 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 1, April, 2003 pp. 63-70 Gender and Health Analysis of Sexual Behaviour in South-Western Nigeria AS Jegede1 and O Odumosu2 1Department of Sociology,
University of Ibadan, Nigeria. 2Nigerian Institute of Social and
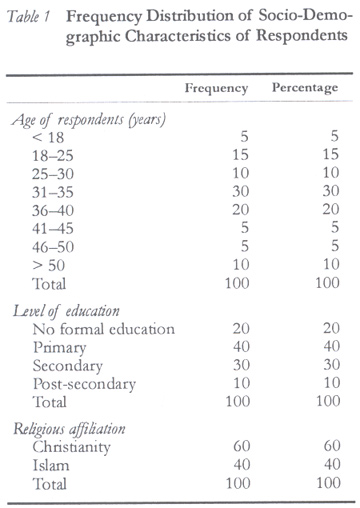
Economic Research (NISER), Ibadan, Nigeria. Code Number: rh03009 ABSTRACT This paper reports the main results of a series of interviews conducted among the Yoruba of south-western Nigeria. Fifty men and fifty women differing in socio-demographic backgrounds were studied. The study revealed that during their first sexual experience, Yoruba girls are at risk of contacting sexually transmitted diseases and of having unplanned pregnancies because of the traditional control measures and lack of adequate sex education even among those from non-traditional backgrounds. Choice of marriage partner is influenced by the kin, which encourages early marriage and multiple sexual relationships through polygyny. Yoruba men do not like contraceptives and the women suffer more of the consequences of sexual relationships than men. Sexual decision-making in Yoruba culture is characterised by certain specific problems of structural and cultural origins such as separate lifestyle of men and women, seeing the discussion of sexuality as a taboo, male dominance, and the perceived side effects of contraceptives. There is need for expanded sexual and reproductive health education strategies targeted at both males and females in this community especially among the adolescent group. (Afr J Reprod Health 2003; 7[1]: 63–70) RÉSUMÉ Analyse des sexes et de la santé pour le comportement sexuel au sud-ouest du Nigéria. Cet article fait un rapport des principaux résultats d'une série d'entretiens que nous avons eus avec des Yoruba du sud-ouest du Nigéria. Cinquante hommes et cinquante femmes d'origine Yoruba domiciliés à Ibadan, mais qui viennent des milieux socio-démographiques différents, ont été étudiés. L'étude a été basée sur une analyse de leurs histoires sexuelles, à l'aide d'une méthode de recherche qualitative. La recherche a démontré que pendant la première expérience sexuelle, les filles Yoruba courent le risque de contracter les maladies sexuellement transmissibles et d'avoir des grossesses non-désirées. Ceci à cause des mesures de contrôle traditionneles et le manque d'éducation sexuelle adéquate même parmi ceux qui ne sont pas issus des milieux traditionnels. Le choix du conjoint est influencé par la famille qui encourage le mariage précoce et les rapports sexuels multiples à travers la polygynie. Les hommes Yoruba n'aiment pas les contraceptifs alors que les femmes souffrent plus les conséquences des rapports sexuels que les hommes. La prise de décision sexuelle dans la culture Yoruba est caractérisée par certains problèmes particuliers d'origine structurale et culturelle, tels les modes de vie différents des hommes et des femmes, la considération de la discussion sur la sexualité comme un tabou, la dominance masculine et les effets secondaires perçus des contraceptifs. Il y a la nécessité des stratégies de l'éducation sexuelle et de la santé reproductive qui viseront les femmes dans cette commumauté surtout parmi le groupe adolescent. (Rev Afr Santé Reprod 2003; 7[1]: 63–70) KEY WORDS: Gender, health, sexual behaviour, contraception INTRODUCTION Debates on reproductive health and contraceptive decision-making centre around the family and about the roles men and women play within it. Although socio-demographic literatures argue that women's and men's social roles and power relations have important implications for fertility levels1-3, it is not clear through what mechanisms gender affects reproductive and contraceptive decision-making, especially in the Nigerian setting. As in other parts of Africa, the extended patriarchal household is widespread in Nigeria. In such patriarchal societies, men's domination limits female ability to influence decisions whether at the macro or micro level. Generally, women are regarded as the weaker sex and as a result are considered subordinate to men. They are allowed limited opportunities in decision-making even in matters that affect their health. Various studies on sexuality, early marriage, fertility rate and widowhood practices indicate gender differential in sexuality decision-making.4-8 The desire by many couples for a large family size is a result of the positive value that the Nigerian society attaches to marriage, family life and procreation. However, women have to bear the negative consequences associated with this desire. At marriage, a woman assumes a relatively low status among members of her husband's extended family, which can only be elevated by her reproductive capacity. As a result, women are given out in marriage as early as 15 years of age in some parts of Nigeria and cannot take decision about the number of children they would want to bear.8-11 Recent data for Nigeria12 indicate high maternal morbidity and mortality rates. Most of the health problems result from sex related diseases. Because of the low level of family planning in Nigeria, women of childbearing age are very much susceptible to sexually transmitted diseases (STDs) such as syphilis, gonorrhoea, acquired immuno-deficiency syndrome (AIDS) and vesico-vaginal fistula (VVF). Studies have shown high incidence and prevalence of these problems in Nigeria.6,7 Although sexual intercourse is an activity involving two people, it results in a change of the status of the woman to that of a patient while the man retains his normal status of wholesomeness. Frederichs argued that the road to death for women continues from infancy through adolescence when girls often marry and get pregnant at early age.13 Because women are not empowered economically, with little or no access to land, training, wage, employment or any means of financial support they may be unable to obtain family planning services without their husbands' consent. The change in status may put women on the danger list of haemorrhage, eclampsia, obstructed labour, puerperal sepsis, illicit abortion and indeed death. The question, therefore, is why can't women who are usually the victims of sexuality decision-making influence such decisions in their favour? American researchers have come up with two seemingly contrasting explanations.14 The structuralists believe that because of the poor socio-economic and educational condition of the black population they are not well-informed about contraceptive methods, no future prospects, and they lack the motivation needed to be active family planners.15 Culturalists on the other hand posit that the norms and values that linger in the black society hinder them from using contraceptives effectively. These approaches can be extended to explain the problem of sexuality in Nigeria. This paper, therefore, explores the process of decision-making about sexuality among the Yoruba of south-western Nigeria and examines the health implications for the parties involved. It also examines whether the American-based theoretical discussion can also be applied to the Yoruba culture. Family Planning in Nigeria In Nigeria, women have been known to use improvised methods of emergency contraception such as Andrew's liver salt, Schweppes Bitter Lemon, salt and potassium solution. More commonly they douche with water only, or soap and water, salt and water, local herbal solutions, Dettol (antiseptic), alum solution, lime and vinegar after unprotected intercourse to prevent pregnancy. In a study of adolescent pregnancy in Nigeria, 80% of pregnancies among unmarried girls were aborted. The number of women at risk of pregnancy is determined by age, patterns of marriage and sexual practice. A relatively late age of marriage and a nuclear pattern of family building have characterised marriage in the western part of the country for many years. It partially accounts for the low birth rates in Europe before the industrial revolution. Where the extended family system is common the age at marriage is usually less and parents play a major role in the selection of partners. In many developing countries where the mean age at marriage is in the teens rather than in the twenties the average family size will be larger than it is in industrialised nations. Assuming that the practice of contraception is effective, i.e., in an imaginary healthy population where all women marry at the age of 15 years and remain married until at least the age of 50 and where no birth control or exclusive breastfeeding is practiced, the average woman will bear about 15 children during her lifetime. It has been observed that contraceptive use in Nigeria is very low (11.3%). Among youths, sexual activity is not planned and precautions are not taken to prevent unintended pregnancy and sexually transmitted diseases, which often leads to abortion. There is also the growing awareness that complications resulting from unsafe induced abortion are important contributing factors to the high rate of maternal mortality and morbidity in developing countries. Studies have shown that unintended pregnancy and induced abortion are common in Nigeria and constitute a public health problem. Of the 50,000 maternal deaths estimated to occur in Nigeria annually, nearly 20,000 are attributed to complications from unsafe abortion. These abortions often result in death or leave the women mutilated or infertile. Women in Nigeria have been known to use non-professional contraceptive methods rather than the more reliable modern methods. No recent studies have reported on the effectiveness of these methods, but their continued use is an indication that Nigerian women have need for emergency contraception. Reports of a survey conducted by the Society for Family Health (SFH) and the Planned Parenthood Federation of Nigeria (PPFN) (major distributors of family planning products in Nigeria) revealed that both the IUCD and hormonal methods are available in the country. The reports also indicated that many pharmaceutical retail outlets in some parts of Nigeria have postinor, a major product designated for emergency contraception. Data suggest the reasons for non-use of modern methods of emergency contraception by Nigerian women. These include lack of information, non-use, non-availability of programme on emergency contraceptive and lack of trained providers. METHODS Fifty men and fifty women of Yoruba descent in Ibadan were recruited to take part in this study. Data were collected using in-depth interviews based on a list of items including family history, upbringing, age at marriage, age at first intercourse, sexual relationship patterns, etc. In some cases a second and a third interview was conducted to obtain further information on sexuality history of the respondent. These interviews were tape-recorded. The group of 50 men and 50 women was fairly representative of Yoruba men and women differing in age, education, social class, number of children, kind of relationship, etc, for a qualitative study of this nature using in-depth analysis. The study lasted five months, between February and June 1999. The researchers, being Yorubas, employed an emic view to evaluate and interpret data collected. They were also at advantage in understanding the views and system of values of the respondents. Majority (60%) of the respondents were between 30 and 49 years of age, 22% were below 30 years and 18% were above 50 years. About 20% of the respondents had no formal education, 35% had only primary education, 25% had secondary education and 20% had post-secondary education. Majority (53%) were Christians while 47% were Muslims. Since this research material was limited to 50 men and 50 women only, there is a need to describe in general terms the common problem of sexual behaviour among Yoruba women. To show these problems in their proper context, this paper presents the findings in two different phases of reproductive life cycle. RESULTS Socio-Demographic Characteristics of Respondents First Dating The data reveal that during their first sexual experience, Yoruba girls are at a high risk of contracting STDs and having unplanned pregnancies, for two major reasons. Firstly, traditional control prescribes premarital chastity to preserve female virginity at the time of marriage. This results in total exclusion of female adolescents from any discussion pertaining to sex and birth control, a practice that seems to persist in the face of general moral laxity particularly in the urban centres. Hence, they cannot make use of contraceptives openly. Secondly, among those who had secondary and post-secondary education, only a few confessed to have had adequate sex education. Sex education is lacking, most especially in the Muslim controlled schools. Another factor is the instability of many relationships. Yoruba girls tend not to use contraception unless they are sure that the relationship with their partner is a serious one that will last long. The female partners believe that a pregnancy will convince her partner of her fecundity. The men also desire that their female partners get pregnant before marriage in order to prove their fertility. This predisposes them to the risk of infection with STDs and unwanted pregnancies. In a `programmed' relationship, however, the couple may use contraception until they are ready for procreation. One respondent said:
During the early reproductive years, only the `indecent' girls engage in premarital sex and use contraception, although girls from the non-traditional backgrounds are more likely to have experienced premarital sexual relationships at the time. The study also indicates that premarital sexual experience is relatively common among girls from traditional backgrounds. Girls from the non-traditional backgrounds may become effective users of contraceptives if their male partners demand for it and both are committed to the relationship. Some of the female respondents became effective users of contraceptives with the cooperation of their male partners when they were sure of their relationship. Yoruba boys, especially the highly educated middle class with high aspirations, usually make their partners know that they do not want to become fathers at a young age. An important finding of this study is that only a few of the violators of premarital sexual taboo practice contraception. This has implication for sexual and reproductive health. Forced Marriage The data show that Yoruba girls, whether living at home or abroad, are delighted to get married. However, they cannot make absolute decision about who to get married to regardless of the level of education. Their choice is subject to family approval. Most of them usually become sexually mature at a relatively young age and so they are given out in marriage for two major reasons. Firstly, `gift marriage', a practice by which mostly the Muslims give out under-aged girls of about 15 years old in marriage. Secondly, because marriage attracts high bride wealth, the lower income people who cannot afford to send their wards to formal or non-formal schools give them out in marriage at a tender age. Some of these young brides are not biologically mature and thus are at high risk of developing reproductive complications such as vesico-vaginal fistula. Their pregnancies usually result in complications that sometimes lead to permanent disabilities or outright death. They are also not mature for their new role as mothers. Polygyny Polygyny is a function of social structure and it is highly practiced among the Yoruba. Being a patrilineal society, women have no power to refuse sexual advances from their husband. The multiple sexual nature of polygyny may, however, lead to serious reproductive health problems. Although extra-marital sexual relation (ale) is frowned at in the society, it is widely practiced especially by women in polygynous unions. They do this to make up for the inadequate attention by their husbands. A husband may contact venereal disease from one of the co-wives and transmit it to the others because they cannot refuse his sexual advances. Birth Interval The study also confirms that women neither have the opportunity to decide on when to have children nor can they decide on the number of children they want. Although the traditional child-rearing practice demands two to three years weaning period, sometimes women throw this rearing practice overboard because of competition among co-wives in order to have the favour of their husbands and kinsmen. This usually leads to too early, too closely spaced and too late pregnancies with their concomitant risks. In this circumstance, women do not use contraception. Abortion Women usually resort to induced abortion if they have unintended pregnancies because of its social consequences, especially if it is outside marriage. Half of the six abortions discussed during the research occurred too soon after the birth of a baby. Christian couples avoid aborting a pregnancy because they see it as “killing a child”. Some women resort to induced abortion because of negative social stigma attached to closely spaced pregnancy and the perception that the living child is an “ultimately weaned child” (alasibo). Others resort to abortion for economic reasons, lack of time, support or space to raise another child especially when the woman is still in school or learning a trade, as indicated in the following response:
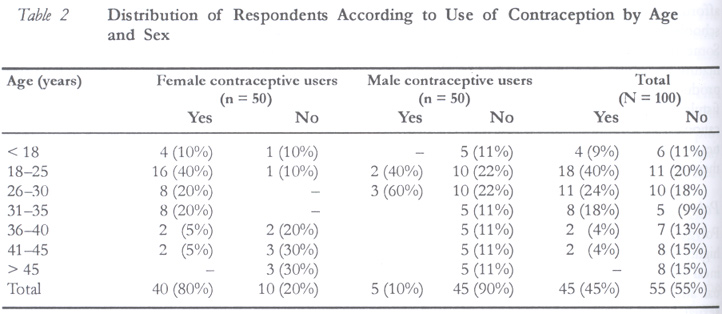
This study found that ineffective use of contraception is most common among women with low educational status. Educated women generally would prefer an abortion. Women with secondary education prefer abortion because they want to have a bright future economically. They want to complete their education or trade before bearing children. The decision to abort is seriously frowned at because many ill-performed abortions cause physical and traumatic experiences. Most women, therefore, try hard to avoid unwanted pregnancy after experiencing abortion once. Contraception This study highlights some of the problems associated with sexual behaviour. For instance, Yoruba men do not like to use condoms, and sterilisation is even more disliked. For these men, sterilisation means loosing their masculinity. Data show that less than one half (45%) of the respondents (females and males) have ever used contraception. Majority (90%) of the 50 male informants stated that they had never used any contraception, while 10% indicated using condoms. These are likely to be unmarried young adults who want to prevent unwanted pregnancies and sexually transmitted diseases (STDs) including HIV/AIDS. This shows a marginal acceptance rate of condom by men. However, all the men (100%) reported that they never attempted or would attempt sterilisation. There is no variation by age for sterilisation. Majority of the male condom users (90%) were aged between 18 and 30 years. This is not surprising since this is the most sexually active unmarried group who may want to avoid unwanted pregnancies. Majority of contraceptive users (70%) were young women aged between 15 and 30 years, while majority of non-users were the older generation (80%) aged 35 years and above. The dropouts were mostly (70%) aged 35 years and above compared to 30% of women below 30 years of age. This shows that the trend in contraceptive adoption is changing with the younger generation favouring it more than the older generation. Most of the women (45%) attempted different brands of pills during their reproductive life. However, some (15%) stopped using them because of side effects; they believe that contraceptives cause more harm than good. In most cases women used contraceptives without the knowledge of their partners for fear of being accused of sexual promiscuity. Also, there is generational differential among women using contraceptives. Contraceptive use in the first phase of reproductive life was also hindered by the attitude of men. Most men did not like condom. They complained that they don't enjoy sex with condoms, as indicated in the following statement:
Besides, they feel that decent girls should not use condoms since their sexual behaviour is not expected to lead to venereal diseases. It was argued that:
The study also found that after delivery many mothers don't use contraceptives. Mothers who breastfeed do not like to use contraceptives because they feel that it would affect their baby.
Such women are at risk of unwanted pregnancy and subsequent induced abortion. Some Yoruba women sometimes get pregnant within one year after the birth of their first baby, which is contrary to traditional practice. DISCUSSION Apart from the problems of contraceptive use, many Yoruba men and women have to overcome their negative perception of family planning; they feel that it has spiritual consequences. As some said:
For example, a man narrated the story of a woman who used a family planning method but was not able to get pregnant when she needed children. He believed that witches had taken advantage of the family planning practice. Other informants indicated that contraceptives are not natural and that they can cause illnesses. The low level acceptance and use of modern contraceptive techniques among traditionalists is related to the fear of posing a challenge to fate if they took personal initiative with regard to a phenomenon that is best left to the gods. There is perceived relationship between contraceptives and the body. The Yoruba believe that the body is an extension of the world and the custodian of the soul, which should be in constant contact with the ancestral spirits. Therefore, the body must be pure and monitor its messages in terms of health and illness. An unhealthy body is believed to produce imbalanced relationship between the soul and the spiritual beings. They say that communication with the body comes through dreams, and that the wishes of the gods for the body are revealed in the dream. Therefore, the body should not be polluted but should remain pure. Sexuality issues are sacredly guarded by the Yorubas. It can only be discussed by the elders. Young members of the society, especially females, are not allowed to discuss sexual matters. This has implications for sex education and contraceptive use. Since elders remain the `gate-keepers' of knowledge about sexuality issues, sex education cannot make an easy in-road to the life of young members of the community. A young woman reported that she dropped out of school when she got pregnant because she could not discuss the issue with her parents. She attempted abortion but it became complicated and thus led to her expulsion from school. Another woman claimed that she suffered from a venereal disease for a long time before she got married because she did not have the money to treat herself and she could not tell her parents. In the Yoruba community, females suffer more effects of sexual relationships than men. Apart from the fact that when they become pregnant they transfer to the community of patients till delivery, they are more vulnerable to most sexually related diseases than men. Also, because of their disadvantaged position in the society they lack resources to take care of themselves. They depend mostly on men who sometimes neglect them after sexual intercourse. Even when the women have resources to take care of themselves they lack the legal rights to be accepted for treatment in the hospital for sex-related problems without the presence of their sexual partners. Women therefore suffer double burden. While they are faced with the problem of taking decisions about their sexual life, they are rejected by the society and their partner when there is any resulting problem. CONCLUSION Sexual decision-making among Yorubas is characterised by certain specific structural and cultural problems. These include separate lifestyle of men and women, the taboo on discussion of sexuality, male dominance role and the perceived side effects of contraceptives. In sum, the upbringing of Yoruba boys and girls, beliefs and lifestyle, as well as the long-lasting unfavourable socioeconomic circumstances increase the risk of sex-related diseases. Several studies have indicated that sexual relationship is particularly high among unmarried youths in Nigeria. An increasing number of Yoruba adolescents migrate from rural areas to urban centres in search of jobs, opportunities for higher education or for apprenticeship, thus breaking away from constraints traditionally applied by family members and village communities. However, having moved from a traditional background where discussion about sexuality is a taboo, especially among the females, the young woman who is sexually active in the urban centre is at risk of unwanted pregnancies and STDs due to either lack of adequate knowledge of contraception or inability to openly use contraceptives for fear of being stigmatised as a promiscuous person (asewo). Although contraceptive decision-making is often left to the men in most cases, the passive role of Yoruba men in the choice of contraceptive method or abortion is often very decisive. First of all, by refusing to use contraceptives, the choice of contraception for Yoruba women is limited. Lack of commitment of Yoruba men to their partners is a problem facing contraceptive decision-making for the women; therefore, they are exposed to the danger of sexually related illnesses. These two factors combined with the biological factor may also partly explain why the level of sexually related morbidity and mortality is higher among women than men. They are at the receiving end and carry the burden of STDs and reproductive diseases apart from the fact that they lack access to preventive and curative care. However, it is concluded that there is greater differential in sexuality decision-making among the Yoruba, and that women experience effects of sexually related problems more than men. The study has shown the relevance of structural and cultural model theory in the explanation of sexuality decision-making among Yorubas. Both structuralist and culturalist approaches provide information for understanding the interactions between gender, health and sexuality. It is recommended that a special programme that will focus on the male folk to compliment the current emphasis on women be designed. Parents should be educated on the dangers of denying their children access to sex education. It is imperative that contraceptive devices be made available free of charge so that people can have access to them. Finally, programmes should be designed to improve the economic status of women to reduce their dependence on men. This will increase their chances of influencing decision-making on matters affecting them. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03009t2.jpg] [rh03009t1.jpg] |
| |||||||||

{kind=link}
{kind=link}