 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
African Journal of Reproductive Health, Vol. 7, No. 2, Aug, 2003 pp. 20-24 The Norplant Experience in Zaria: A Ten-Year Review DNP Haggai Correspondence: Dr Deborah Haggai, Department of Obstetrics and Gynaecology, Ahmadu Bello University Teaching Hospital, Zaria, Kaduna State, Nigeria. E-mail: dhaggai@hotmail.com Code Number: rh03019 ABSTRACT Norplant is an effective, long-acting, reversible, progestin-only contraceptive that provides protection for up to five years. The aim of this review is to ascertain the response of family planning clients in Zaria to Norplant. In Nigeria, Family Health International started pre-introductory clinical research on Norplant in 1985 at five sites including Zaria. Since the conclusion of the study, Norplant services have been maintained, but no attempt has been made to report the response of this largely Hausa and Muslim community where contraceptive use is generally low. It is important to determine whether the advantages of Norplant have had an impact on this setting. The study showed that most of the clients were satisfied with the method. There was a progressive increase in the number of women using Norplant by 1995, with a significant decrease in the number of women undergoing sterilisation. Acceptability of Norplant is on the increase, thus, it should be easily available, accessible and affordable. (Afr J Reprod Health 2003; 7[2]: 20-24) RÉSUMÉ Expérience de Norplant à Zaria: compte rendu couvrant une période de dix ans. Norplant est un contraceptif à action prolongée, réversible, teneur uniquement en progestérone, qui donne la protection d'une durée de jusqu'à cinq ans. Cette étude a pour but de déterminer la réponse à Norplant de la part des clientes de la planification familiale à Zaria. Au Nigéria, la Family Health International a commencé la recherche clinique de pre-introduction sur Norplant en 1985 dans cinq lieux y compris Zaria. Depuis la fin de l'étude, les services Norplant ont été retenus, mais aucun effort n'a été fait pour signaler la réponse de cette communauté, en majorité haoussa et musulanes où l'utilisation des contraceptifs est, en général, base. Il est nécessaire de déterminer si les avantages de Norplant ont eu un impact quelconque sur le milieu. L'étude a montré que la plupart des clientes ont été contentes de la méthode. Il y a eu une augumentation progressive par rapport au nombre des femmes qui utilisaient Norplant en 1995 alors qu'il y a eu une baisse considérable par rapport au nombre des femmes qui subissaient la stérilisation. Puisque l'acceptation de Norplant s'accroît, il faut qu'il soit disponible, à la portée de tous et qu'il soit abordable. (Rev Afr Santé Reprod 2003; 7[2]: 20-24) KEY WORDS : Norplant, Family Health International, family planning, contraceptive, Zaria, Nigeria INTRODUCTION Continued effort to produce an ideal contraceptive method for the human race has led to the variety of contraceptive methods available today. An ideal contraceptive should provide full client satisfaction, be 100% effective, must be safe, should be reversible, and without side effects or residual effects after use. It is unfortunate that there is no single contraceptive that has fulfilled all these criteria. The search over the years has led to the development of Norplant contraceptive implants. Norplant is an effective long-acting, reversible progestogen-only contraceptive that provides protection for up to five years.1-7 Its development began in the laboratories of the Population Council's Centre for Biomedical Research in 1966. The first clinical studies began in Chile in 1974. In 1975, a multinational phase III trial was initiated in six countries, namely, Brazil, Chile, Denmark, Dominican Republic, Finland and Jamaica. The pre-introduction clinical trials began in eight countries between 1980 and 1982 and these continued to spread to more countries over the years. Globally, Norplant acceptance is on the increase. Indonesia has the largest population of Norplant users. Other countries with significant use include Sweden, Thailand, Finland and Columbia. There are more than 46 countries now using the contraceptive. The Family Health International (FHI) has reported continuation rate of 84.8% after one year. Rationale for the Study In Nigeria, FHI started pre-introductory clinical research on Norplant in October 1985 at five sites in Nigerian teaching hospitals located in Ibadan, Zaria, Benin City, Ilorin and Jos. Continuation rates of 90.1, 84.9 and 77.4 per 100 women at one, two and three years respectively were reported in the centres.8,9 Since the conclusion of the FHI study in Zaria, Norplant services have been maintained, but no attempt has yet been made to report the response of this largely Hausa and Muslim community. It is well known that in general contraceptive use is low in such communities10 and it is important to determine whether the advantages of Norplant have had an impact on this setting. In January 1989, the Association for Voluntary Surgical Contraception (AVSC) also supported Norplant services as part of operations research in five sites in Nigeria, different from the FHI sites. These were university teaching hospitals of Port Harcourt, Calabar, Maiduguri and Lagos, and the Ogun State Ministry of Health, Abeokuta. AIMS AND OBJECTIVES OF STUDY This study was carried out to ascertain the response of family planning clients in Zaria to Norplant within the context of general family planning services offered at the Ahmadu Bello University Teaching Hospital, Zaria. Its objectives are as follows:
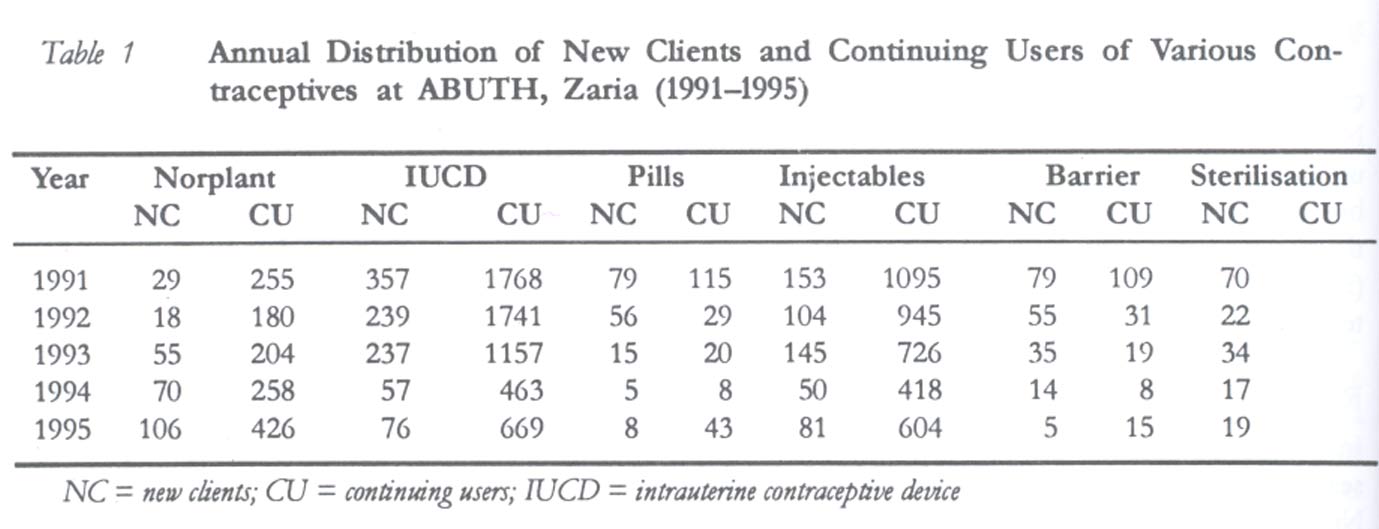
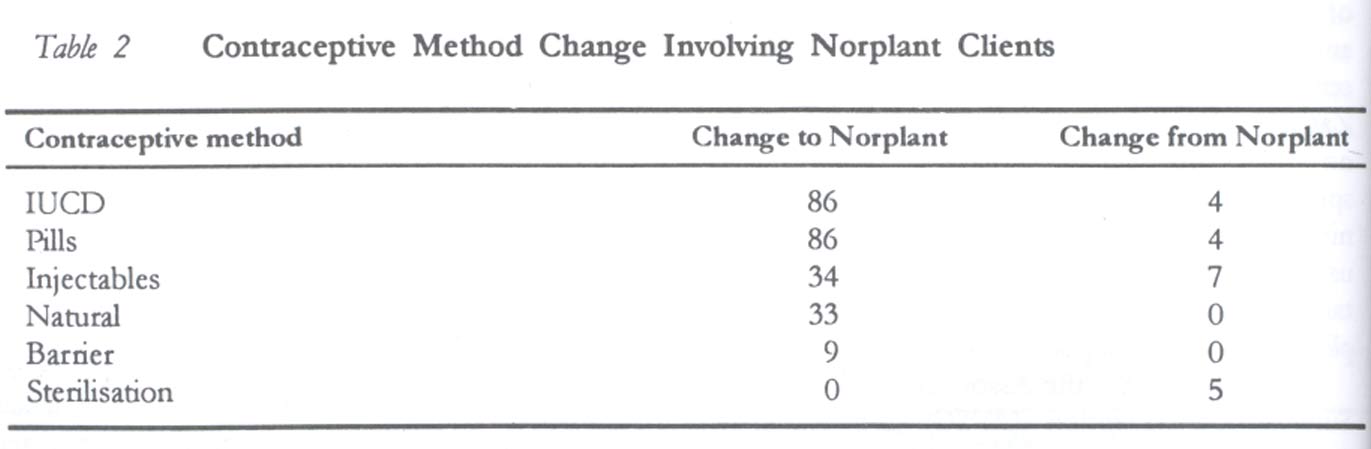
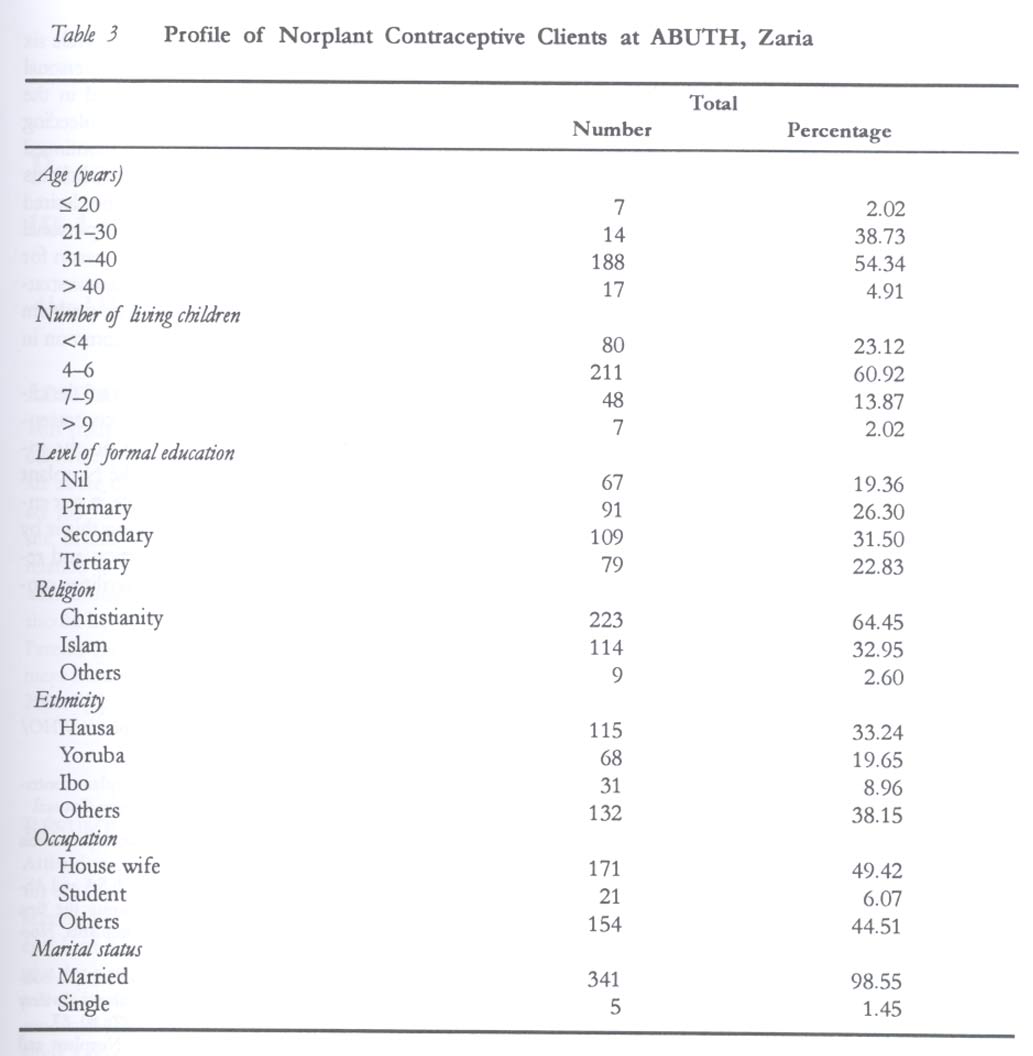
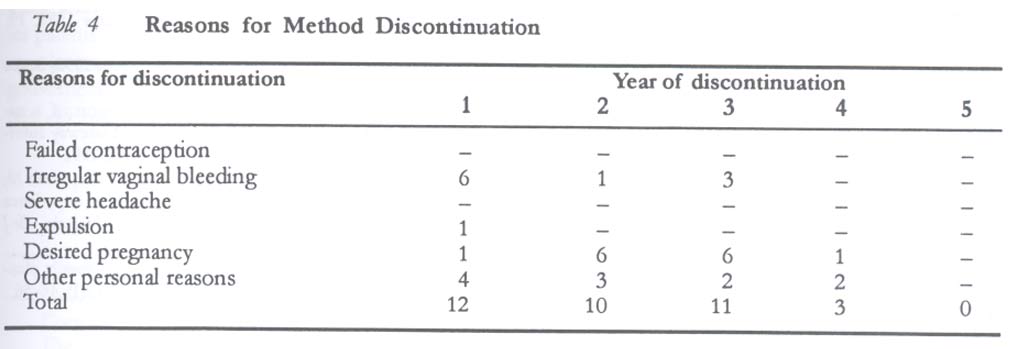
MATERIAL AND METHODS This review is a retrospective study of case files of clients who attended the family planning clinic of the Obstetrics and Gynaecology Department, Ahmadu Bello University Teaching Hospital, Zaria, from January 1, 1991 to December 31, 1995. The family planning clinic operated from 2.00 p.m. to 5.00 p.m. daily on working days until July 1995 when services were provided from 7.00 a.m. to 9.00 p.m. daily, Monday through Saturday. This clinic is run by trained family planning service providers and doctors of the Obstetrics and Gynaecology Department. A doctor is usually posted to the clinic to attend to cases and manage complications that may be associated with the various methods. The various methods available at the centre include intrauterine contraceptive device, oral contraceptives, Norplant, injectables, barrier methods and sterilisation. Norplant services are provided by doctors and nurses trained in its insertion and removal. Both married and single women were offered Norplant including lactating mothers. Written spousal consent was obtained from all married women before including them in the study. During the period of the study all clients were provided with general counselling on all contraceptive methods available at the clinic including details of side effects and complications. They were given opportunity to ask questions on the various methods. Those who accepted Norplant implants were individually counselled to ensure that they understood the risks and benefits as well as side effects that may be associated with its use. All women with absolute contraindications to Norplant use, such as acute liver disease or jaundice, undiagnosed vaginal bleeding, breast cancer, coronary artery or cerebrovascular disease or severe hypertension, and women who expressed major concerns regarding tolerance of side effects, were offered alternative method of birth control. Pregnancy was also considered an absolute contraindication. Prior to insertion of the implants, general physical and pelvic examinations were carried out on each woman. The first follow-up visit was after four weeks. After this the women came for follow-up at the third, sixth and twelfth months, and subsequently yearly until the implants were removed or renewed. The clients were advised to return to the clinic if symptoms developed at any time regardless of their scheduled follow-up visit. At each follow-up visit, clients' satisfaction was ascertained and any complaints or complications managed and recorded in the client's record form. Routine records of weight and blood pressure were also made at each visit. Reasons for implant removal included completion of five years, accidental pregnancy, menstrual disorders, planned pregnancy, medical and other personal reasons. Renewal of insertion was done for clients who wanted it immediately after removal. RESULTS The total number of clients who benefited from the various methods of contraception available during the period is shown in Table 1. A total of 346 case files of Norplant users were available for analysis. DISCUSSION The most popular methods of contraception used in 1991 in this setting were IUCD and injectables, while the least used was the Norplant implant (Table 1). By 1995, Norplant had gained popularity as demonstrated by a progressive increase in number of women using Norplant over the years under review. A significant decrease in the number of women undergoing sterilisation was also recorded. Barrier methods and the pills are still not commonly utilised among our clients. Method change from one form of contraception to the other (Table 2) also demonstrates the acceptability of Norplant among our clients. There were more clients changing from other methods to Norplant than vice versa. Four clients changed to other methods because they wanted a shorter rest before conception after the five-year period of usage. Among the five clients who changed to sterilisation, two had total abdominal hysterectomy due to other medical reasons and came for removal of the implants. The demographic characteristics of users are shown in Table 3. Majority of the clients fell between ages 31 and 40 years and only a few were in the extremes of the reproductive life, that is, less than 20 years and more than 40 years. About 61% of clients had 4-6 living children and only 2% had more than nine living children. The level of formal education was low among our clients. Almost 99% of the women were married. Single ladies do not find it very comfortable to access contraception in our setting because they are looked upon as loose girls. The introduction of Norplant II might be the option for women who desire short period contraception. From the study, 339 out of 346 clients (98%) were satisfied with this method and would recommend it to others. This is similar to the figure of over 95% who would recommend it to a friend in other centres.7 Only 36 clients discontinued the method during the ten-year study, 12 within the first year of use, 10 in the second year, 11 in the third year and three in the fourth year (Table 4). Among those who discontinued in the first year, six were due to irregular vaginal bleeding, one was due to expulsion, one desired pregnancy because she lost her baby, while the other four had personal reasons ranging from marital disharmony to change of husband. In the second year, only one discontinued because of irregular vaginal bleeding while six desired pregnancy and three had other personal reasons. Among the 11 who discontinued in the third year, three had irregular vaginal bleeding while six desired pregnancy and two discontinued for personal reasons. There were only three clients who discontinued in the fourth year; one desired pregnancy and the other two had other personal reasons. Failed contraception was not a reason for discontinuation in any of the clients, demonstrating the effectiveness of the method. The problem of irregular vaginal bleeding was more common in the first year and thereafter reduced. In conclusion, it is evident that most of the clients were satisfied with this method of contraception and user rates in this setting are on the increase. It is therefore necessary to make Norplant easily available, accessible and affordable in our environment. The way forward in achieving this is by training more health workers on insertion and removal techniques so that more health facilities canoffer the services. REFERENCES
Copyright 2003 - Women's Health and Action Research Centre The following images related to this document are available:Photo images[rh03019t3.jpg] [rh03019t4.jpg] [rh03019t1.jpg] [rh03019t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}