 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 13-19 Dual Protection against Sexually Transmitted Infections and Pregnancy in South Africa Chelsea Morroni1,2,3, Jennifer Smit2,4, Lynn McFadyen2,5, Mmabatho Mqhayi2,5 and Mags Beksinska4 1Women's Health Research Unit, University of Cape Town, Cape
Town. 2Africa Centre for Population Studies and Reproductive Health,
Hlabisa, KZN. 3Fogarty AITRP, Department of Epidemiology, Mailman
School of Public Health, Co lumbia University, New York, USA. 4Reproductive
Health Research Unit, Department of Obstetrics and Gynaecology, University
of the Witwatersrand, Durban. 5Clinical Sciences, Pfizer, Global
Research and Development, Sandwich, UK. 6Reproductive Health Research
Unit, Department of Obstetrics and Gynaecology, University of the Witwatersrand,
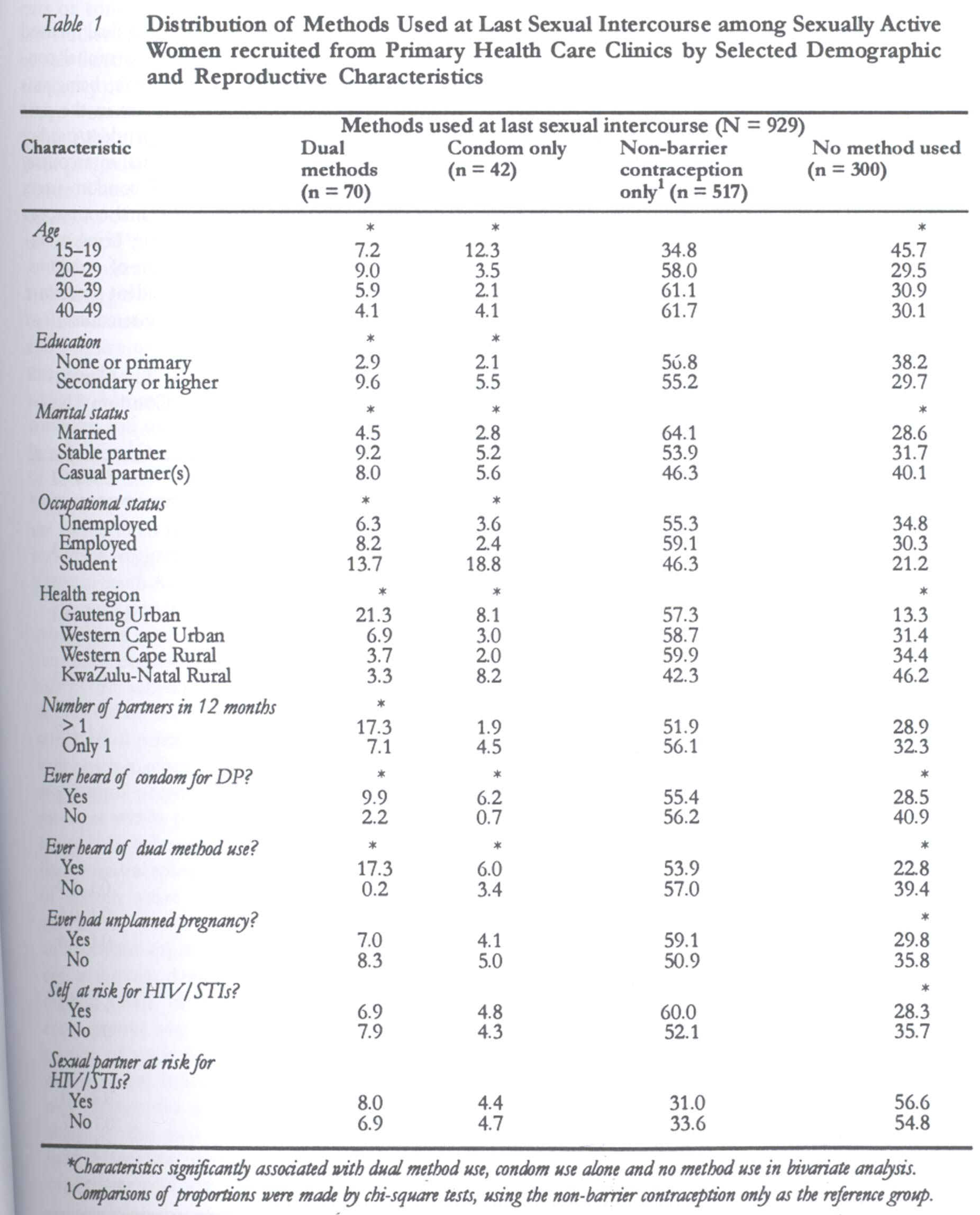
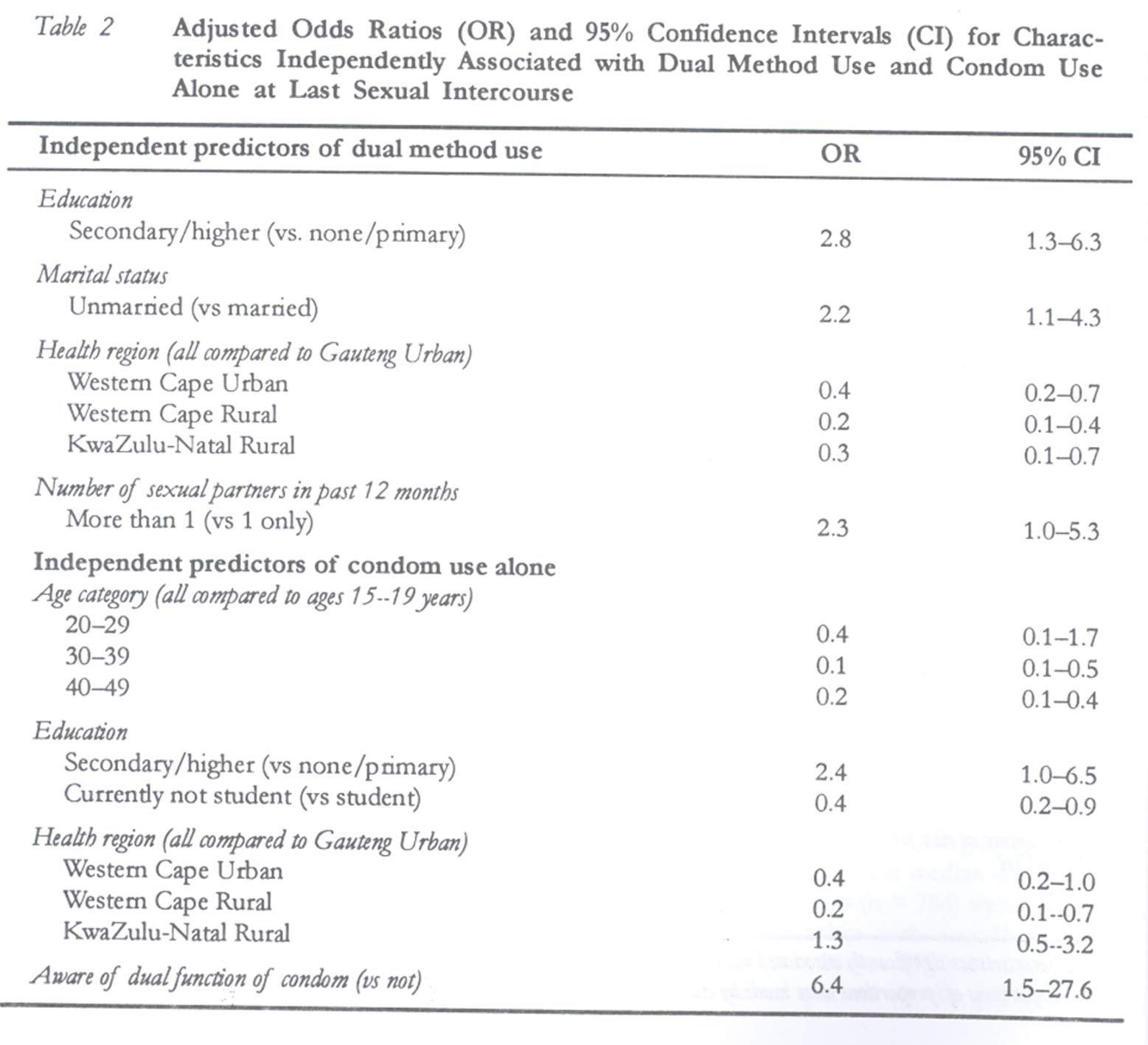
Johannesburg Code Number: rh03018 ABSTRACT Promotion of simultaneous protection against sexually transmitted infections (STIs) and unintended pregnancy, referred to as dual protection, represents an important public health intervention. We investigated its prevalence and correlates in South Africa. A cross-sectional survey of 929 sexually active women, aged 15-49 years, was conducted in 89 public primary health care clinics, with dual method use and use of condom alone at last sexual intercourse as outcomes. At last intercourse, 12% of women were protected from both STIs and pregnancy. In multivariate analysis, higher education, being unmarried, and multiple sex partnership in the past year were predictors of dual method use, while younger age, higher education and awareness of the dual function of condoms were predictors of condom use alone. Dual protection is low in this population. The predominance of hormonal contraceptive use in South Africa means that increasing barrier method use among hormonal contraceptive users is an important strategy for increasing dual protection. (Afr J Reprod Health 2003; 7[2]: 13-19) RÉSUMÉ Double protection contre les infections sexuellement transmissibles et contre la grossesse en Afrique du Sud. La promotion de la protection simultanée contre les infectons sexuellement transmissibles (IST) et contre la gossesse non-voulue, qu'on appelle la double protection, représente une intervention importante de la santé publique. Nous avons étudié sa prévalence et ses corrélats en Afrique du Sud. Nous avons mené une enquête tranversale auprès des 929 femmes sexuellement actives, âgées de 15 à 49 ans, auprès de 89 cliniques de santé primaire publiques, à l'aide de la méthode à double fonction et de l'utilisation unique des préservatifs au cours du dernier rapport sexuel, comme des issues. Au cours du dernier rapport sexuel, 12% des femmes ont été protégées contre à la fois les IST et la grossesse. A travers une analyse multivariée, nous avons trouvé que l'étude supérieure, le fait d'être célibataire et d'avoir plusieurs partenaires au cours de l'année passée, ont été des indices de l'emploi de la méthode à double fonction alors que le fait d'être encore plus jeune, d'avoir acquis une scolarité supérieure et la conscience par rapport à la double fonction des préservatifs, ont été des indices de l'utilisation des préservatifs seulement. L'emploi de la double protection est faible dans cette population. La prédominance de l'utilisation des contraceptifs hormonaux en Afrique du Sud signifie que l'emploi croissant de la méthode des barrières chez les usagers du contraceptif hormonal constitue une stratégie importante pour l'augmentation de la double protection. (Rev Afr Santé Reprod 2003; 7[2]: 13-19) KEY WORDS : Dual protection, contraception, sexually transmitted infections, condoms, South Africa INTRODUCTION South Africa is faced with growing epidemics of HIV, other sexually transmitted infections (STIs) and unintended pregnancy. There has been a dramatic increase in HIV infection, with seroprevalence among antenatal attenders increasing from less than 1% in 1990 to almost 25% in 2001.1 Other STIs also contribute significantly to morbidity and mortality2 and have particularly serious long-term health consequences for women.3,4 At the same time, there are high rates of teenage pregnancy, with 35% of South African women having been pregnant by 19 years of age,5 and evidence to suggest that up to 53% of South African pregnancies are either unplanned (36%) or unwanted (17%).5,6 In this context, the promotion of dual protection, defined as simultaneous prophylaxis against STI and unintended conception, is an increasingly important public health intervention.7 Despite the recognition of dual protection as a critical strategy in reproductive health policy,8 there are few data available on dual protection and dual method use in South Africa. As part of a national study of contraceptive practices,9 we investigated the knowledge, prevalence, and demographic and behavioural correlates of dual protection, with a particular focus on dual method use among women attending public primary health care clinics across the country. METHODS Data were collected as part of a cross-sectional study conducted between November 1999 and August 2000.9 Participants were recruited from 89 public sector primary health care facilities sampled from four health catchment areas in three provinces across the country. Participants were interviewed at all primary health care facilities in a deep rural area (n = 14) in the province of KwaZulu-Natal and at 17 purposively selected health facilities in an urban area of Gauteng Province. A random sample, weighted according to patient load, of 30 Western Cape Province health facilities in an urban region and 28 in a rural region were also selected. The larger provincially representative sample was selected in this province in response to a request by the Western Cape health authority for health planning purposes. South Africa is diverse in terms of language, culture, access to health and educational services, and urbanisation; we chose health regions to reflect this diversity. At each facility, at least 10 women (maximum of 18) between the ages of 15 and 49 years attending the clinic for any reason (including accompanying another) were consecutively selected over a period of one to two days. They were interviewed prior to or after their consultation using a structured questionnaire. Consent was obtained from each participant and no incentive was offered for participating. Data were analysed using SPSS 9.0. The analysis included only women who reported sexual intercourse in the twelve months prior to the interview (n = 929, 87% of the 1068 women surveyed). Participants were grouped according to the methods they and/or their partner used during their most recent act of sexual intercourse: (1) dual method use (male or female condom plus non-barrier contraception); (2) condom use alone (male or female condom); (3) non-barrier contraception use alone (such as hormonal contraceptives, sterilization, or an IUD); and (4) no method use. The main outcomes were dual method use at last intercourse and use of a condom alone at last intercourse. Women who used non-barrier contraception alone at last intercourse formed the reference category for these analyses. We chose last sexual intercourse as the reference period because self-reports of method use of last intercourse are less susceptible to recall errors than are reports of previous intercourse events due to relative recency. Also, research in South African populations suggests that condom use at last intercourse is a reasonable proxy for consistent condom use.10 The characteristics associated with dual method use and/or condom use alone in bivariate analysis (p < 0.1) were entered into separate logistic regression models to identify the independent predictors of each outcome. FINDINGS Among the 929 participants reporting sexual intercourse in the previous year, the median age was 25 years, and 83% of subjects (n = 766) were married or in a stable relationship with a male partner. Most participants (n = 866 or 93%) reported having only one sexual partner in the previous 12 months; 57% (n = 530) reported at least one unplanned pregnancy and 49% (n = 452) reported becoming pregnant before age 20. Forty five per cent (n = 420) described themselves as being at risk of acquiring HIV or other STIs. Almost all participants had heard of male condom (n = 900 or 97%) and 28% (n = 282) had ever used a male condom. Seventy per cent of participants (n = 648) were aware that a condom alone could be used to prevent both pregnancy and infection, but fewer respondents (n = 399 or 43%) were aware that a condom could be used with another effective contraceptive method to achieve dual protection. Table 1 describes respondents' demographic and reproductive health characteristics by methods used at last sexual intercourse. One hundred and twelve subjects (12%) were protected from both pregnancy and STIs the last time they had sexual intercourse, with 70 (7.5%) using dual methods and 42 (4.5%) using a condom alone. Five hundred and seventeen women (56%) were protected from pregnancy only through the use of a non-barrier contraceptive, while approximately one third of respondents (n = 300) used no method at all. In multivariate analysis comparing dual method users with women who used only hormonal contraception (Table 2), higher education, being unmarried, having multiple sex partners in the past year, and health region were independent predictors of dual method use at last sexual intercourse. In the multivariate comparison of condom users with women who used only hormonal contraception, younger age, higher education, being a student, awareness of the dual function of condoms, and the health region were independent predictors of condom use alone at last sexual intercourse. DISCUSSION While most previous dual protection research studies have focused exclusively on family planning clients or condom procurers,11,12 this is one of the few studies focusing on a general clinic population in sub-Saharan Africa. Our data suggest that the frequency of dual protection is low among sexually active women attending public health facilities in South Africa, with 12% of women protected from both pregnancy and infection at last sexual intercourse. These findings are broadly consistent with the results of other studies conducted in sub-Saharan Africa.11,12 This survey was conducted among individuals attending public health facilities, with access to health education and condoms. Thus, awareness and practice of dual protection may be higher in this sample compared to the general population. In addition, like most studies investigating the use of condoms and other contraceptives, this study may be subject to biases associated with the over-reporting of method use.13 Both of these factors could lead these results to overestimate the levels of dual method use and condom use at last sexual intercourse in this population, suggesting that the frequency of dual protection in South Africa may be even lower. Seventy per cent of subjects in our study were aware that a condom could be used alone to prevent both pregnancy and infection, and less than half of the subjects (43%) were aware that a condom could be used with another contraceptive to achieve dual protection. Greater awareness of the various approaches to dual protection, through integration of pregnancy and HIV/STIs prevention messages within primary health promotion, is required.14 In light of the high prevalence of non-barrier contraceptive use in South Africa, with 59% of sexually active 15-49-year-olds reporting current use of a non-barrier contraceptive method,5 an important approach to promoting dual protection is through dual method use: adding a barrier method (male or female condom) to existing contraceptive use. That a somewhat greater proportion of study participants used dual methods at last sexual intercourse than only a condom may support the greater feasibility and acceptability of the dual method approach from the user perspective. Alternatively, the greater level of dual method use may reflect provider reluctance to promote the condom alone, due to its lower contraceptive efficacy compared to hormonal methods, or provider reluctance to move established hormonal method user s to a less effective birth control method, such as a barrier method.15-17 Health promotion messages and counselling for dual method use, which are different from condom promotion messages,18 are urgently needed in this population. Our data suggest that the characteristics of dual method users and users of condoms alone differ in some respects. While higher education was a predictor of both dual method use and condom use alone at last sexual intercourse, we found that younger women were more likely to use condoms alone. Thus, the promotion of condoms alone for dual protection may be more appropriate among teenagers, who are initiating contraceptive behaviours, whereas the promotion of dual method use may be more appropriate for women with established use of hormonal contraception. The dual function of the condom as both a contraceptive and means of HIV/STIs prevention needs to be better promoted,19,20 as women in our study who were aware of the dual function of condoms were over six times more likely to have used a condom at last sexual intercourse than women who were not. This promotion should include the role of emergency contraception as a "back-up" contraceptive method in case of condom failure.9,21 Despite having identified basic gaps in knowledge about dual protection strategies and the characteristics of women who do and do not practice dual protection i n this study, our finding that perceived self and partner risk for HIV/STIs was not associated with dual protection underscores the existence of obstacles to barrier method use that extend beyond a woman's knowledge of her risk and her personal risk assessment.22 In addition, we found that nearly one third of women surveyed (n = 300 or 32%) were not protected from pregnancy or STIs at last sexual intercourse. Given that these women were sexually active and were accessing primary health care services, this finding is worrisome. This finding, which is consistent with general South African contraceptive prevalence data,5 indicates a substantial unmet need for pregnancy and STIs prevention even among health service attenders. This cross-sectional study provides preliminary insights into the prevalence and correlates of dual method use and dual protection among South African women. The interpretation of these findings may be limited by the focus on method use at last sexual intercourse only. Prospective studies that can capture patterns of method use over time are required to assess more fully women's risk of and protection against STIs and unwanted pregnancy. Such information will aid South Africa policymakers and health workers in understanding dual protection and ultimately increasing its practice. ACKNOWLEDGEMENTS This research was supported by a grant from the Wellcome Trust (050522/Z/97/Z). Permission to conduct the study was obtained from the relevant authorities in provincial and district departments of health, and ethical approval for the study was provided by the Universities of Durban-Westville, Witwatersrand and Cape Town. We are grateful to our fieldworkers, our data capturers, the study participants and the health service personnel who accommodated this research. Landon Myer and Alfredo Morabia provided valuable comments on previous drafts of this paper. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03018t2.jpg] [rh03018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}