disease such as malaria only in majority of cases, but a few other diseases such as tuberculosis and sexually transmitted disease were prevalent as well. More women (85%) in the non-waiters group had no antenatal risk factors as compared to 78% among waiters (Table 2) (p < 0.05). More women in the waiters group suffered from hypertension during birth (p < 0.001) while more women (89%) in the non-waiters group had no intrapartum risk factors as compared to 77% of waiters (Table 2) (p < 0.001). Among non-waiters 95% had spontaneous vertex delivery as compared to 86% of waiters (p < 0.01). This difference was also reflected in the higher rates of breech delivery, caesarean section (p < 0.05) and vacuum extraction (p < 0.01) in the waiters. No difference was found in perinatal and maternal mortality between the two groups (Table 3). Mean birth weight of the children in both groups did not differ (2873g in non-waiters versus 2857g in waiters). There was no difference in the percentage of low birth weight (< 2500g) either (Table 2). DISCUSSION Facilities called maternity waiting homes by the WHO are also described in literature as maternity villages, maternity waiting shelters or dormitories, antenatal villages, antenatal shelters or hostels. Despite this variety of names, only few documents on their use and effectiveness have been published.5-9 Findings of these studies and ours are summarised in Table 3. The maternity waiting home was originally intended to be used by women with high risk pregnancies whose homes are in remote and inaccessible rural areas. This original concept is adapted in various ways all over the world.10 One of the important factors on which the success of a maternity waiting home is based is a properly functioning referral system. All women with high risk pregnancies should be referred while those with low risk pregnancies may deliver at home. Most of our waiters (91%) had high risk pregnancies and they lived at greater distance from hospital compared to the non-waiters. We found more nulliparous women, women with a history of previous caesarean section or women with breech or transverse presentations in the waiter group. On the other hand, 57% of the non-waiters still had high risk pregnancies, and of these 27% were living outside 20km radius. From our data, however, we conclude that the referral system in our study area is functioning reasonably well. The fact that the hospital provides food for the waiters could well be a stimulus that encourages its use. In the Karawa health zone in Zaire, the lack of this service was one of the reasons that the maternity waiting home was rarely used.11 Although the waiters had more high risk pregnancies, the outcome of pregnancy was not worse than for non-waiters. Perinatal mortality was similar in both groups and there was no significant difference in birth weight in either group. In contrast to our study, a large part of the waiting population in Millard's and Chandramohan's studies consists of women with low risk pregnancies (Table 3). In our study, the overall perinatal mortality is 53 per 1000. We cannot gauge whether this figure is an underestimation, as we have no knowledge what happens to the children once they leave hospital. The studies in Zimbabwe and Ethiopia all show a lower perinatal mortality for women staying in a MWH as compared to non-waiters (Table 3). Each author, however, points out the fact that there was a bias. In Ethiopia, the stillbirth rate was ten times higher in the non-waiters than in waiters. This was ascribed to the fact that many women in the non-waiter group were emergency admissions with severe complications. In our study, one maternal death occurred only in the non-waiters. The main difference in outcome is the number of assisted births, which is related to the higher risk of pregnancies in the waiters. We assume that the women staying as waiters had their operative deliveries for good medical reasons. When they, for whatever reason, would have decided to give birth at home, perinatal outcome would probably have been worse. The similarity in perinatal outcome for waiters with significantly more high risk pregnancies than in the non-waiter group can be interpreted as the positive effect of the MWH. The method used in ours and other studies clearly has its limitations. It will always be difficult to draw firm conclusions on the effectiveness of MWH by comparing two groups delivering in hospital. Unknown bias may account for the differences in outcome between the groups. A more effective study design would be to compare pregnancy outcome in two separate communities, one with and another without a MWH. The best method in a large community would be to assign women at random to a MWH. This, however, presents problems with the conduct of such study protocol in the difficult circumstances of a rural hospital. Nevertheless, we feel confident to conclude that in rural Zambia MWHs with appropriate selection of high risk pregnancies play important roles in reducing perinatal mortality. ACKNOWLEDGEMENT We thank the midwives and hospital staff of Nyanje RCZ hospital for their efforts and dedication towards data collection, and the pregnant women for their cooperation. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03006t2.jpg] [rh03006t3.jpg] [rh03006t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}