 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 1, April, 2003 pp. 103–112 Attitudes of Health Care Providers to Persons Living With HIV/AIDS in Lagos State, Nigeria Sylvia Bolanle Adebajo1, Abisola O Bamgbala1 and Muriel A Oyediran2 1Department of Community
Health and 2Institute of Child Health and Primary Care, Lagos University
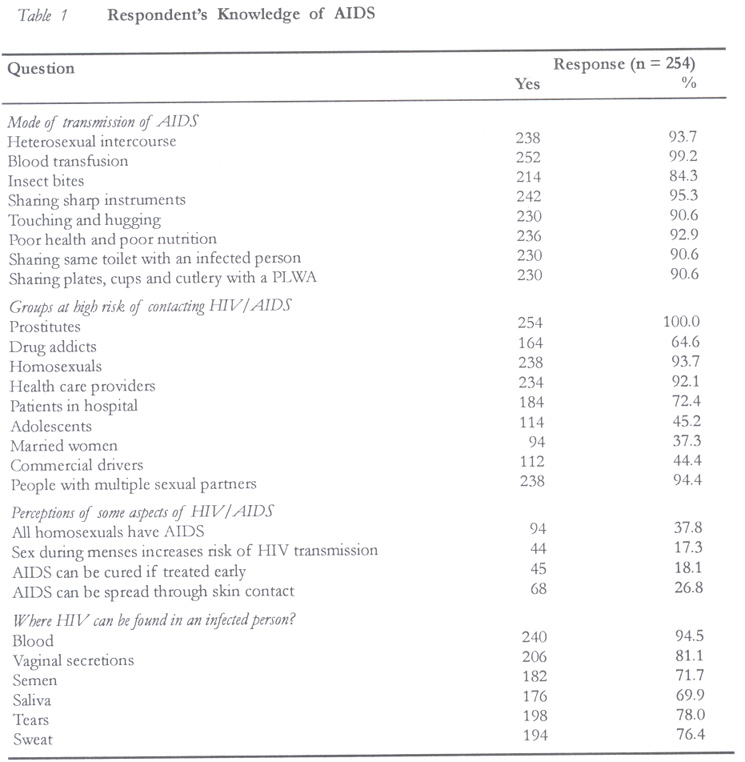
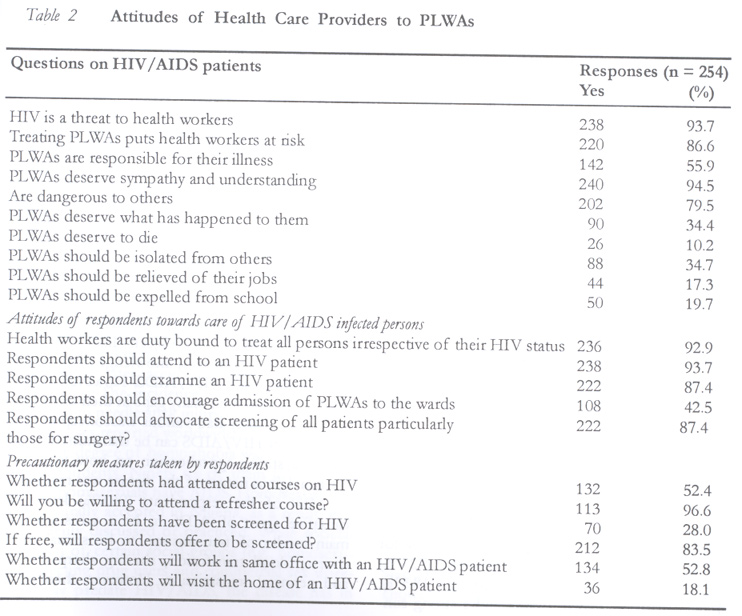
Teaching Hospital, P.O. Box 2088, Lagos, Nigeria. Code Number: rh03013 ABSTRACT This study was conducted to examine the knowledge, beliefs and attitudes of nurses and laboratory technologists towards people living with HIV/AIDS (PLWA) and the factors responsible for these attitudes. Information was elicited from 254 randomly selected nurses and laboratory technologists from 15 government owned health facilities in Lagos State with the use of a structured questionnaire. Results indicate that most of the respondents (96.3%) had moderate to good knowledge of HIV/AIDS. Respondents' level of knowledge was influenced by the level of formal education attained, length of practice, gender and attendance at refresher courses on HIV/AIDS (p < 0.05). In contrast, respondents' age, occupation and religion did not significantly influence their level of knowledge (p > 0.05). Attitude towards PLWA was poor. Some (55.9%) of the health workers felt that PLWAs are responsible for their illness, while 35.4% felt that they deserve the punishment for their sexual misbehaviours. Only 52.8% of the respondents expressed willingness to work in the same office with a PLWA, while only 18.0% would accept to visit or encourage their children to visit a PLWA, probably because of the fear of contagion. It is, therefore, essential that health care providers be properly informed in order to improve their quality of care for PLWAs. (Afr J Reprod Health 2003; 7[1]: 103–112) RÉSUMÉ Attitudes des dispensateurs des soins médicaux envers les sidéens dans l'etat de Lagos. Cette étude a été menée pour examiner la connaissance, les croyances et les attitudes des infirmières et des techniciens de laboratoires envers les sidéens et les facteurs qui en sont responsables. L'information a été recueillie, à l'aide d'un questionnaire structuré, auprès de 254 infermières et techniciens de laboratoire selectionnés au hasard dans 15 hôpitaux gouvernementaux dans l'Etat de Lagos. Les résultats ont montré que la plupart des interrogés (96,3%) ont une bonne connaissance du VIH/SIDA. Le niveau de connaissance chez les interrogés a été influencé par le niveau de l'éducation formelle atteint, la durée de la pratique, les sexes et la fréquentation aux stages de recyclage sur le VIH/SIDA (p < 0,05). Par contre, l'âge, le métier et la religion des interrogés n'ont pas influencé, leur connaissance de manière significative, (p < 0,05). L'attitude envers les sidéeens était mauvaise. Certaines (55,9%) parmi les infirmières estimaient que les sidéens étaient responsables de leur maladie alors que 35,4% estimaient qu'ils méritaient la punition pour leurs mauvaises conduites sexuelles. Seuls 52,8% des interrogés ont exprimé la volonté de travailler dans le même bureau que les sidéens alors que 18.0% aimeraient visiter ou encourager leurs enfants de visiter les sidéens probablement de peur d'être infectés. Il est donc bien nécessaire que les dispensateurs des soins médicaux soient bien informés afin d'améliorer leur qualité de soins pour les sidéens. (Rev Afr Santé Reprod 2003; 7[1]: 103–112) KEY WORDS: AIDS, HIV, attitude, health care providers, PLWA INTRODUCTION From the beginning of the pandemic in 1981 to date, HIV has continued to spread at the rate of more than 10,000 new cases per day despite significant efforts made to contain its spread.1 If this trend persists unchecked, a cumulative total of over 60 million adults would have been infected by the end of the year 2000 with the largest number (63%) emerging from sub-Saharan Africa.2 Nigeria, the most populous country in Africa is not spared, as the epidemic continues to show a rapidly increasing trend with a median prevalence of over 5% and over two million people already infected.3 With the increasing number of people living with HIV/AIDS, AIDS control and preventive strategies must not only continue to encourage behavioural modifications by all, but should also highlight the need to respect the rights to care of the increasing number of people with HIV/AIDS. In addition, there should be full integration of these persons within the context of their families and the society at large in the most appropriate ways that would allow them to continue to live productive lives socially and economically.4 In reality, however, the fear of being infected at workplaces, educational institutions and in the community has led to irrational and discriminatory treatment of people living with HIV/AIDS (PLWA). Their rights to employment, housing, education and even health and nursing care are being violated because of their HIV status.5-7 This practice unfortunately exists despite strong evidence from research that has revealed that non-sexual contact with HIV positive individuals carries little or no risk.5, 8-11 This is even more so if careful precautions with blood products are taken, as this further protects people from contracting the infection.6,12-14 Health care providers, who are also members of the general community, are likely to elicit similar prejudicial and fearful reactions to HIV/AIDS infected persons as members of the community. The resultant effects of such negative attitudes include poor patient management, with people being denied most needed treatment, care and support. This in turn could affect their morale, self-esteem and self-determination to live quality lives devoid of stigma, fear, repression and discrimination.15,16 Maintaining the desired quality of life of people with HIV/AIDS is possible mainly through extensive, competent and compassionate nursing care. Yet, the provision of this care raises health and occupational concerns for all levels of health care providers.7 There is, therefore, an urgent need for all health care providers, particularly nurses who have direct contact and spend more time with patients, to examine their personal attitudes towards PLWAs, as this can compromise compassionate care. This study is aimed at determining the level of knowledge, attitudes and beliefs of nurses and laboratory technologists towards HIV/AIDS infected persons and to recommend appropriate measures to address the deficiencies identified. MATERIALS AND METHODS This descriptive cross-sectional survey of three hundred registered nurses and laboratory health technologists was conducted between July and September 1999 in Lagos State, the most populous state in Nigeria. It was conducted to assess their level of knowledge of the causes, modes of transmission and methods prevention of HIV/AIDS and their attitudes to people living with HIV/AIDS using a well structured, self-administered questionnaire that contained 44 items. With permission sought from all relevant authorities, selected respondents who gave their full consent to participate in the study were recruited. Prior to this, they were duly informed about the general nature and purpose of the study and their right to withdraw at any time without prejudice to their present or future employment. Respondents' level of knowledge of HIV/AIDS was computed by judging their answers to the causes, modes of transmission and prevention of HIV/AIDS. A mark was awarded for every correct response to a set of questions and no mark was awarded for incorrect responses. The total mark obtainable was sixteen and the levels of knowledge based on the highest scores attainable were as follows: 0–9 = poor knowledge; 10–12 = fair knowledge; and 13–16 = good knowledge. Similarly, respondents' attitude to PLWA was also assessed quantitatively judging from the proportion of `yes' responses to individual questions asked on how they would react, relate or treat PLWAs. These responses were computed individually. Sampling From a comprehensive list of government-owned health facilities in the Lagos metropolis, fifteen health facilities were randomly selected by simple balloting. From each selected health facility, a list of names of nurses and laboratory technologists was obtained from the respective medical directors. From the list, respondents were selected by stratified sampling method using a ratio of two laboratory technologists to three trained nurses. A maximum of 20 health workers comprising thirteen nurses and seven laboratory technologists were recruited from each health facility. To ensure anonymity and confidentiality, respondents in each health facility were requested to drop their completed questionnaires devoid of personal identities into sealed boxes provided by the study team. The questionnaires were administered and collected in the boxes provided by the principal investigator assisted by four experienced and trained interviewers. Two hundred and fifty four questionnaires (84.6%) were returned at the end of the data collection exercise. Data obtained were crosschecked for consistency and analysed using the statistical analysis software (SAS Institute Inc, Cary, NC). RESULTS Two hundred and fifty four health workers comprising one hundred and four (40.9%) laboratory technologists and one hundred and fifty nurses (59.1%) were surveyed. There was a disproportionate sex distribution of 181 (71.3%) females and 73 (28.7%) males. Many (56.7%) of them were aged between 30 and 39 years with a mean age of 36.0 years (SD 6.42). Less than half of the respondents had practiced for 10–15 years with an average duration of 10.4 years (SD 5.64). Over three quarters of the respondents were Christians and the majority of them had been sponsored by their health facilities to attend at least one refresher course on HIV/AIDS. Levels of Knowledge of HIV/AIDS Two hundred and forty respondents (94.5%) claimed that they had seen at least one case of AIDS. Based on a total of 16 marks, one hundred respondents (39.4%) had very good knowledge, one hundred and forty five (57.1%) had fair knowledge, while only nine (3.5%) had poor knowledge. A high level of knowledge of HIV/AIDS was displayed by respondents who had higher level of formal education compared to those with lower levels (p = 0.016). The longer the length of practice, the higher the level of knowledge (p = 0.0003); more males (40.6%) than females (37.5%) had excellent scores on knowledge (p = 0.009); and attending a refresher course on HIV/AIDS was associated with a higher level of knowledge (p = 0.01). In contrast, age, occupation and religion did not significantly influence the level of knowledge of respondents (p > 0.05). Although the overall level of knowledge of the modes of transmission and methods of prevention was fair, there were some deficiencies and misconceptions. (Table 1) Causes and Modes of Transmission of HIV Over ninety five per cent of the respondents knew the causes of AIDS and correctly identified heterosexual intercourse, blood transfusion and sharp instruments as some modes of transmission of HIV. However, in addition to these, some respondents believed that HIV could also be transmitted through insect bites (15.7%), hugging or touching an infected person (9.4%), sharing the same toilet and cooking utensils with an infected person (9.4%), and by having skin contact with an infected person (27.1%). High Risk Target Population People who indulge in prostitution, homosexuality and multiple sexual partnering were correctly identified by over 90% of the respondents as groups of people at high risk of contracting HIV. However, an appreciable proportion (50%) of the respondents failed to identify commercial drivers, adolescents and drug addicts as other high risk groups. Likewise, the respondents had poor knowledge of the groups of people least likely to contract HIV. For example, 72.4% and 92.1% respectively of the respondents incorrectly identified patients in hospital and health care providers as groups also at high risk of contracting HIV/AIDS. Areas of Misconception Identified Some degree of homophobia was detected among the respondents. Over one third of the them felt that all homosexuals have AIDS. A large proportion of the respondents (82.7%) did not know that women are at increased risk of contracting or transmitting HIV during their menstrual period. A few of the respondents (18.1%) felt that AIDS is curable if treatment is commenced early. Although 94.5% of the respondents correctly identified blood as a vehicle of transmission of HIV, only 81.1% and 71.7% correctly identified vaginal and semen secretions respectively. Furthermore, 69.9%, 78.0% and 76.4% of the respondents respectively thought that HIV can be transmitted through saliva, tears and sweat. Attitudes of Respondents to People Living with HIV/AIDS Two hundred and thirty eight respondents (93.7%) believed that HIV/AIDS is a serious threat to health workers and 87% believed that treating PLWA puts them at increased risk of contracting HIV. Many of the respondents (79.5%) believed that an HIV infected person poses a great danger to others, 34.7% felt that HIV infected persons should be isolated, over half (55.9%) felt that AIDS patients are responsible for their illness, and 90 (34.4%) felt that they deserve the consequences of their reckless life as a form of punishment from God. Many (89.8%), however, felt that they do not deserve to die. Majority (94.5%) felt that they deserve to be treated with empathy and understanding and given the best medical care possible. (Table 2) Whilst many of the respondents felt that persons with AIDS should be allowed to live their normal lives, i.e., to continue working or schooling, 44 (17.3%) believed that they should be relieved of their jobs and 50 (19.7%) recommended that students infected with AIDS should be expelled from school. The majority of respondents (91.3%) claimed that they would retain their friendship with PLWAs, 154 (52.8%) expressed their willingness to work in the same office with an AIDS patient and only 46 (18.0%) said they would visit or encourage their children to visit an AIDS patient. Attitude of Health Workers towards Treatment of HIV/AIDS Patients Ninety three per cent of the respondents accepted that they are duty bound to treat all ill persons irrespective of their HIV status and agreed to treat persons known to be infected with HIV/AIDS. A lower percentage (87.4%) agreed to examine or touch them. Most of the respondents (87.4%) advocated for the screening of all patients prior to admission into the wards particularly those admitted for surgical procedures, but only 108 (42.5%) would encourage the admission of PLWAs to the wards. Respondents' Level of Awareness of the Universal Precautions against HIV Two hundred and eight respondents (81.9%) were aware of and had read the universal precautions for health workers, while only 66 (26.0%) were aware of its existence at their workplaces. Only about half (52.4%) were privileged to attend a refresher course on HIV/AIDS, and when asked almost all the respondents expressed the desire to attend a refresher course on HIV/AIDS if given the opportunity. Attitudes of Health Workers to HIV Screening Only seventy respondents (28.0%) had been screened for HIV. Of these, 31.4% were screened prior to blood donation, 45.7% out of curiosity or for personal interests, 17.1% either on doctor's advice or for routine antenatal check, and 5.7% for travel requirements. Other respondents (72.0%) had never been screened because of fear (18.5%), high cost of the test(s) (9.8%), and a strong conviction that they will never be infected (71.7%). However, many of the respondents (83.5%) said they were willing to be tested if HIV screening is provided free of charge. All the respondents unanimously agreed that HIV screening should be made free for all health workers. More respondents aged 30–39 years (37.5%) had been screened for HIV when compared with 11.1% and 16.2% of those aged 20–29 years and above 40 years respectively (p = 0.0001). More male respondents (46.6%) had been screened for HIV compared to 20.3% of females (p = 0.0003). The longer the length of practice, the less likely it was for respondents to have been screened (p = 0.03). Also, 34.6% of the laboratory technologists were screened, compared to 23.3% of nurses although this difference was weakly statistically significant (p = 0.049). In contrast, the level of formal education and religion of respondents did not significantly influence whether or not they were screened for HIV (p > 0.05). DISCUSSION Until recently, HIV/AIDS control programmes in Nigeria had focused primarily on preventing the spread of HIV through behaviour modifications. However, with the growing number of PLWAs, there is increasing concern on the crucial role of the health care delivery system in providing wide range of care and support. This has become inevitable as almost every person living with HIV is bound to fall sick at one time or the other, thereby requiring medical care from health workers who are well trained and willing to provide such care. The study revealed that a significant proportion (96.5%) of the study subjects had appreciable (moderate to high scores) knowledge of the causes and prevention of HIV/AIDS. However, in spite of this, there existed many gaps in their knowledge of HIV and they had various misconceptions regarding how HIV/AIDS can be transmitted. In addition, a strong apprehension on how to handle the contagious nature of the disease was revealed. Most of the respondents (96.0%) knew the causative agent of AIDS to be a virus and the main modes of transmission to be sexual intercourse, blood transfusion, sharing sharp objects and perinatal transmission. However, there were also erroneous beliefs by the majority of the respondents that the HIV could be transmitted through insect bites (84.3%), touching and hugging (90.6%), sharing of toilet facilities with infected persons (90.6%), and poor levels of health and nutrition (92.9%). Okotie et al, in their study amongst civil servants, reported much lower figures of 36.8% and 37.9% on the sharing of utensils and casual kissing respectively as other modes of transmission.9,17 Epidemiological studies throughout the world have reported only three main modes of HIV transmission. One is through sexual intercourse with an infected person; second, through exposure to blood, blood products or transplanted organs or tissues; and third, from an infected mother to her fetus or infant before, during or shortly after birth.9,17-18 Casual contacts such as touching, hugging and kissing an infected person with HIV/AIDS do not result in HIV transmission.18 Respondents had varied knowledge of people at high risk of contracting HIV/AIDS. Whilst a significant proportion correctly identified prostitutes (100%), homosexuals (93.7%), people with multiple sexual partners (94.4%), only 64.6%, 44.4% and 45.2% of the respondents respectively correctly identified intravenous drug users, commercial drivers and adolescents as other high risk groups. In addition, many of them did not seem to know groups of people who are least likely to contract HIV/AIDS. For example, 92.1% and 72.4% of the respondents felt that health workers and in-patients are at very high risk of contracting HIV. Odujinrin et al reported much lower figures (51.5%) of health workers who identified homosexuals as a high risk group.19 Studies have suggested that the risk of nosocomial transmission of HIV is extremely low (0.3%) even after accidental parenteral inoculation.6,8,17,20-21 The incidence of HIV infection resulting from needle stick injury is a rare event with only 41 cases reported worldwide.9 Some degree of homophobia was displayed by the respondents. Ninety six of them (37.8%) felt that all homosexuals have AIDS. Homosexuality is not culturally accepted in Nigeria, as a result, it is not openly discussed or practiced. While societal rejection of certain social groups (e.g., homosexuals, injecting drug users and commercial sex workers) may predate HIV/AIDS, the disease has in many cases reinforced the stigma against them. In many societies, living with HIV/AIDS is often seen as a shameful thing. It is even made worse if the infection is perceived to be associated with some minority groups or sexual behaviours. Studies have shown that homophobia accounts for a significant level of variation in the expressed attitude towards the willingness of health workers to treat heterosexual and homosexual AIDS patients.22-25 It is important that the curricular of prospective health workers in the medical, nursing and paramedical institutions be incorporated with educational programmes on HIV/AIDS to encourage more open discussions and positive attitudes towards homosexuality and other forms of sex. Identified gaps in knowledge include the misconception that AIDS could be cured if treated early. Only 44 women (17.3%) knew that the risk of contracting HIV is higher during menstruation. Similarly, respondents demonstrated poor knowledge of the sources of HIV. Besides blood, vaginal secretions and semen, over one fifth of the respondents also mentioned saliva, tears and sweat as other sources of HIV. Although HIV has been isolated from most body fluids such as blood, semen, vaginal secretions, saliva, tears, urine, breast milk, cerebrospinal and amniotic fluids, only blood, blood products, semen, vaginal secretions, donor organs/tissues and breast milk have been implicated in the transmission of its infection.20,21 Saliva, for instance, is known to be a hostile body fluid for HIV, which quickly inactivates the virus.9 There is also good evidence that HIV is not transmitted through close skin contact even over prolonged periods.20,21 Over three quarters of respondents (93.7%) in this study considered HIV as a threat to health workers. They believe that caring for PLWAs puts them at increased risk of contracting HIV infection. Factors that have been implicated to be strongly associated with the unwillingness of health care providers to treat AIDS patients besides homophobic attitudes23 include the fear of losing other patients patronising their hospital if information spreads that HIV/AIDS patients are being treated there.26 The fear of contracting HIV through accidental inoculation of infected blood has assumed alarming proportions, affecting not only the career choices of young people and discriminatory practices towards PLWAs, but it has also compromised the quality of care provided for them. Lack of confidence of health workers arising from the lack of knowledge and skills to provide AIDS counselling and advice has been identified as another factor that can explain the negative attitudes exhibited.9,27,28 It is important to provide opportunities during HIV training courses for prospective health workers to freely express their feelings without perceiving that they will be judged. HIV/AIDS is sometimes seen either as the result of personal irresponsibility or is linked to sexual perversion and is seen as a punishment for those infected.15 In this study, more than half of the respondents felt that persons infected with HIV/AIDS are responsible for their illness, hence, 34.4%, made up of 48 nurses (32.0%) and 12 laboratory technologists (11.5%) (p < 0.0001) thought that they deserve the punishment that befell them. Religion did not significantly influence how respondents viewed HIV/AIDS patients (p > 0.05). Klonoff et al similarly reported that nurses viewed PLWAs as deserving their illness in much the same way as they viewed non-compliant diabetic and renal patients.29 Factors that have been found to contribute to HIV/AIDS-related stigma include the fact that HIV/AIDS is a life-threatening disease; it is associated with behaviours such as homosexuality and injecting drug users. People living with HIV/AIDS are often thought to be responsible for becoming infected, and religious and moral beliefs that having HIV/AIDS is the result of moral fault such as promiscuity or deviant sexual behaviours that deserve to be punished.7,15,16 Despite the fact that most of the respondents in this study (92.9%) admitted to having a moral obligation as health workers to treat HIV/AIDS patients, only 42.5% would encourage their admission on the wards, and where admission of the patient is inevitable they recommended that all such patients, particularly those for surgery, be screened for HIV before admission. Attitudes of respondents to PLWAs were generally poor. Two hundred and two respondents (79.5%) thought that PLWAs are dangerous to others and should therefore be isolated. These findings compare favourably with reports from within and outside Nigeria.30,31 Although the majority of the respondents were willing to treat HIV/AIDS patients, their reluctance to have any direct contact with them could be explained by the fear of contagion indirectly expressed by their concerns and prejudicial attitudes towards AIDS patients. The study has also found that a few of the respondents exhibited discriminatory attitudes towards HIV patients. For example, 44 (17.3%) respondents said PLWAs should be laid off their jobs while 50 (19.7%) said they should be expelled from school. The WHO/ILO guidelines on HIV/AIDS at the workplace stipulate that HIV is not and should not be a cause for termination of employment.21,32 Discriminating against individuals with HIV, particularly the high risk group, tends to marginalise infected people, thus making them to become far more difficult to reach and work with. This will in turn make any intervention or prevention initiatives harder to introduce and sustain.33 Under the numerous international agreements and accords, societies are under obligation to provide equal protection and equal access to a broad range of services and benefits that are necessary for individual well being irrespective of their HIV status.34 Only 70 respondents (28.0%) had been screened for HIV. The reasons given by the remaining respondents for not being screened included fear of the unknown (18.5%), unaffordable cost (9.8%) and the feeling that they are not likely to contract HIV ( 70%). The benefits of HIV testing cannot be over-emphasised although it has drawn a lot of controversies resulting in some activists totally condemning it for fear of discrimination and victimisation.7 In the current phase of the HIV epidemic in Nigeria, it is essential for certain conditions to be in place if voluntary HIV screening is to be accepted by all. First, the screening tests must be affordable and even made free for the vulnerable groups, i.e., young persons, pregnant women, children and people suffering from chronic illnesses. Second, antiretroviral drugs should be readily available at affordable prices and widely distributed to persons found to be HIV positive. Third, adequate pre and post-test counselling should be provided by skilled counsellors and confidentiality maintained. Combating the stigma and discrimination against people who are infected with HIV/AIDS is as important as developing medical cures in the process of preventing and controlling the global epidemic. Substantial progress can be made in overcoming stigma and discrimination against PLWAs through the legal process. Unfortunately, PLWAs lack knowledge of their rights in the society. They need to be educated to make them better able to challenge the discriminating stigma and denial they encounter in the society. People living with HIV/AIDS also have much to give by being involved in the response to HIV. By involving them in the design and implementation of projects to combat HIV/AIDS, the impact of how the society views them can be vastly reduced. Institutional and other monitoring mechanisms can enforce the rights of people living with HIV/AIDS and provide powerful means of mitigating the worst effects of discrimination and stigma. Political leaders have a clear responsibility to create a society that is free of stigma by speaking out without hindrance about AIDS in their countries and by creating an enabling environment that will make the society see people with HIV/AIDS as part of it. Health care workers, including doctors, nurses, paramedical personnel and traditional healers, have a very important role to play in reducing HIV/AIDS-related stigma. Negative attitudes and lack of understanding are real issues contributing to stigma from health workers. In their unique positions, health care providers have a responsibility to provide quality care and services without stigmatising and without being judgmental. It is, therefore, pertinent that all health care providers have access to up-to-date information on all aspects of HIV/AIDS, i.e., its modes of transmission, prevention, counselling and guidelines for safe practice. They should be competent to provide care and counselling to patients, know the universal precautions and accept caring for people living with HIV/AIDS as their ethical and moral duty. A safe environment should be secured for all health care providers including the provision of protective equipment and materials that will shield them from exposure to HIV and other blood-borne diseases such as hepatitis B and C. CONCLUSION In view of the current unchecked status of the HIV/AIDS pandemic and the fact that there is yet no known cure or vaccine for it, it is critical that health care providers improve their quality of care for PLWAs. Health care providers as health educators should play a dominant role in safeguarding the health of the community by encouraging the rehabilitation and integration of people already infected with the virus within the context of their families and the society as well as preventing the transmission of HIV. To facilitate this, the curricula of various training institutions should incorporate both cognitive and affective programmes that will expand the scope of prospective health workers, improve their level of awareness of HIV/AIDS and encourage the development of more open and positive attitudes towards PLWAs. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03013t2.jpg] [rh03013t1.jpg] |
| |||||||||

{kind=link}
{kind=link}